
Abstract
Background
Cross-sectional and longitudinal studies show conflicting results regarding the association between cognition and life-space mobility, and little is known regarding the mediators and moderators of the association.
The aim of this study was to investigate the association between cognition and life-space mobility in older adults, as well as the intervening variables modifying the relationship.
Methods
Community-dwelling older adults aged 65 years and older (N = 1643) were assessed at three time points over a period of 2 years. Growth mixture models with mediation and moderation analysis were utilised to investigate association between cognitive function and life-space mobility. The potential mediators and moderators were depressive symptoms, locus of control, gait speed and grip strength. Analysis was controlled for age, sex, education, annual income, number of chronic illnesses, and living site.
Results
The direct association between initial scores of cognitive function and life-space was mediated by initial scores of depressive symptoms and gait speed, and moderated by initial scores of grip strength. No direct association between change in cognitive function and change in life-space mobility was found; the scores were mediated by change in depressive symptoms.
Conclusions
We conclude that the relationship between change in cognitive function and life-space mobility in older adults is not well-defined over an observation period of 2 years.
Similar content being viewed by others
Background
The concept of life-space mobility is receiving growing attention in the field of aging. It defines a spectrum of geographic areas that extend from domicile to distant destinations [1]. Constricted life-space mobility has been associated with adverse health outcome, including illness, poor self-rated health, difficulty in basic and instrumental activities of daily living, [1] depressive symptoms, [1, 2] frailty, and death [2].
Webber and colleagues have presented a comprehensive framework illustrating variables associated with life-space mobility [3] (Webber framework). Five categories of determinants of life-space mobility were hypothesized: (i) cognitive determinants are relevant for reaching distant destinations; (ii) psychosocial determinants affects the motivation to be mobile; (iii) physical performance reflects the influence of strength and balance; (iv) environmental context reflects the influence of the built environment; and (v) financial resources, which influences activities, access to mobility aids and modes of transportation. According to the Webber framework, all categories of determinants are influenced by age, culture, and personal life history.
The association between cognition and life-space mobility has been investigated in the literature, but the direction of the relationship remains unsettled. Although mobility may stimulate cognition, high levels of cognitive function may be a prerequisite for being mobile. Mobility is a complex activity requiring high levels of physical and cognitive function, especially when venturing beyond one’s domicile [4]. A decline in higher-order cognitive abilities might be followed by a decline in the more complex aspects of life-space mobility, such as driving [5]. Older adults can also adjust their mobility behavior in a way that reflects their cognitive skills [6].
Empirically, cross-sectional studies have reported significant association between higher cognition and an expansive life-space, [2, 7,8,9,10] although discrepant findings were reported [11,12,13]. To our knowledge, three longitudinal studies have investigated whether baseline cognitive function was associated with future life-space mobility, all with mixed results [14,15,16].
Determinants may influence each other and interact to shape mobility, as suggested in the Webber framework. This opens the possibility that intervening variables mediate or moderate [17] the association between cognition and life-space mobility. Studies have shown that psychosocial determinants (depression or locus of control) and physical determinants (grip strength or walking speed) are related to cognition [9, 18,19,20] and to life-space mobility [1, 2, 8, 9, 11]. These determinants are legitimate, intervening variables in change in both cognition and mobility. However, with few exceptions, [9] the role of psychosocial and physical determinants as mediators or moderators in the association between cognition and life-space mobility has not been investigated.
Using the Webber framework, the current study examines the association between cognition and life-space mobility in community-dwelling older adults. It also focusses on the role of depressive symptoms and locus of control as psychosocial determinants, and the role of gait speed and grip strength as physical determinants. Both determinants are considered to be proximate forces modifying the association of change in cognition and physical mobility. Other determinants in the Webber framework are considered control variables. Specifically, the main research questions are:
-
1.
Is change in cognition associated with change in physical mobility?
-
2.
Do depression, locus of control, gait speed, and grip strength intervene in the association of change between cognition and mobility? If so,
-
a.
Do they play intervening roles along the continuum of values of the measurement instruments, from the lower to the higher end?
-
b.
Or, is there a threshold at which they start to intervene?
-
a.
The first question pertains to the main issue raised within the Webber framework. The second question identifies four proximate intervening variables, while questions 2.a and 2.b specify the mechanisms – mediation and moderation - through which these variables act. Figure 1 models the relationship among the six variables, including control variables. Mediation is illustrated by using psychological determinants, and moderation by using the physical determinants.These research questions were examined using data from a longitudinal study of frailty – FRéLE (Fragilité: étude longitudinale de ses expressions [21]). Growth mixture models were used, simultaneously testing the association among the set of variables at baseline, or at a fixed state, and the association over time, or the rate of change [22]

Theoretical Model*
.
Methods
Participants and design
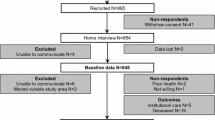
The FRéLE study sampled community-dwelling older adults (aged 65 and over) from three locations in the province of Québec, Canada: a metropolitan area (Montréal); a mid-sized city (Sherbrooke); and a small town and surroundings (Victoriaville). Participants were recruited in 2010 by a random sample drawn from the Québec Medicare database. The sample was stratified by sex, age, and location to secure a sufficient number of participants presenting with frailty. Individuals with significant hearing problems, or inability to speak either French or English were excluded. From the database, 4915 individuals were identified and 432 were excluded based on the study screening criteria. Of the 4483 qualified individuals, 52.2% refused to participate. Of the remaining 2141 individuals, 20% dropped out of the survey before T0 (baseline), 2% could not be contacted, and 1.3% did not complete the questionnaire, leaving a total of 1643 participants in the study (see Additional file 1: Part 1 for sample characteristics and Additional file 5).
Participants underwent a series of functional and psychosocial measurements carried out by trained health professionals at baseline (T0), and two annual follow-ups (T1, T2). When moderate to severe cognitive issues were suspected, the consent of a trustee or fiduciary was obtained. The research protocol was approved by the Research Ethics Committee of the Jewish General Hospital (#15–182). Preliminary analysis revealed that the sociodemographic characteristics and health status of FRéLE participants reflected the community-dwelling elderly population across the province [23].
Measures
Predictor variable
Cognitive function (MoCA)
Cognitive function was measured using the Montreal Cognitive Assessment instrument [24]. MoCA scores ranged from 0 to 30, with lower scores representing greater cognitive impairment. The test-retest reliability of the MoCA is high, along with its internal consistency [24]. FRéLE respondents with scores above 23 on the Mini-Mental State Evaluation [25] were given the MoCA. The 66 respondents excluded from taking the MoCA were considered to have a lower cognitive status. They were not excluded from the analysis and were censured to the left. In the current study, continuous MoCA scores were used.
Predicted variable
Life-space mobility (LSA)
The Life-Space Assessment index [1] was used to investigate life-space mobility. In the LSA, five different types of life-space are assessed: within-home, around home, neighborhood, town and outside of town. For each type of life-space, participants reported the frequency of movement during the previous 4 weeks, and whether assistance was needed. LSA scores ranged from 0 to 120, with higher scores reflecting greater life-space mobility. The LSA shows excellent test-retest reliability over a two-week period [1].
Intervening variables
Depressive symptoms (GDS)
Depressive symptoms were assessed using the 15-item version of the Geriatric Depression Scale [26]. GDS scores ranged from 0 to 15, with higher scores indicating higher levels of depressive symptoms. In order to align GDS scores with other time-varying variables scores, they were transformed: high scores indicated lower depressive symptoms. Continuous GDS scores were used in this study.
Locus of control (LoC)
The Personal Mastery Scale [27] is a seven-item scale assessing the extent of the belief that one is able to control or influence outcomes. For each item, scores ranged from 1 (strongly agree) to 4 (strongly disagree), with higher scores reflecting a higher level of control.
Gait speed (gait)
Walking speed (cm/sec) was assessed by recording the time required to walk 4, 3, or 2.44 m (according to the space available in the participant’s home) [28].
Grip strength (grip)
Handgrip strength was measured using the hand Baseline vigorimeter, following American Society of Hand Therapists recommendations [29]. Three measures for each hand were taken, alternating between the dominant and non-dominant hand. For the current study, the variable represented the average score in KiloPascal (KPa) of the three measures from the strongest hand.
Control variables
Control variables were assessed by a series of items on sex, age, education, annual income, number of chronic illnesses, and living site (metropolitan area, mid-sized city, small town) [30].
Statistical analysis
Modelling change on time-varying variables
The predictor variable (MoCA), the predicted variable (LSA), and the four intervening variables (Gait, Grip, GDS, and LoC) are time-varying indicators, as is one of the control variables (number of chronic illnesses). Change in each of the seven variables over the three observed time periods was modelled using growth modelling [31] with non-ignorable dropout cases [32]. At each period, the average of the time-varying variables at T0 was subtracted from the corresponding score. LSA, MoCA, gait speed, and grip strength scales were transformed by dividing each by a constant in order to align the range of variance values among all variables [22].
Observed scores for LSA (Lsam_t0; Lsam_t1; Lsam_t2) at the three time periods are shown in Fig. 2 with rectangles; above the rectangles, linked with arrows, are the associated standard errors (not shown). Over three time periods, the variables are patterned by two parameters: their intercepts (iL6-type), representing state or cross-sectional results; and the slope (sL6-type), representing change (increase, decrease, or stability). Coefficients for intercept with observed scores at each period are fixed to “1”, and for slope to “0”, “1” and “2” [31]. Change parameters for T0 are fixed to zero for identification purposes. Inasmuch as non-null standard errors are associated with intercept, respondent scores vary. Though slope may signal changes, the standard errors may not be significantly different from zero, inasmuch as the amount of change is not different among respondents. In this case, the cohort of respondents changes collectively in the same way from one time period to another.The first step in the analysis estimates the growth model parameters for each predicted and predictor variable and for the intervening time-varying variables, adjusting for control variables. Level of significance was set at α ≤ 0.05. The set of non-statistically significant growth model coefficients is then fixed to zero and tested to examine whether they can be excluded from further analysis using bootstrap likelihood ratio test (BLRT) and Bayesian information criterion (BIC).

Growth model: One variable
Pattern-mixture modelling (PMM) is used to model non-ignorable dropout cases (Fig. 2) [32, 33]. PMM does not explore causal effects of observed variables on dropout [32]. Rather, sources of variation in the outcome variables are identified.
Modelling change in LSA and MoCA
The association of MoCA with LSA, adjusting for control variables, is estimated using three terms: the regression of the intercept of LSA (iLSA) on 1) the intercept of MoCA (iMoCA); and the regression of the slope of LSA (sLSA) on 2) iMoCA and 3) sMoCA.
Parameter estimates for MoCA and for LSA growth models (Table 1) may change with the regression of LSA on MoCA. For example, the coefficient for dropout may lose statistical significance, inasmuch as MoCA and LSA contribute to loss of respondents between panels.
Muthén and Muthén [22] proposed the decomposition of complex models into parts, integrating the parts using resulting estimated parameters as starting values. This strategy was used in building the model to test our main hypotheses (Fig. 1). As in Cheong et al., [34] shapes of the growth trajectory for each intervening variable were investigated.
Mediating and moderating the association of MoCA with LSA
The direct association of MoCA with LSA, and the mediation and moderation of psychosocial characteristics and physical performance between MoCA and LSA are estimated with the Muthén and Asparouhov [31] web of hypotheses found in Fig. 3. The terms in Fig. 3 were derived from the expected value of LSA conditional on MoCA, and on the intervening variables [31]. Thus, the expected value of LSA is conditional based on:
-
1.
The coefficient of MoCA: β2. This is the Baron and Kenny [17] estimation of the direct effect of MoCA on LSA;
-
2.
The product of the coefficient of a mediator and MoCA with the coefficient of LSA and this mediator: β1ϒ1. This is the Baron and Kenny [17] formulation of the mediation hypothesis, with extensions by MacKinnon et al. [35] and Preacher et al.; [36]
-
3.
The term for moderators: β3ϒ1. This is homologous with the Hayes index [37] of moderated mediation when the interaction involves the predictor and a mediator variable. In the Baron and Kenny scheme, [17] the interaction term β3 alone defines moderation; [38]
-
4.
The term β3ϒ0. Because ϒ0 is not involved in the association of MoCA with intervening variables, [31] β3ϒ0 does not contribute to indirect association, but to direct association. Thus, even though β2 = 0, the direct association of MoCA with LSA can be significant.

Direct effects, mediators and moderators: A web of hypotheses
Modeling intercept and slope introduces restrictions among the associations. Slope represents change occurring across all observation points, while intercept involves observations at baseline only. Thus, slope cannot predict intercept, but intercept can predict slope. The Parallel Process Latent Growth model [34] is an example. This model has been extended to include: [39] 1) the intercept-only model, where intercepts are sole mediators; 2) the slope-only model, where slopes are sole mediators; and 3) the multiple mediation model, where both intercepts and slopes are mediators. Intercepts are not mediators for other intercepts in any of these models. Thus, in these models, the structure of association among the intercepts is considered ignorable [40]. The FRéLE design is observational and longitudinal. Two data generating processes are proposed as expressions of the theoretical model of change originating from the Webber framework: 1) observations at baseline resulting from the cumulative operation of the model over the life-course, and 2) changes during the longitudinal observational period (2 years). This two-way process requires that the mediation and moderation structure is imposed on both intercepts and slopes.
Null hypotheses, as shown in Fig. 3, were tested using the Mplus constraint procedure [22]. Standard errors in the indicators for mediator and moderator were bootstrapped for all models, except for the model with two interaction terms. The bootstrap procedure could not be applied in this latter case, as the computer time required to obtain estimates became unwieldy on a 2-Xeon-based machine with 32 threads.
Results
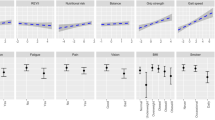
At baseline, the average score on the LSA original scale was 62.6, decreasing somewhat over time. The MoCA score was below the threshold of 26 for normal cognitive functioning, [24] but increasing from baseline to T1. Grip strength was the only intervening variable with a continuing, decreasing trend. Gait speed was slightly above the cut-off point for acceptable functioning (8 cm/sec), with an average of 8.8 cm/sec. Gait speed and both psychosocial determinants were stable.
Estimating change in time-varying variables
Preliminary analysis was conducted to ensure that change observed in time-varying variables could not be confounded by unstable, unreliable measurements. Results suggested that change could not be attributed to measurement errors (Additional file 2: Part 2).
Table 1 provides the parameter estimates of modelling change for each of the intervening variables, adjusted for control variables. There were significant variations in respondent scores. Growth rates were negative on LSA, gait speed, grip strength, and GDS, and positive on MoCA. Dropouts had lower scores than respondents who remained in the study at T1, suggesting that the estimated positive values of growth rate on MoCA may be a survival effect. Though growth rate for LoC did not change significantly between periods, variations in respondent growth rates were obtained. Finally, except for MoCA, residual errors were smaller at T2 than at T0, indicative of a decrease in the heterogeneity of respondents (Additional file 3: Part 3).
Regression of MoCA and LSA
The coefficients for the regression of MoCA and LSA, with control variables included in the model, are shown in Table 2. The growth rates for MoCA and LSA and their random terms were more or less in the same range as estimates in Table 1. However, the association of iMoCA with sMoCA lost statistical significance. Only the regression coefficients of the LSA intercept (iLSA) on MoCA intercept (iMoCA) were significant. Thus, if life-space increased with MoCA, a change in life-space was not sensitive to levels and change in MoCA.
Estimating interactions
Following the Muthén and Muthén procedure, [22] interactions among the intervening variables and MoCA were grouped in six parts, one for each intervening variable intercept and slope with significant standard error (Table 3). Interaction was defined by the rule that iLSA cannot be regressed on slope terms for MoCA and intervening variables, and intervening variable intercept terms cannot be regressed on sMoCA. Intervening variable intercept terms were accepted as potential moderators between sMoCA and sLSA inasmuch as their association with sMoCA was not statistically significant. Latent interaction terms were obtained with the “xwith” operator in Mplus, [22] as in Luo et al. [41]. No interaction terms involving GDS and LoC were significant (Table 3, Part 2). The interaction of gait speed (iGait), and grip strength (iGrip) with iMoCA was significant (Table 3, Part 1) Interaction of iGrip with sMoCA almost reached significance for sLSA at the 0.05 level. Significant interaction terms, plus interaction of iGrip with sMoCA for sLSA, were introduced in a model including control variables, and the predictor, intervening, and predicted variables (Table 4). Interaction terms for iLSA were statistically significant when tested one at a time, but their BIC statistics were nearly equal to BIC for the model without interaction (Table 4, Part A.1). Also the null hypothesis for the interaction term for sLSA could not be rejected (Table 4, Part A.1). Both interaction terms for iLSA were entered in a model (Table 4, Part B.1), and the contribution of each examined. The contribution of iGait was not significant, while the null hypothesis for the interaction term with iGrip was rejected (Table 4, Part B.2). Finally, the significance of the interaction involving iGrip was tested against a new null model including the term for iGrip. The null hypothesis of no interaction was rejected (Table 4, Part B.3) and the interaction term of iMoCA with iGrip for iLSA was the only interaction retained in the final model.
Introducing intervening variables
A single model was set up that simultaneously included all statistically significant parameters from the above analytical steps. Parameters were excluded if both the estimates and the associated log likelihood ratio tests did not reach statistical significance. Results are shown in Figs. 4, 5 and 6. These figures are organized based on MoCA and LSA intercept and slope terms for clarity. Also, only the significant structural parameters involving association among intercept and slope for MoCA, the intervening variables, and LSA are shown. Control variables and residuals have been excluded from these figures for greater clarity.

Mediators and Moderators: MoCA’s intercept & LSA’s intercept*

Mediators and moderators: MoCA’s intercept & LSA’s slope*

Mediators and moderators: MoCA’s slope & LSA’s slope*
The model for the association of iMoCA with iLSA is shown is Fig. 4. Though the direct association between the two is not significant, it was included in the model because of the iMoCA-iGrip interaction terms. Thus, the possibility that iGrip is a moderator was examined. All intervening variables were shown to be associated with iMoCA and all, except iLoC, were associated with iLSA. iGDS, iGait and iGrip were tested as mediators. Estimated regression parameters involving sLSA and iMoCA are shown in Fig. 5. sLSA was associated with iGait and sGDS. Only iGait may have a mediator relationship with iMoCA and sLSA. Finally, in Fig. 6, the terms for change are emphasized to enhance the association among sMoCA and sLSA, and the intervening variables. No direct association was found between the two variables. Also, sMoCA is associated with sGait, sGrip and sGDS. As the sGait and sGrip standard errors were fixed to zero, no association with sLSA could be estimated. In this case, only sGDS could be considered to be a mediator. In summary, the set of our main hypothesized mediations, except for LoC, was potentially retained for mediation involving intercept only. iGrip was retained as a moderator between iMoCA and iLSA. The term for change on LSA (sLSA) was not related to the intercept or slope for MoCA. sGDS and iGait were associated with sLSA, and sGDS almost reached statistical significance as a mediator between sMoCA and sLSA.
Statistical significance of mediator and moderator terms
The term for direct effect (β3ϒ0) was not statistically significant. All mediator and moderator relations shown in Figs. 4, 5 and 6 were statistically significant, except for the mediation of iGrip between iMoCA to iLSA. However, iGrip remained a statistically significant moderator (table not shown).
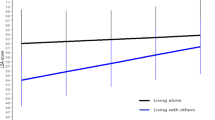
Figure 7 shows three regression lines for standardized iLSA scores on standardized iMoCA scores. The association of iMoCA with iLSA is progressively headed toward zero as iGrip scores increase. iGrip appears to compensate for the association of iMoCA with iLSA at lower scores on iMoCA. Thus, the association of iMoCA with iLSA is significant only for low iGrip scores. However, statistical significance is not a measure of association. Statistically significant coefficients in this study were small (Additional file 4: Part 4).

Averages standardized iLSA scores predicted by iMoCA at three levels of standardized scores for iGrip
The weighted distribution of the number of FRéLE respondents on the iMoCA continuum is shown in Fig. 7 as shaded bars. The modification of the association of iMoCA with iLSA at low levels of iGrip concerns a minority of respondents.
Discussion
The aim of this study was to examine the longitudinal association between cognitive decline and change in life-space mobility in community-dwelling older adults, and to investigate the impact of moderators and mediators on this association. Based on the Webber framework, two questions were asked. The first examined the extent that change in cognitive function was associated with change in life-space mobility. In a model with cognition as the sole predictor, including controlled variables, the direct association was not significant. To our knowledge, no other studies have examined associations between change in cognitive function and change in life-space mobility. In our study, the direct association between the two variables was significant at baseline, suggesting an accumulation of reciprocal effects throughout the life course. Yet, with the introduction of intermediate psychosocial and physical performance variables, this direct association fell into the non-statistically significant range. Some studies did not report cross-sectional associations between cognition and life-space mobility, [11,12,13] while others showed a relationship [2, 7,8,9,10]. Discrepancies between these findings may be explained by heterogeneity in samples (e.g., Canadians, Americans female, Mexican Americans), sample size (ranging from 300 to 2737), age of respondents (e.g., 65 years and older, 75 years and older, 65–74 years), and country in which the studies were conducted (USA, Canada, Brazil, Columbia, Finland). That is, associations between cognition and life-space mobility may be influenced by individual as well as sociocultural factors.
The second question dealt with the mediation and mediator roles of psychosocial variables (depression and Locus of Control) and physical performance variables (gait speed and grip strength), and their potential to affect the association between change in cognitive function and life-space mobility. Our results showed a weak mediating effect for change in depression. Locus of control was not associated with change in life-space mobility; it had no mediating nor moderating roles. In contrast, one study reported that locus of control moderated association between cognition and life-space mobility at baseline [9]. Baseline values on gait speed were related with change in life-space mobility. Though change was observed at the cohort level in gait speed and grip strength, the change rate did not vary among individuals. The association of change in gait speed and grip strength with change in life-space mobility could not be estimated.
At baseline, gait speed played a mediating role in the association between cognition and life-space mobility. Examined separately, interactions of gait speed and grip strength with cognition were statistically significant. However, only the interaction of grip strength remained statistically significant when both were entered simultaneously in the structural equation. Grip strength played a moderating role at baseline only: the association of cognition with life-space mobility decreased with increasing grip strength up to a point where the association had no statistical significance. Of the psychosocial variables, baseline depression showed a trend towards mediating association between cognitive function and life-space mobility. Locus of control was not associated with life-space mobility. Our results, at baseline, thus replicate those of studies reporting an association between higher depressive symptoms and lower life-space mobility [1, 2, 8].
Changes were observed in this study over a two-year period, a short period of time by any standard. Nonetheless, change in cognition and life-space mobility has been observed. Locus of control did not change at the population level, but change in individuals was observed. Grip strength decreased chronologically at the same level across the entire FRéLE sample.
To sum up our results, in persons aged 65 and over, change in life-space mobility occurs slowly and is not related to cognition at the population level. Only change in depression and gait speed at baseline was associated with change in life-space mobility. A low level of association was obtained between the Webber framework determinants and life-space mobility.
Our results support the fact that slow change, observed over time throughout the aging process is complex and not well-understood. Our results also suggest that the process of change in life-space mobility extends over a long period of time, including the entire life course. Thus, from a population health perspective, persons aged 65 and over cumulate life-long social, psychosocial, and health experiences, and any change in health status, from then on, depends on their life course. Whether or not conclusions can be drawn on the efficacy of population health interventions on slowly changing issues observed at a population level is a difficult topic. Whether public health interventions or policies on physical performance at the population level could affect the process of change in life-space mobility, given changes in cognitive ability, is still an unanswered question within the framework of this paper. Mobility in itself is a determinant of health [42]. Indeed, mobility is essential to create and maintain relationships and to participate socially [43]. Social participation has been associated with benefits to physical, cognitive and mental health of seniors [44]. Therefore, future studies should focus on a better understanding of the impact of determinants of health on mobility as well as the impact of mobility on health in seniors, in light of the Webber framework.
There are some limitations to the current study. First, although longitudinal, the study was not designed to determine the direction of causal processes in cognitive deficit, life space, psychosocial characteristics, or physical function, but rather to estimate the source of variations of change in life-space mobility within the Webber framework. Our research questions were legitimate, given our use of growth curve modelling and our understanding of causality in an observation-based longitudinal study design. Causality was not examined, but we tested and used null hypotheses for parameters derived from a structural equation model to get insight on the absence of causality in the set of predictor, intermediate, and predicted variables.
Second, association and interaction among the intermediate variables have not been considered. Also, it could be argued that some of the controlled variables should have been considered for moderation effects. Modeling these associations and interactions would have increased the already complex structural models tested in this paper, pushing to the limit our ability to obtain reliable parameter estimates.
Third, FRéLE was not designed to be representative of the older population in the three locations. However, the distribution of FRéLE characteristics does reflect the elderly population across Quebec.
Fourth, respondents lost to follow-up had lower scores on predictor, intermediate, and predicted variables, than those who remained in the study. However, these sources of variations attributable to non-ignorable missing cases were included in models. Fifth, only changes occurring in a short period of time were observed in the FRéLE study. However, significant changes in cognition and life-space, and psychosocial variables were observed over a two-year period. The variables in this study may require an observation period of longer than 2 years for their association in change to appear. We have not been able to identify latent classes for change in life-space mobility, suggesting that patterns of change are uniform in FRéLE respondents, whatever their age. It is possible that latent classes for change in the predictor and intermediate variables exist. However, estimating latent classes for change on multiple variables introduces complexity in the modelling of the structural equations, in the interpretation of results, and in the estimation procedures. Future work in this direction is under consideration (Additional file 5).
Conclusions
In conclusion, differences in respondents at baseline may have resulted from sequences of multiple processes over their life course: resilience, recovery, improvement or sustained decline [45]. The baseline variables of association, mediation and moderation could be considered as a starting point to examine life course processes. The type of processes that individuals, population subgroups, and whole populations experience could have resulted in different population health states, at baseline and over the course of our study. The FRéLE study was not set up to identify these processes. Nonetheless, locating FRéLE baseline results within a life course perspective opens up opportunities for new studies. In a life course perspective [46] where the baseline model (Fig. 4) can be considered the result of cumulative processes, a strong case can be made in retaining a mediating hypothesis for physical performance variables and depression, and a moderating hypothesis for grip strength. Though the iGait interaction term was not significant when it was considered with iGrip, difficulties in estimating multiple interaction terms in structural equation models suggest caution before rejecting the moderation hypothesis for iGait in future studies. Finally, correlated change in cognitive process and life-space at the population level seems to occur at a low level over all ages, 65 and older. A two-year period may be too short to capture these changes. Also, the association of cognition with life-space mobility seems to be limited to a small proportion of people, as suggested by the moderator role of grip strength. In effect, association of cognition with mobility was limited to lower scores on grip strength, while the sample grip strength scores were skewed toward middle and high scores. Finally, baseline results can be considered a cross-sectional sample, while growth-modeling results are derived from a longitudinal design. In any case, the cross-sectional data and longitudinal data in the FRéLE sample did not yield the same results.
Abbreviations
- BIC:
-
Bayesian information criterion
- BLRT:
-
Bootstrap likelihood ratio test
- FRéLE:
-
Fragilité: étude longitudinale de ses expressions [Frailty: A longitudinal study of its expression]
- Gait:
-
Gait speed
- GDS:
-
Geriatric depression scale
- Grip:
-
Grip strength
- i :
-
Intercept
- KPa:
-
KiloPascal
- LoC:
-
Locus of control
- LSA:
-
Life-space assessment
- MOCA:
-
Montreal cognitive assessment
- PMM:
-
Pattern-mixture modelling
- s :
-
Slope
References
Baker PS, Bodner EV, Allman RM. Measuring life-space mobility in community-dwelling older adults. J Am Geriatr Soc. 2003;51(11):1610–4.
Xue Q-L, Fried LP, Glass TA, Laffan A, Chaves PH. Life-space constriction, development of frailty, and the competing risk of mortality: the Women's health and aging study I. Am J Epidemiol. 2007;167(2):240–8.
Webber SC, Porter MM, Menec VH. Mobility in older adults: a comprehensive framework. The Gerontologist. 2010;50(4):443–50.
Wettstein M, Wahl HW, Shoval N, Oswald F, Voss E, Seidl U, Frolich L, Auslander G, Heinik J, Landau R. Out-of-home behavior and cognitive impairment in older adults: findings of the SenTra project. J Appl Gerontol. 2015;34(1):3–25.
O'connor ML, Edwards JD, Wadley VG, Crowe M. Changes in mobility among older adults with psychometrically defined mild cognitive impairment. J Gerontol B Psychol Sci Soc Sci. 2010;65((3):306–16.
Ball K, Owsley C. Increasing mobility and reducing accidents of older drivers. In: Schaie KW, Pietrucha M, editors. Mobility and transportation in the elderly. New York: Springer Publishing Company, Inc.; 2000. p. 213–51.
Barnes LL, Wilson RS, Bienias JL, Mendes de Leon CF, Kim H-JN, Buchman AS, Bennett DA. Correlates of life space in a volunteer cohort of older adults. Exp Aging Res. 2007;33(1):77–93.
Peel C, Sawyer Baker P, Roth DL, Brown CJ, Brodner EV, Allman RM. Assessing mobility in older adults: the UAB study of aging life-space assessment. Phys Ther. 2005;85(10):1008–119.
Sartori AC, Wadley VG, Clay OJ, Parisi JM, Rebok GW, Crowe M. The relationship between cognitive function and life space: the potential role of personal control beliefs. PsycholAging. 2012;27(2):364–74.
Rantakokko M, Iwarsson S, Portegijs E, Viljanen A, Rantanen T. Associations between environmental characteristics and life-space mobility in community-dwelling older people. J Aging Health. 2015;27(4):606–21.
Al Snih S, Peek KM, Sawyer P, Markides KS, Allman RM, Ottenbacher KJ. Life-space mobility in Mexican Americans aged 75 and older. J Am Geriatr Soc. 2012;60(3):532–7.
Curcio C-L, Alvarado BE, Gomez F, Guerra R, Guralnik J, Zunzunegui MV. Life-space assessment scale to assess mobility: validation in Latin American older women and men. Aging Clin Exp Res. 2013;25(5):553–60.
Silberschmidt S, Kumar A, Raji MM, Markides K, Ottenbacher KJ, Al Snih S: Life-space mobility and cognitive decline among Mexican Americans aged 75 years and older. J Am Geriatr Soc 2017:Epub ahead of print.
Allman RM, Baker PS, Maisiak RM, Sims RV, Roseman JM. Racial similarities and differences in predictors of mobility change over eighteen months. J Gen Intern Med. 2004;19(11):1118–26.
Poranen-Clark T, von Bonsdorff MB, Rantakokko M, Portegijs E, Eronen J, Kauppinen M, Eriksson JG, Rantanen T, Viljanen A: Executive function and life-space mobility in old age. Aging Clin Exp Res 2017:Epub ahead of print.
Shah RC, Maitra K, Barnes LL, James BD, Leurgans S, Bennett DA. Relation of driving status to incident life space constriction in community-dwelling older persons: a prospective cohort study. J Gerontol A: Biomed Sci Med Sci. 2012;67(9):984–9.
Baron RM, Kenny DA. The moderator–mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–82.
Atkinson HH, Rapp SR, Williamson JD, Lovato J, Absher JR, Gass M, Henderson VW, Johnson KC, Kostis JB, Sink KM. The relationship between cognitive function and physical performance in older women: results from the women’s health initiative memory study. J Gerontol A Biomed Sci Med Sci. 2009;65((3):300–6.
Watson N, Rosano C, Boudreau R, Simonsick E, Ferrucci L, Sutton-Tyrrell K, Hardy S, Atkinson H, Yaffe K, Satterfield S. Executive function, memory, and gait speed decline in well-functioning older adults. J Gerontol A Biomed Sci Med Sci. 2010;65((10):1093–100.
Yaffe K, Blackwell T, Gore R, Sands L, Reus V, Browner WS. Depressive symptoms and cognitive decline in nondemented elderly women: a prospective study. Arch Gen Psychiatry. 1999;56(5):425–30.
Galand C, Béland F, Fletcher J. FRéLE team: FRéLE : une étude québécoise sur la fragilité [FRéLE: a study on fraily in Quebec]. In: Béland F, Michel H, editors. La fragilité des personnes âgées: définitions, controverses et perspectives d’action [Fraily in older adults: definitions, controversies, and perspectives of action]. Rennes: Presses de l’EHESP; 2013. p. 177–204.
Muthén LK, Muthén BO: Mplus User’s guide, 7th edition edn. Los Angeles, CA: Muthén & Muthén; 1998-2017.
Provencher V, Béland F, Demers L, Desrosiers J, Bier N, Avila-Funes JA, Galand C, Julien D, Fletcher J, Trottier L, et al. Are frailty components associated with disability in specific activities of daily living in community-dwelling older adults? A multicenter Canadian study. Arch Gerontol Geriatr. 2017;73:187–94.
Nasreddine ZS, Phillips NA, Bedirian V, Charbonneau S, Whitehead V, Collin I, Cummings JL, Chertkow H. The Montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–9.
Folstein MF, Folstein SE, McHugh PR. “mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–98.
Yesavage JA, Sheikh JI. 9/geriatric depression scale (GDS) recent evidence and development of a shorter version. Clin Gerontol. 1986;5(1–2):165–73.
Pearlin LI, Menaghan EG, Lieberman MA, Mullan JT. The stress process. J Health Soc Behav. 1981:337–56.
Guralnik JM, Simonsick EM, Ferrucci L, Glynn RJ, Berkman LF, Blazer DG, Scherr PA, Wallace RB. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49(2):M85–94.
Fess EE. Grip strength. In: Casanova JS, editor. Clinical assessment recommendations. 2nd ed. Chicago: American Society of Hand Therapist; 1992. p. 41–5.
Groll DL, To T, Bombardier C, Wright JG. The development of a comorbidity index with physical function as the outcome. J Clin Epidemiol. 2005;58(6):595–602.
Muthén B, Asparouhov T. Causal effects in mediation modeling: an introduction with applications to latent variables. Struct Equ Model Multidiscip J. 2015;22(1):12–23.
Muthén B, Asparouhov T, Hunter AM, Leuchter AF. Growth modeling with nonignorable dropout: alternative analyses of the STAR* D antidepressant trial. Psychol Methods. 2011;16(1):17–33.
Demirtas H, Schafer JL. On the performance of random-coefficient pattern-mixture models for non-ignorable drop-out. Stat Med. 2003;22(16):2553–75.
Cheong J, MacKinnon DP, Khoo ST. Investigation of mediational processes using parallel process latent growth curve modeling. Struct Equ Model. 2003;10(2):238–62.
MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychol Methods. 2002;7(1):83.
Preacher KJ, Rucker DD, Hayes AF. Addressing moderated mediation hypotheses: theory, methods, and prescriptions. Multivar Behav Res. 2007;42(1):185–227.
Hayes AF. An index and test of linear moderated mediation. Multivar Behav Res. 2015;50(1):1–22.
Chmura Kraemer H, Kiernan M, Essex M, Kupfer DJ. How and why criteria defining moderators and mediators differ between the Baron & Kenny and MacArthur approaches. Health Psychol. 2008;27(2S):S101.
von Soest T, Hagtvet KA. Mediation analysis in a latent growth curve modeling framework. Struct Equ Model. 2011;18(2):289–314.
Holland PW, Rubin DB. Causal inference in retrospective studies. ETS Res Rep Ser. 1987;1987(1):203–31.
Luo W, Lee K, Koh ICH. Do competitive performance goals and cooperative social goals conflict? A latent interaction analysis. Learn Individ Differ. 2015;39:186–92.
Gardner P. The role of social engagement and identity in community mobility among older adults aging in place. Disabil Rehabil. 2014;36(15):1249–57.
Pinquart M, Sorensen S. Influences on loneliness in older adults: a meta-analysis. Basic Appl Soc Psychol. 2001;23(4):245–66.
Stav WB, Hallenen T, Lane J, Arbesman M. Systematic review of occupational engagement and health outcomes among community-dwelling older adults. Am J Occup Ther. 2012;66(3):301–10.
Infurna FJ, Grimm KJ. The use of growth mixture modeling for studying resilience to major life stressors in adulthood and old age: lessons for class size and identification and model selection. J Gerontol B. 2017;73(1):148–59.
Kuh D, Ben-Shlomo Y. A life course approach to chronic disease epidemiology. 2nd ed. Oxford: Oxford University Press; 2004.
Acknowledgements
The authors wish to thank Claude Galand and John Fletcher for data management, and Rebecca Rupp for administrative support.
Funding
The FRéLE study was supported by the Canadian Institutes of Health Research – Instituts de recherche en santé du Canada (FRN# 82945). Additional funding was obtained from the Réseau québécois de recherche sur le vieillissement (Québec Research Network on Aging), Fonds de recherche du Québec – Santé (FRQS) (FRN# 3/31/2014). NB is supported by funding from the FRQS (Bursary # 29032).
The funding sources had no role in the design of the study, in collection, analysis, and interpretation of data, and in writing the manuscript.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
NB, DJ, LD and JD: Drafting the introduction; FB: Operationalizing the theoretical model, testing statistical models, responsible for the method and results sections; DJ: Involved in writing the methods section; FB, NB, DJ and LD: Responsible for the discussion section. All authors made substantial contributions to the study concept, development of the theoretical model, interpretation of results, and manuscript revision for intellectual content. All approved the final version and agreed to be accountable for aspects regarding accuracy and integrity of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The research protocol was approved by the Research Ethics Committee of the Jewish General Hospital (#15–182). Written consent was obtained from participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
Part 1 Characteristics of respondents. Describes the characteristics of the FRéLE sample. (DOCX 21 kb)
Additional file 2:
Part 2 Reliability of the time-varying variables. Examines the reliability of the time-varying variables to ensure that change observed in these variables was not confounded by unstable reliability of the measures. (DOCX 28 kb)
Additional file 3:
Part 3 Estimating change in each of the time-varying variables. Describes change in each of the time-varying variables. (DOCX 25 kb)
Additional file 4:
Part 4 Statistical significance and strength of association. Describes change in the predicted variable based on a 1-unit change in the predictor variable. (DOCX 23 kb)
Additional file 5:
Table S1. Characteristics of FRéLE participants. Table presenting descriptives of the FRéLE sample. (DOCX 26 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Béland, F., Julien, D., Bier, N. et al. Association between cognitive function and life-space mobility in older adults: results from the FRéLE longitudinal study. BMC Geriatr 18, 227 (2018). https://doi.org/10.1186/s12877-018-0908-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-018-0908-y