
Abstract
Background
As a gram-negative and microaerophilic bacterium, Helicobacter pylori (HP) is the main cause of chronic gastritis. Therefore, considering the high prevalence of HP infection worldwide, as well as the increasing prevalence of metabolic disorders, the present study aimed to investigate the relationship between HP infection eradication and metabolic profile.
Methods
This prospective case-control study was performed on patients with HP infection whom referred to 7 medical centers in 3 countries (Iran, Egypt, and Vietnam) in 2020–2021. The metabolic profile of all of the participants evaluated before starting of treatment for HP eradication and 3 months after the treatment. Then changes of metabolic profile compared between those with successful HP eradication (group A) and subjects who failed to eradicate (group B).
Results
Overall, 199 patients, including 93 male (46.7%) with the mean age of 44.5 years (18–93 years) included. Based on response to treatment, the participants allocate into group A (those who respond to HP eradication): 164 cases (82.42%); or group B as those who failed to achieve eradication (35 cases, 17.58%). Racially 86.9% of participants were Caucasian and 89% diagnosed as non-ulcer dyspepsia (NUD). The most prevalent comorbidity include hypertension (11.5%) and hyperlipidemia (10%) which were more prevalent in group B (P = 0.002). Three months after therapy, average weight of participants among those who achieved eradication (group A) decreased from 73.1 to 71.4 kg (P = 0.01), but in comparison with group B, was non-significant (P = 0.171). The BMI of patients before and after treatment did not show any significant differences. The biochemical parameters of patients before and after treatment were not significantly different regardless of treatment success (P > 0.05). The levels of total cholesterol and VLDL cholesterol after treatment were not significantly different from baseline values in two groups. HDL and LDL cholesterol levels before and after treatment in the resistant group were significantly higher than the responding group. Average serum TG level decreased significantly after treatment in the group A (P < 0.0001), in contrast to the resistant group (P = 0.356). The liver transaminases (AST and ALT) before and after treatment were not significantly different between the two groups (P > 0.05). The results of logistic regression showed that the eradication of infection has no significant affect any of the metabolic profile parameters.
Conclusion
HP infection treatment in individuals without significant metabolic disorders does not affect metabolic parameters up to 3 months after eradication. HP eradication among subjects with several comorbidities mandates eradication protocol intensification to avoid treatment failure.
Similar content being viewed by others

Introduction
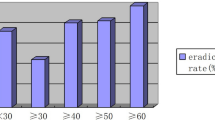
Helicobacter pylori (HP) infection is one of the most common infections globally and involves more than 50% of the human population. Moreover, it has a higher prevalence in developing countries [1,2,3]. Epidemiologic studies have reported prevalence of this infection about 24%, 37%, 47%, 55%, 63%, and 79% among the populations of Oceania, North America, Europe, Asia, Latin America, and Africa respectively [4, 5].
HP infection could be associated with several upper gastrointestinal problems, such as chronic gastritis, peptic ulcer and gastric cancer or lymphoma. Moreover, recent studies have reported a potential association between HP infection and some non-gastric problems, such as metabolic syndrome risk factors, atherosclerosis, and cardiovascular diseases, including myocardial infarction and stroke [6,7,8,9,10]. HP induced gastrointestinal inflammation may impair the uptake of glucose and lipids, resulting in altered lipid and glucose metabolisms. Moreover, some studies have reported a significant relationship between HP infection and increased risk of metabolic disorders. Such relations also state by systemic inflammation and altered leptin and ghrelin levels caused by HP infection [11,12,13,14,15].
According to recent evidences, abnormal lipid profile, including Low-Density Lipoprotein (LDL) and High-density Lipoprotein (HDL), are important metabolic risk factors for cardiovascular diseases and HP infection is associated with altered serum lipid levels [16]. Some studies have even reported significant relationships between HP infection and altered HDL, LDL, total cholesterol and Triglyceride (TG) levels [17]. One possibility is HP mediated atherogenic property by its effects on lipid and glucose metabolisms. Some evidences reported that successful eradication of HP infection can improve gastric mucosal damage and prevent subsequent gastric cancer and other related complications. However, the effect of HP eradication on lipid profile, glucose levels, and other parameters of the metabolic profile has not illustrated yet [18, 19].
A recent meta-analysis showed that HDL and TG levels improved significantly following HP eradication compared to baseline values before the treatment. However, LDL levels did not affected significantly by treatment [20]. On the other hand, an older meta-analysis reported that the HP eradication has no significant effect on serum lipid profile and insulin resistance [21, 22]. Therefore, considering the high prevalence of HP infection in worldwide, as well as the increasing prevalence of metabolic disorders, the present study aimed to investigate the relationship between HP infection eradication and metabolic profile.
Methods
This prospective case-control study conducted on patients with HP infection who attend in outpatient clinics of seven referral medical centers in three countries (Iran, Egypt, and Vietnam) in 2020–2021. The study approved by the ethics committee of Ahvaz Jundishapur University of Medical sciences (IR.AJUMS.HGOLESTAN.REC.1400.089) based on the principles of the Declaration of Helsinki for human research. Firstly, the purpose and method of conducting the study explained to the participants. Then, eligible patients requested to sign a written consent if they wished, before entering the study. The pertained ethic number and IRB approved and accepted by all of the participating centers.
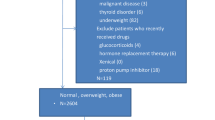
Inclusion criteria include age higher than 18 years, clinical diagnosis as peptic ulcer disease (PUD), non-ulcer dyspepsia (NUD), or intestinal metaplasia, confirmation of HP infection in biopsy sample by pathological report and positive fecal antigen test, and signing the consent form to participate in the study. Exclusion criteria include presence of serious underlying diseases including active malignancies, sever heart failure, uncontrolled diabetes mellitus, sever renal failure, advanced chronic liver disease, viral hepatitis, history of any gastric surgery, current pregnancy or lactation, and previous history of HP eradication during last 6 months before study.
At the beginning, the demographic characteristics of patients (age, sex, medical history, body mass index (BMI), smoking) recorded through a checklist. The metabolic profile of participants including Fasting Blood Sugar (FBS), alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), HDL-C, LDL-C, cholesterol, TG, BUN and Cr measured and determined. Then all of the patients treated for HP infection with one of the existing protocols based on responsible physician choice. The participants followed by weekly phone calls and requested to report any side effects or complication related to medical therapy.
All of the participants received eradication regimen for 2 weeks, then the therapy with PPI continued for four more weeks (totally 6 weeks). Two weeks after the end of the treatment period and discontinuation of the drugs (week 8), a stool antigen test (SATs) performed to prove the eradication and the effectiveness of the treatment. Based on success of eradication, the participant allocated to group A (those who achieved eradication) and group B (those who failed eradication). Three months after the end of treatment, the Metabolic profile of participants including blood glucose, lipid profile, and liver transaminases measured again and any changes compared between two groups.
Statistical methods
Statistical analysis performed by SPSS software (SPSS Inc., Chicago, IL, USA) version 22. For quantitative variables, the mean and median determined, and the data scatter from the standard deviation and Interquartile range (IQR) used. In qualitative variables, frequency and percentage used to describe the data. The normality of the data checked by Kolmogorov-Smirnov test and the Q-Q diagram. Non-parametric Mann-Whitney U and Chi-squared tests applied to analyze the results, and Wilcoxon test used to compare the changes of different parameters before and after treatment. Logistic regression (LR) used and the level of significance in the tests was considered 0.05.
Results
This study performed on 199 patients, including 93 male (46.7%) with the mean age of 44.57 ± 13.92 years (18–93 years) (Table 1). Based on response to treatment, the participants allocate into group A (those who respond to HP eradication): 164 cases (82.42%); or group B as those who failed to achieve eradication (35 cases, 17.58%). Racially 86.9% of participants were Caucasian. 89% of participants diagnosed as non-ulcer dyspepsia (NUD) (Fig. 1). The most prevalent comorbidity include hypertension (11.5%) and hyperlipidemia (10%) (Table 2) and prevalence of them was higher in group B who failed eradication (P = 0.002) (Table 1). There was no significant difference in the frequency of HP induced GI disease between two groups (P = 0.06) (Table 1).

Clinical diagnosis of participants (PUD Peptic ulcer disease; DU Duodenal ulcer; GU Gastric ulcer; IM Intestinal metaplasia; NUD Non-ulcer dyspepsia)
The most common therapeutic protocols include amoxicillin-based dual therapy and clarithromycin base triple or quadruple regimens (Table 3). The success rate of eradication among those without comorbidity was 86.8% versus 68% in subjects with any comorbidity (P = 0.0031).
Three months after therapy, average weight of participants among those who achieved eradication (group A) decreased from 73.1 to 71.4 kg (P = 0.01), but in comparison with group B, this weigh reduction was non-significant (P = 0.5) (Table 4). The BMI of patients before and after treatment did not show any significant differences. The biochemical parameters of patients before and after treatment were not significantly different regardless of treatment success (P > 0.05) (Table 4). The levels of total cholesterol and VLDL cholesterol after treatment were not significantly different from baseline values in two groups. HDL and LDL cholesterol levels before and after treatment in the resistant group were significantly higher than the responding group. Average serum TG level decreased significantly after treatment in the group A (P < 0.0001), but in the resistant group, no significant change was observed in TG serum level (P = 0.356) (Table 4).
The liver transaminases (AST and ALT) before and after treatment were not significantly different between the two groups (P > 0.05) (Table 4). The results of logistic regression showed that the eradication of infection has no significant affect any of the metabolic profile parameters. The adjusted logistic regression model based on various variables (including age, sex, race, nationality, underlying disease, type of HP induced GI disease, therapeutic regimen, and smoking), showed that eradication of HP infection had no significant effect on the any of the patients’ metabolic profile parameters (Table 5).
Discussions
According to findings of the current study, successful HP eradication could be accompany by a significant decrease in serum TG levels, 3 months after the treatment compared to baseline values while in Logistic regression model, it was non-significant (Table 5, P = 0.929). However, there was no difference between the responders and refractory cases in other metabolic profile parameters. Moreover, the levels of other metabolic profile parameters would not significantly change up to 3 months after the treatment. A study by Adachi et al. in 2018 reported the improving effect of HP infection eradication on the lipid metabolism of the affected patients. They compared the lipid profiles of the patients with and without HP infection and showed significantly lower HDL levels in the patients with HP [23]. Likewise, patients with successful HP eradication had higher HDL levels and lower total cholesterol, LDL, and TG levels compared to those with persistent HP infection.
A meta-analysis showed increased HDL and TG levels in the patients with HP infection following eradication compared to pre-treatment values. However, serum LDL levels were not significantly changed [20]. These findings were compatible with the results of current study, reporting significantly reduced TG levels following infection eradication. Moreover, a cohort study reported that the patients with successful HP infection eradication had significantly decreased HDL and increased LDL levels 1.5 years after the treatment compared to the group who were positive for HP infection [24]. A potential explain could be better appetite due to gastritis management after HP eradication.
According to another study, eradication of HP infection could significantly decrease the TG levels while causing a slight increase in HDL levels following 1 year and 8 weeks from commencing the treatment. However, other metabolic parameters were not significantly changed. On the other hand, a study by Maruyama et al. reported no significant changes in total cholesterol, TG, LDL, and HDL levels after HP infection eradication compared to values before the treatment, which could explain by the use of statins and anti-HP regimen in the patients [25]. Another study by Nam et al. reported the improving effect of HP treatment on the lipid profile of the affected patients, including increased HDL and decreased LDL levels, after a 2 year follow-up period [26].
A study by Haeri et al. (2018) in Iran did not show a significant difference in LDL and HDL levels between the patients with and without HP infection [19]. However, Ansari et al. (2010) reported significantly lower HDL and Apolipoprotein A1 (Apo A1) levels and higher total cholesterol, TG, LDL, Apolipoprotein B (Apo B), Alkaline Phosphatase (ALP), cholesterol-to-HDL ratio, and LDL-to-HDL ratio in the patients with HP infection compared to the control group [27]. Considering all these findings, the effect of HP infection on metabolic profile, including the lipid profile, is still controversial. Therefore, further studies are mandatory to confirm the changes in lipid profile due to HP infection, as well as the improving effect of HP eradication on lipid profile. On the other hand, the relation between HP infection and cardiovascular events and stroke have reported in several investigations [9, 10] and could be explained by potential involvement of HP infection in atherosclerosis pathogenesis by inducing local or systemic inflammation and subsequently stimulating plaque progression and instability [8, 11,12,13].
There was no significant intergroup or intragroup difference in other biochemical parameters, including hemoglobin, platelet, Mean Corpuscular Volume (MCV), creatinine, calcium, Thyroid-Stimulating Hormone (TSH), and vitamin D levels. However, a recent study by Shafrir et al. (2021) reported a relationship between vitamin D levels and HP infection, showing significantly lower vitamin D levels in patients with HP infection compared to normal non-infected individuals [28]. Moreover, the group who responded to treatment had significantly higher vitamin D levels compared to the unresponsive group. Therefore, it is possible that HP infection be able to disturb vitamin D absorption by induction of duodenal inflammation although this issue needs further verification in future studies.
The present study showed a non-significant decreased BMI in the responsive group 3 months after the treatment compared to the pre-treatment values (P = 0.074). Therefore, there was no concern about obesity and weight gain in the present study. Moreover, a study by Liou et al. (2019) showed that HP infection eradication could significantly reduce the BMI of the patients after 8 weeks of eradication treatment [29]. However, a study by Zojaji et al. (2013) did not show the significant effect of HP infection on BMI [30]. These findings were compatible with the present study and same as some other studies with similar results [31, 32]. Although, they were incompatible with several studies showing a significant BMI increase after HP infection eradication. Therefore, there is a potential negative relationship between HP infection and obesity [25, 33,34,35], and the controversy between different studies can be due to different populations and methods.
According to our results, there was no significant intergroup or intragroup difference in the Fasting Blood Sugar (FBS) of the patients. Therefore, eradication of HP infection had no significant effect on the patients’ FBS. However, some studies have shown the improving effect of HP eradication on FBS. For example, a study by Dogan et al. (2015) on 370 patients with normal glucose levels showed the improving effect of successful eradication of HP on FBS, HbA1c, and insulin resistance (IR-HOMA) of the patients 6 months after the treatment compared to pre-treatment values [22]. They concluded that HP eradication could significantly improve the FBS levels and insulin resistance in patients with normal glucose levels which is in contrast to finding of current study.
An interesting finding in current work is higher prevalence of comorbidities such as hypertension and hyperlipidemia among resistant cases who fail to achieve HP eradication (P = 0.02). This issue means higher probability of successful HP eradication among those without comorbidity (86.8% vs. 68%, P = 0.0031). If this issue prove in future studies, can interprets as necessity of HP eradication regimens intensification by prolongation of the course or using higher doses of antibiotics among those with several comorbidities.
The limitation of current work was short period of patients follow up (3 months) and it is postulated that longer follow up time be able to help further elucidation of any relation between HP infection and metabolic profile.
Conclusion
HP infection eradication significantly reduced the serum TG levels in the patients with successful eradication. However, it had no significant effect on other metabolic profile parameters up to 3 months after eradication. On the other hand, HP eradication among subjects with several comorbidities mandates eradication protocol intensification to avoid treatment failure.
Availability of data and materials
The DATA would be available based on personal request to corresponding author.
References
Diaconu S, Predescu A, Moldoveanu A, Pop CS, Fierbințeanu-Braticevici C. Helicobacter pylori infection: old and new. J Med Life. 2017;10(2):112–7.
Cho J, Prashar A, Jones NL, Moss SF. Helicobacter pylori infection. Gastroenterol Clin North Am. 2021;50(2):261–82.
Malfertheiner P, Megraud F, O’Morain CA, Atherton J, Axon AT, Bazzoli F, Gensini GF, Gisbert JP, Graham DY, Rokkas T, El-Omar EM. Management of Helicobacter pylori infection—the maastricht IV/florence consensus report. Gut. 2012;61(5):646–64.
Hooi JKY, Lai WY, Ng WK, Suen MMY, Underwood FE, Tanyingoh D, et al. Global prevalence of Helicobacter pylori infection: systematic review and meta-analysis. Gastroenterology. 2017;153(2):420–9.
Crowe SE. Helicobacter pylori infection. New Engl J Med. 2019;380(12):1158–65.
Upala S, Jaruvongvanich V, Riangwiwat T, Jaruvongvanich S, Sanguankeo A. Association between Helicobacter pylori infection and metabolic syndrome: a systematic review and meta-analysis. J Dig Dis. 2016;17(7):433–40.
Lim SH, Kim N, Kwon JW, Kim SE, Baik GH, Lee JY, Park KS, Shin JE, Song HJ, Myung DS, Choi SC. Positive association between Helicobacter pylori infection and metabolic syndrome in a Korean population: a multicenter nationwide study. Dig Dis Sci. 2019;64(8):2219–30.
Wang B, Yu M, Zhang R, Chen S, Xi Y, Duan G. A meta-analysis of the association between Helicobacter pylori infection and risk of atherosclerotic cardiovascular disease. Helicobacter. 2020;25(6):e12761.
Wang JW, Tseng KL, Hsu CN, Liang CM, Tai WC, Ku MK, Hung TH, Yuan LT, Nguang SH, Yang SC, Wu CK. Association between Helicobacter pylori eradication and the risk of coronary heart diseases. PloS One. 2018;13(1):e0190219.
Doheim MF, Altaweel AA, Elgendy MG, Elshanbary AA, Dibas M, Ali AA, Dahy TM, Sharaf AK, Hassan AE. Association between Helicobacter pylori infection and stroke: a meta-analysis of 273,135 patients. J Neurol. 2021;268(9):3238–48.
Crowe SE. Helicobacter pylori infection. N Engl J Med. 2019;380(12):1158–65.
Malfertheiner P, Megraud F, O’Morain CA, Gisbert JP, Kuipers EJ, Axon AT, et al. Management of Helicobacter pylori infection-the maastricht V/florence consensus report. Gut. 2017;66(1):6–30.
Katsiki N, Athyros VG, Karagiannis A, Mikhailidis DP. High-density lipoprotein, vascular risk, cancer and infection: a case of quantity and quality? Curr Med Chem. 2014;21(25):2917–26.
Vafaeimanesh J, Hejazi SF, Damanpak V, Vahedian M, Sattari M, Seyyedmajidi M. Association of Helicobacter pylori infection with coronary artery disease: is Helicobacter pylori a risk factor? Sci World J. 2014;2014:516354.
Budzyński J, Koziński M, Kłopocka M, Kubica JM, Kubica J. Clinical significance of Helicobacter pylori infection in patients with acute coronary syndromes: an overview of current evidence. Clin Res Cardiol. 2014;103(11):855–86.
Saito I, Yamagishi K, Kokubo Y, Yatsuya H, Iso H, Sawada N, et al. Association of high-density lipoprotein cholesterol concentration with different types of stroke and coronary heart disease: the Japan public health center-based prospective (JPHC) study. Atherosclerosis. 2017;265:147–54.
Mladenova I. Helicobacter pylori and cardiovascular disease: update 2019. Minerva Cardioangiol. 2019;67(5):425–32.
Xu Z, Li J, Wang H, Xu G. Helicobacter pylori infection and atherosclerosis: Is there a causal relationship? Eur J Clin Microbiol Infect Dis. 2017;36(12):2293–301.
Haeri M, Parham M, Habibi N, Vafaeimanesh J. Effect of Helicobacter pylori infection on serum lipid profile. J Lipids. 2018;2018:6734809.
Nam SY, Ryu KH, Park BJ, Park S. Effects of Helicobacter pylori infection and its eradication on lipid profiles and cardiovascular diseases. Helicobacter. 2015;20(2):125–32.
Upala S, Sanguankeo A, Saleem SA, Jaruvongvanich V. Effects of Helicobacter pylori eradication on insulin resistance and metabolic parameters: a systematic review and meta-analysis. Eur J Gastroenterol Hepatol. 2017;29(2):153–9.
Dogan Z, Sarikaya M, Ergul B, Filik L. The effect of Helicobacter pylori eradication on insulin resistance and HbA1c level in people with normal glucose levels: a prospective study. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2015;159(2):242–5.
Adachi K, Mishiro T, Toda T, Kano N, Fujihara H, Mishima Y, et al. Effects of Helicobacter pylori eradication on serum lipid levels. J Clin Biochem Nutr. 2018;62(3):264–9.
Wang Z, Wang W, Gong R, Yao H, Fan M, Zeng J, et al. Eradication of Helicobacter pylori alleviates lipid metabolism deterioration: a large-cohort propensity score-matched analysis. Lipids Health Dis. 2022;21(1):34.
Maruyama M, Kamimura K, Hoshiyama A, Hoshiyama K, Hoshiyama M, Hoshiyama Y, et al. Effect of Helicobacter pylori eradication on elder cases: observational study in community-based medicine. World J Clin Cases. 2017;5(12):412–8.
Nam SY, Ryu KH, Park BJ, Park S. Effects of Helicobacter pylori infection and its eradication on lipid profiles and cardiovascular diseases. Helicobacter. 2015;20(2):125–32.
Ansari MHK, Omrani M-d, Sayyah B, Ansari SK. Effect of Helicobacter pylori infection on the lipid, lipoproteins, apolipoprotein-A1, lipoprotein (a) and apolipoprotein-B in patients with gastritis. Afr J Microbiol Res. 2010;4(2):084–7.
Shafrir A, Shauly-Aharonov M, Katz LH, Paltiel O, Pickman Y, Ackerman Z. The association between serum vitamin D levels and Helicobacter pylori presence and eradication. Nutrients. 2021;13(1):278.
Liou JM, Chen CC, Chang CM, Fang YJ, Bair MJ, Chen PY, et al. Long-term changes of gut microbiota, antibiotic resistance, and metabolic parameters after Helicobacter pylori eradication: a multicentre, open-label, randomised trial. Lancet Infect Dis. 2019;19(10):1109–20.
Zojaji H, Ataei E, Sherafat SJ, Ghobakhlou M, Fatemi SR. The effect of the treatment of Helicobacter pylori infection on the glycemic control in type 2 diabetes mellitus. Gastroenterol Hepatol Bed Bench. 2013;6(1):36–40.
Kawano S, Kawahara A, Nakai R, Fu HY, Tsuji S, Tsujii M. Helicobacter pylori infection does not affect serum leptin concentration and body mass index (BMI) in asymptomatic subjects. J Gastroenterol. 2001;36(8):579–80.
Tatsuguchi A, Miyake K, Gudis K, Futagami S, Tsukui T, Wada K, et al. Effect of Helicobacter pylori infection on ghrelin expression in human gastric mucosa. Am J Gastroenterol. 2004;99(11):2121–7.
Albaker WI. Helicobacter pylori infection and its relationship to metabolic syndrome: Is it a myth or fact? Saudi J Gastroenterol. 2011;17(3):165–9.
Lane JA, Murray LJ, Harvey IM, Donovan JL, Nair P, Harvey RF. Randomised clinical trial: Helicobacter pylori eradication is associated with a significantly increased body mass index in a placebo-controlled study. Aliment Pharmacol Ther. 2011;33(8):922–9.
Kebapcilar L, Sari I, Renkal AH, Alacacioglu A, Yuksel A, Ilhan E, et al. The influence of Helicobacter pylori eradication on leptin, soluble CD40 ligand, oxidative stress and body composition in patients with peptic ulcer disease. Intern Med. 2009;48(24):2055–9.
Acknowledgements
This article is part of final thesis of Dr Azam Satari for her gastroenterology fellowship course. This study approved and endorsed by alimentary tract research center of Ahvaz Jundishapur University of Medical sciences without any financial support. The authors would like to dedicate this work to Professor Barry Marshall for his endless efforts and continues support of young researchers.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
PA as corresponding author; EH as clinical supervisor and main colleague; AP as main colleague in patient inclusion; AS as cooperative colleague in study design and arrangement; MJR as main colleague in patient inclusion; MN as main colleague in patient inclusion; AH as main colleague in patient inclusion; OE as main colleague in patient inclusion; MHA as main colleague in patient inclusion; QTT as main colleague in patient inclusion; MA as main colleague in patient inclusion; SB as main colleague in patient inclusion; SM as main colleague in patient inclusion; SJH as clinical supervisor; AS as Endocrinologist and supervisor. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki, so this study approved by ethical committee of Ahvaz Jundishapur University of Medical Sciences (IR.AJUMS.HGOLESTAN.REC.1400.089). Informed consent was obtained from all study participants and informed consent was obtained from all subjects and/or their legal guardian(s).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Alavinejad, P., Hajiani, E., Parsi, A. et al. Effect of Helicobacter pylori eradication on metabolic profile: an international, multicenter, case-control study. BMC Gastroenterol 22, 507 (2022). https://doi.org/10.1186/s12876-022-02604-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12876-022-02604-3