
Abstract
Background
Transarterial radioembolization (TARE) with yttrium-90 microspheres is a clinically effective therapy for hepatocellular carcinoma (HCC) treatment. This study aimed to perform a systematic review of the available economic evaluations of TARE for the treatment of HCC.
Methods
The Preferred Reported Items for Systematic reviews and Meta-Analyses guidelines was followed by applying a search strategy across six databases. All studies identified as economic evaluations with TARE for HCC treatment in English or Spanish language were considered. Costs were adjusted using the 2020 US dollars based on purchasing-power-parity ($US PPP).
Results
Among 423 records screened, 20 studies (6 cost-analyses, 3 budget-impact-analyses, 2 cost-effectiveness-analyses, 8 cost-utility-analyses, and 1 cost-minimization analysis) met the pre-defined criteria for inclusion. Thirteen studies were published from the European perspective, six from the United States, and one from the Canadian perspectives. The assessed populations included early- (n = 4), and intermediate-advanced-stages patients (n = 15). Included studies were evaluated from a payer perspective (n = 20) and included both payer and social perspective (n = 2). TARE was compared with transarterial chemoembolization (TACE) in nine studies or sorafenib (n = 11). The life-years gained (LYG) differed by comparator: TARE versus TACE (range: 1.3 to 3.1), and TARE versus sorafenib (range: 1.1 to 2.53). Of the 20 studies, TARE was associated with lower treatment costs in ten studies. The cost of TARE treatment varied widely according to Barcelona Clinic Liver Cancer (BCLC) staging system and ranged from 1311 $US PPP/month (BCLC-A) to 71,890 $US PPP/5-years time horizon (BCLC-C). The incremental cost-utility ratio for TARE versus TACE resulted in a 17,397 $US PPP/Quality-adjusted-Life-Years (QALY), and for TARE versus sorafenib ranged from dominant (more effectiveness and lower cost) to 3363 $US PPP/QALY.
Conclusions
Economic evaluations of TARE for HCC treatment are heterogeneous. Overall, TARE is a cost-effective short- and long-term therapy for the treatment of intermediate-advanced HCC.
Similar content being viewed by others


Background
Hepatocellular carcinoma (HCC) is the most common type of primary neoplasm of the liver, the sixth most common cancer, and the third leading cause of cancer death globally [1,2,3]. Liver cancer mortality accounts for 8.4% of all cancer deaths as of 2020 [3]. Patients with HCC have a significant humanistic and economic burden [4]. The annual direct costs for HCC patients, regardless of stage or treatment, ranged from $29,354.47 to $58,529.45 per patient in the United States. Also, indirect costs, such as reduced labour productivity, account for 10.8% ($49.1 million) of the overall annual cost (direct and indirect) of HCC [4].
The Barcelona Clinic Liver Cancer (BCLC) staging system is the most widely used and most frequently recommended by scientific societies. This is the only system that relates the prognostic evaluation (based on 5 stages) to the different treatment options [1, 2]. The recently updated BCLC guideline recommends first-line treatments such as ablation, resection, transplantation, and transarterial radioembolization (TARE) as an option for patients in the early stages of the disease (BCLC-0, BCLC-A) or patients with a tumour size ≤ 8 cm who are not eligible for ablative techniques or resection. For the intermediate stage (BCLC-B), treatment options include transplantation for patients with well-defined nodules, transarterial chemoembolization (TACE) for patients with the preserved portal flow, and a defined tumour burden, or systemic therapy. For advanced-stage (BCLC-C), systemic therapy based on immunotherapy (a combination of atezolizumab and bevacizumab) is the main treatment option, and the second line option is tyrosine kinase inhibitors (TKIs). The treatment option in the terminal stage (BCLC-D) is palliative care [2].
The characteristics of the predominant arterial flow in patients with HCC have justified treatment with intra-arterial therapies, such as TARE with yttrium 90 microspheres (90Y-TARE) as a therapeutic option for HCC. 90Y-TARE has demonstrated clinical efficacy as an alternative treatment for HCC in radiological response and shown adequate safety profile in patients in different stages of the disease [2]. In the early to intermediate stage of HCC, treatment with TARE prolongs the time to progression, which reduces the withdrawal from transplant or surgical resection waiting lists [5, 6]. In the advanced stage of HCC, available evidence (the SARAH [7] and SIRveNIB [8] studies) has determined 90Y-TARE presents an efficacy profile and survival benefit compared to sorafenib. Also, when the combination of 90Y-TARE with sorafenib was evaluated (the SORAMIC study [9]), the toxicity was no greater than sorafenib monotherapy [9].
A recent update of the European Society of Medical Oncology (ESMO) clinical practice guidelines recommends using 90Y-TARE as an alternative treatment in the early and intermediate stages of HCC. The guideline recommends using TARE in exceptional circumstances, patients with diseases limited to the liver or with a good liver function but for whom TACE or systemic therapy is not possible [10]. Two types of microspheres are known to include the beta 90Y emitter: glass (TheraSphere®) [11] and resin (SIR-Spheres®) microspheres [12]. Additionally, there is a third type based on holmium-166 (166Ho, QuiremSpheres®) [13] that was not included in the review due to limited clinical evidence, as indicated by the National Institute for Clinical Excellence (NICE) [14].
In addition to the clinical evidence, economic studies justify the use of new innovative therapies to optimize clinical outcomes in the context of the National Health System (NHS). Given the clinical benefits, limited economic resources, and greater emphasis placed on strengthening healthcare systems, there is an inherent need to generate economic evidence that enhances efficiency and prioritizes the available health resources [15]. Subsequently, a review of the economic benefits of 90Y-TARE in the HCC population needs to be established. Thus, this systematic review aimed to review and summarize the economic evaluations of the use of 90Y-TARE for the treatment of primary hepatic neoplasms, specifically HCC.
Methods
Search strategy and identification of studies
A systematic review of all economic evaluations on TARE for the treatment of HCC and published in Spanish and English was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) methodology [16, 17].
The search strategy was designed using the Population, Intervention, Comparison, Outcomes (PICO) methodology. Also, Boolean operators without limitations and by these criteria: type of study, language, or year of publication (except the limitation of the search of communications to congresses to a 5-year period) were applied. A manual search of the citations of the initially selected articles was performed to identify potentially relevant additional publications. Key search terms included “Hepatocarcinoma”, “Hepatic neoplasms”, “Primary liver tumour”, “Primary liver tumours”, “Liver metastases”, “Secondary liver cancer”, “Hepatocellular carcinoma”, “HCC”, “Intrahepatic cholangiocarcinoma”, “Colorectal metastasis”, “Colorectal metastases”, “Colorectal carcinoma”, “Colorectal neoplasms”, “Colon”, “Neuroendocrine tumours”, “Yttrium-90”, “90Y”, “90-Y”, “Y-90”, “Y90”, “radioembolization”, “transarterial radioembolization”, “transcatheter arterial radioembolization”, “TARE”, “Selective internal radiation therapy”, “SIRT”, “sirtuins”, “TheraSphere”, “SIR-Spheres”, “SIRSpheres”, “Cost”, “Cost utility”, “Cost benefit”, “Cost efficiency”, “Cost analysis”, “Budget impact” and “economic evaluation” (Additional file 1).
Databases were searched for all economic evaluations using 90Y-TARE for hepatic neoplasms published until May 2021. The following electronic databases were explored: Medline through PubMed, Embase, The Cochrane Library, and MEDES; health technology assessment agencies, including the European Network for Health Technology Assessment (EUnetHTA), Network of Health Technology Assessment Agencies (REDETS), and the National Institute for Health and Care Excellence (NICE); and communications from international conferences, including the Cardiovascular and Interventional Radiological Society of Europe (CIRSE), European Conference on Interventional Oncology (ECIO), European Association of Nuclear Medicine (EANM), Society of Interventional Oncology (SIO), International Society for Pharmacoeconomics and Outcomes Research (ISPOR), European Congress of Radiology (ECR) and Society of Nuclear Medicine and Molecular Imaging (SNMMI).
Inclusion and exclusion criteria
Studies that performed an economic evaluation of 90Y-TARE as a single treatment, as a combination treatment, or as part of a treatment sequence, regardless of the line of treatment, disease, or comparator, were considered. Studies that did not comply with the inclusion criteria were excluded. Economic evaluations that did not refer to 90Y-TARE as part of their development or evaluation were excluded. The inclusion and exclusion criteria were first applied to the titles and abstracts of the publications, and the full texts of the selected studies were reviewed.
Data extraction
Two independent authors (NE and IO) executed the search strategy and independently screened all studies. Possible discrepancies after the review were resolved through discussion and consensus among the authors. Data was extracted using a standardized template (reviewed by NE and IO) and the parameters collected include author/s, year and country of publication, type of economic evaluation defined as full (cost-effectiveness-analysis [CEA], cost-utility analysis [CUA], and cost-minimization analysis [CMA]) and partial (cost-analysis [CA] and budget-impact-analysis [BIA]) economic evaluations, perspective, time horizon, type of model, evaluated comparative alternatives, patient characteristics, cost estimation, health outcomes, and cost-effectiveness results. Cost estimates were extracted as reported in the publication, converted to euros (€), and inflated to 2020 (€, 2020) using the reference exchange published by the European Central Bank. Inflation rates were derived from the Organisation for economic co-operation and development (OECD). To eliminate differences in the purchasing power across the different currencies and countries, a purchasing power parity factor (PPP) was performed to convert the costs to international dollars (US$ PPP) [18].
Quality assessment
The methodological quality of the included studies was assessed using the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) checklist [19]. CHEERS includes a 24-item checklist and assigns a score of 1 if the explicit parameters contemplated in the studies were met (“YES”) and a score of 0 if they were not (“NO”). The full (CEA, CUA, and CMA) economic evaluations were evaluated against a 24-item checklist, and the partial (CA and BIA) were evaluated against a 20-item-checklist. This difference was due to the 4 items (items 9, 10, 12, and 21) not being applicable to the study type. An internal classification criterion was developed to assess and categorize the quality of included studies as low (< 50%), medium (50% and 80%), and high (> 80%). The final included studies were independently reviewed by co-authors (NE and IO).
Results
Study selection
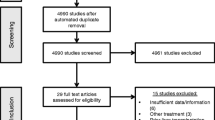
The database search identified 423 studies records, of which 394 were excluded as duplicates or did not meet the inclusion criteria. A total of 29 full-text studies were screened, of which nine studies were excluded due to: metastasis of colorectal cancer (n = 7), metastasis of neuroendocrine tumours of hepatic origin (n = 1), and intrahepatic cholangiocarcinoma (n = 1). Twenty studies met the eligibility criteria. A flow diagram of records founds, screened, selected, and full-text studies evaluated is shown in Fig. 1.

Bibliographic selection based on the PRISMA criteria
Overview of the included studies
Eleven of the 20 studies (55%) were full economic evaluations [20,21,22,23,24,25,26,27,28,29,30] and nine studies (45%) were partial evaluations [31,32,33,34,35,36,37,38,39] (Table 1). Using the CHEERS checklist, the thirteen articles were of high quality (mean score of 94%), and seven abstracts/poster were of lower quality assessment (mean score of 56%), mainly because of the limited breadth of data.
Full economic evaluations (n = 11)
Characteristics of the included studies
Eleven publications were categorized as full economic evaluations (7 articles [20, 22, 23, 26, 28,29,30] and 4 congress communications [21, 24, 25, 27]). Seven were published from a European perspective [22,23,24,25,26, 28, 29] and four from the USA [20, 21, 27, 30]. The HCC population studied were mainly patients with HCC in the intermediate and advanced stages (8 of 11 publications: one BCLC-B [23], four BCLC-C [24, 25, 27, 30], and three grouped stages BCLC-B and BCLC-C [26, 28, 29]); one publication grouped early and intermediate stages [22], and two publications grouped all three stages (BCLC-A, B and C) [20, 21].
Regarding the type of microsphere evaluated, three publications did not specify the type of microsphere [21, 26, 27]; two studies referred to TheraSphere® [22, 24], two studies referred to SIR-Spheres® [25, 29], three studies referred to both types (TheraSphere® and SIR-Spheres®) [20, 23, 30], and one study reported the use of three types of microspheres, including QuiremSpheres® [28]. The main comparators were TACE [20,21,22,23] and sorafenib [24,25,26,27,28,29,30, 30], in addition to transarterial embolization (TAE) [22], TACE with doxorubicin-releasing particles (DEB-TACE) [22] and lenvatinib [28].
Regarding the pharmacoeconomic parameters, two of the eleven studies were CEA [20, 21], eight were ACU [22,23,24, 26,27,28,29,30], and one was a CMA [25]. Six of the eleven studies used a Markov modelling [22,23,24, 26, 27, 30], two studies utilized Monte-Carlo modelling [20, 21], two were survival-based models [28, 29], and one utilized decision trees modelling [28]. The cost minimisation study did not specify the type of model [25] used. The time horizon ranged from 5 years [20, 21, 30] to lifetime [23, 26, 27, 29]. The payer’s perspective predominated (10 of 11 publications), although one study focused on the social perspective [28]. The outcome measures included overall survival (OS), life month gained (LMG), life years gained (LYG), quality-adjusted life years (QALY), incremental cost-effectiveness ratios (ICERs), incremental cost-utility ratios (ICURs), willingness-to-pay (WTP), and incremental net monetary benefit (NMBs). The characteristics of the full economic evaluations are summarized in Table 2.
TARE versus TACE
TACE therapy was one of the comparators considered in four of the eleven studies [20,21,22,23]); two studies [20, 21] compared TARE with TACE, a third study [22] included TACE and two other comparators (TAE and DEB-TACE), and lastly publication reported TACE as part of a sequence of therapies (TARE, TACE and possibly sorafenib [TTS sequence] versus TARE plus sorafenib [TS sequence]) [23]. The stages of the evaluated patients were heterogeneous; early [20,21,22], intermediate [20,21,22,23], and advanced [20, 21] disease.
TARE versus TKI
Seven studies [24,25,26,27,28,29,30] used systemic therapy as a comparator; 6 studies [24,25,26,27, 29, 30] reported only sorafenib as a comparator, and one study [28] included lenvatinib. Additionally, these seven studies evaluated patients with the intermediate-advanced disease.
Results of the full economic evaluations
The costs and health outcomes reported in the eleven studies were heterogeneous (Table 3).
TARE versus TACE
Four studies reported higher costs (TARE versus TACE) [20,21,22], and this finding was independent of the patient's BCLC-A, B, or C in three studies. The fourth publication presented a higher cost in TS sequence therapy than TTS sequence (47% of patients with sorafenib) in patients with the intermediate disease [23].
In one study, the health outcomes reported for patients in the intermediate stage showed a benefit of TARE over TACE in terms of LYG and QALY [22]. The study evaluated sequences of therapies, TTS (with optional sorafenib), and showed a greater incremental benefit than TS for LYG and QALYs [23]. Two studies [20, 21]) reported the benefits for TARE in the advanced stage (BCLC-C), with lower benefits compared to TACE in the early and intermediate stages.
The ICERs of TARE versus TACE presented monthly (LMG) [20] and annual costs (LYG) [22]. Additionally, two studies [22, 23] presented ICUR results (€/QALY), and one study did not present any ratios [21]. For the early and intermediate stages of the disease, one study (Manas et al. [22]) presented an ICER of £ 12,833/LYG (£, 2020) (12,291 $US PPP/LYG) and established the ICUR of TARE versus TACE at £ 17,279/QALY (£, 2020) (17,397 $US PPP/QALY), with a 76.5% probability of being profitable considering a cost-effectiveness threshold of £ 20,000/QALY (£, 2020). In the intermediate stage, one study evaluated two treatment sequences and reported that TTS (with sorafenib in 47% of patients), including TARE, was the dominant strategy (i.e., it offered greater effectiveness with lower associated cost). When compared to TS, an 83% probability of being efficient based on a threshold of € 50,000/QALY was estimated [23]. In the advanced stage, TARE was superior to TACE (ICER 8 $US PPP/LMG) when the intervention was evaluated in one lobe and obtained an ICER of $ 356/LMG ($, 2013) (399 $US PPP/LMG) when the two-lobe intervention was evaluated [20]. TARE was inferior (with lower effectiveness and higher associated cost) when used in the early and intermediate stages [20]. The second publication by Rostambeigi et al. [21] did not detail the calculation of ICERs.
TARE versus TKI
Six [24,25,26, 28,29,30] of the seven studies compared TARE with sorafenib in patients with intermediate-advanced stage and reported lower costs for TARE (differences between 1454 to 46,982 $US PPP). However, Parikh et al. [27] evaluated a similar group of patients and reported conflicting cost results, a difference attributable to the source of the clinical trial efficacy parameters.
The benefits for health outcomes were greater for TARE [24,25,26, 29] than sorafenib in four of the seven studies (maximum QALY gained was 0.540 in BCLC-B, 0.27 in BCLC-C, and 0.601 in both stages); two studies [27, 28] showed greater health benefits for sorafenib (maximum QALY gained was 0.09), and one study [30] reported differing results depending on the source of clinical efficacy.
For patients with advanced-stage, TARE therapy was considered superior to sorafenib in five [24,25,26, 29, 30] of the seven studies when the SARAH RCT clinical parameters were used [7] as the source of clinical efficacy. The remaining two studies [27, 28] reported sorafenib was superior to TARE in patients with intermediate-advanced stage.
Study quality reporting assessment
Included studies categorized as full economic evaluations were appraised for their quality: six of the eleven studies (55%) [22, 23, 26, 28,29,30] had a high score when evaluated with the 24-item checklist (mean compliance: = 99%). Approximately, 27% (3 of 11) and 18% (2 of 11) of the studies had a moderate score (mean compliance: 66%) [20, 25, 27] and a low score (mean compliance of 46%) [21, 24], respectively.
Partial economic evaluations (n = 9)
Characteristics of the included studies
Nine publications were partial evaluations (6 articles [31, 34,35,36,37, 39] and 3 congress communications [32, 33, 38]). Six publications were from the European perspective [31, 33, 36,37,38,39]), two from the United States [34, 35], and one from the Canadian perspective [32]. The HCC population included patients with intermediate and advanced stages in seven of the nine studies [31,32,33, 36,37,38,39]; five studies [31, 32, 36, 37, 39] reported the inclusion of patients as BCLC-B or BCLC-C, and two studies defined the intermediate or advanced stage as unresectable HCC (Muszbek et al.) [33, 38]. Of the two remaining studies, one (Ray et al.) [34] described HCC in a way that can be assumed to correspond to an early BCLC-A stage (male patient 65 years old with unresectable solitary HCC of 3 cm isolated in 1 lobe, not suitable for transplantation), and the second study (Ljuboja et al.) [35] did not define the population.
Three of the nine studies evaluated SIR-Spheres® [31, 35, 39], one included TheraSphere® [32], three considered both TheraSphere® and SIR-Spheres® [36,37,38], and two did not specify the type of microsphere evaluated. The comparators were TACE [31, 32, 34, 35, 38], ablative therapy [34, 35] and systemic therapies (sorafenib [31, 33, 36, 37, 39] and lenvatinib [39]).
Regarding the time horizon, six studies were CA [31, 33,34,35,36, 38] and reported time horizons ranging from 1 month to 2 years. The remaining three studies were BIA [32, 37, 39] and reported time horizons ranging from 3 years to a lifetime horizon. The payer’s perspective was most frequently used (100%); with the exception of one study that considered the social perspective [38]. The HCC stages of the study population, the comparators, and the outcome measures considered in the partial economic evaluations are highlighted in Table 4.
TARE versus TACE
Treatment with TACE was considered as a comparator in five [31,32,33,34,35] of the nine studies. Four of five studies reported the stages of HCC (early [34], intermediate, and/or advanced stages [31,32,33]). In studies of intermediate-stage HCC, one study compared only TACE versus TARE [33], two studies [31, 32] included sorafenib in addition to TACE, and two studies [34, 35] reported including radiofrequency ablation (RFA).
TARE versus TKI
Four studies [36,37,38,39] used systemic therapy as a comparator: three [36,37,38] reported sorafenib as a comparator, while one [39] publication also included lenvatinib in the assessment. All four studies considered patients in the intermediate-advanced stage.
Results of the partial economic evaluations
The costs and health outcomes were heterogeneous, mainly due to the type of economic evaluation performed and the grouping of patients with the different stages of the disease. Aggregated data for intermediate and advanced stages (BCLC-B combined with BCLC-C) were reported in five studies [31, 32, 36, 37, 39]. Data differentiated by HCC stages was reported in three studies (BCLC-A [34], BCLC-B [33], and BCLC-C [38]), and one publication [35] did not report the stage of disease (Table 5).
TARE versus TACE
Four CAs [31, 33,34,35] and one BIA [32] compared TARE versus TACE. The CA studies mostly indicated higher treatment costs (range: 11,572–42,368 $US-PPP) with TARE than with TACE (range: 9577–35,855 $US PPP) treatments [31, 33,34,35], ablative therapy (range: 3790–11,135 $US PPP) [34, 35] or sorafenib (12,460 $US PPP) [31]. However, one study (Muszbek et al.) [33] reported similar costs for TARE and TACE regardless of whether the costs were obtained from the official source (the NHS) or via a micro-costing approach [40]. Furthermore, Colombo et al. [31] highlighted the omission of the costs of unplanned hospitalization and adverse events (AEs) from their assessment. However, Ray et al. [34] established that in the early stage (based on a hypothetical cohort of patients older than 65 years) TARE had lower costs than TACE in more than one-third of the simulations of the evaluated scenarios. The BIA [32] study found cost savings with TARE during 3 consecutive years (savings of 40,699; 64,454, and 82,437 $US PPP at years 1, 2, and 3, respectively) of evaluation in a simulated population of 200 patients in a Canadian hospital.
No health outcomes were reported in the five studies that compared TARE with TACE. However, Colombo et al. [31] evaluated the treatment patterns in four centres in Italy and found TACE as the treatment of choice for intermediate HCC and sorafenib as the most commonly used first-line treatment for advanced HCC.
TARE versus TKI
The cost comparisons of TARE versus TKI (2 CA [36, 38] and 2 BIA [37, 39]) reported dissimilar results for TARE in patients with intermediate and/or advanced-stage disease. The CA by Lucà et al. [36] reported significantly lower cost for TARE (18,096 $US PPP) than sorafenib subgroup (28,520 $US PPP). Besides, the CA by Muszbek et al. [38] identified significant changes in the clinical practices for the management of advanced HCC patients, showing a 54 to 79% decrease in monthly costs compared to previous surveys. The BIA published by Rognoni et al. [37] from the Italian Health perspective was estimated to save € 7 million with the progressive increase in the use of TARE (from 20 to 50%) instead of sorafenib over 5 years. The second BIA (Pollock et al.) [39] evaluated TARE versus without TARE in four European countries (Spain, France, Italy, and the United Kingdom) and reported the use of TARE in Spain would generate a cost savings of 26.5% over a 3-year period.
Within the type of resources used, the pharmacological cost, the work-up, the number of procedures and the management of AEs were identified as cost drivers for TARE and TKIs. Only three [36, 37, 39] of the four studies provided health outcomes in the survival rates [36], the number of events (deaths or hospitalizations) avoided [37], incremental LYG [39], and the proportion of patients receiving treatment with curative intent [39]. The CA by Lucà et al. [36] estimated that TARE had significantly higher medium-term survival rates than sorafenib (TARE 64.1% vs. sorafenib 24.3%; p = 0.012) after 2 years of follow-up of patients with intermediate-advanced HCC. The BIA by Rognoni et al. [37] reported a greater number of deaths avoided (2 and 14 deaths in 5 and 10 years, respectively) and fewer hospital admissions due to hepatic decompensation (32 hospitalizations avoided in 5 years) in the intermediate-advanced stage. The BIA by Pollock et al. [39] reported an incremental LYG of 0.009 with TARE (1.176 LYG) compared to sorafenib (1.168 LYG) and reported that 71 additional patients would benefit from treatment with curative intent over a 3-year period.
Study quality reporting assessment
Approximately six [31, 34,35,36,37, 39] of the nine studies (67%) had a high score when evaluated with a 20-items checklist (mean compliance:93%). The remaining three studies (33%) were rated as having a moderate quality (mean compliance: 62%) [32, 33, 38].
Discussion
This review demonstrates that there is evidence that 90Y-TARE is a potentially cost-effective therapy for the treatment of HCC in the intermediate and advanced stages. 90Y-TARE was associated with lower treatment costs than sorafenib but higher treatment costs when compared to TACE or ablative therapy. However, the BIA conducted in Canada reflects cost savings associated with 90Y-TARE, even when the incremental cost of the device acquisition was considered [32]. Though, studies that compared 90Y-TARE with TACE did not account for AEs (postembolization syndrome) [20, 22], a key cost component and lower repetition rate associated with TARE than with TACE [22, 31].
Health outcomes vary with maximum health benefits associated with TARE when compared with TACE for intermediate- [22] and advanced-stage patients [20, 21] and when compared with sorafenib for intermediate- [26] and advanced-stage patients [24,25,26, 29, 36, 37, 39]. However, the comparison of the effectiveness of TARE versus TACE suggests that TARE may be more beneficial to intermediate HCC as it offers a greater possibility for curative intent in these patients [22]. Similarly, these results suggest that a greater number of patients with advanced HCC can obtain greater clinical benefits from TARE, though at a higher cost [25]. Compared with sorafenib and assuming the same clinical efficacy [24,25,26,27, 29, 30], maximum health benefits could be obtained using TARE, given the lower overall cost of TARE reported in studies [24, 25, 27, 29, 30]. Thus, assuming the same health resources for TARE and sorafenib, a greater number of patients could potentially be treated with TARE than with sorafenib, given the cost savings of TARE [32, 37, 39].
Several strengths to our study exist. To our knowledge, this is the first systematic review of the economic evidence of 90Y-TARE therapy in hepatic neoplasms that included HCC. This review included a strict inclusion criterion focusing on economic evaluations on TARE in liver neoplasms. An extensive search strategy was conducted by performing a search of both English and Spanish studies from the international bibliographic databases with the largest number of indexed publications (Medline and EMBASE) and of a database of publications in Spanish (MEDES). Also, with the goal of identifying the greatest possible number of studies, communications presented at various international conferences were consulted.
Some limitations to our study exist. First, given English and Spanish studies were included in our review, this may lead to excluding other potential economic evaluations published in other languages. As such, there is a potential for publication bias. Second, the diversity of methodologies used and the different parameters such as a variety of sources of clinical efficacy, comparators, and time horizons may limit the external validity of the results. Third, costs were reported for different dates and currencies, or did not report the reference year for cost items collected. Regardless, costs were adjusted to 2020 ($US PPP costs). Also, studies with missing reference years were assumed to be the same as cost reference sources or the study’s publication year. Fourth, the internal evaluation of the study quality varied as the appraisal of the quality of studies showed considerable differences across studies. Given we included conference abstracts (n = 7) with no full-text version available at the time of this review, this limited the analysis and appraisal of the results. Even though some included studies were abstracts, it is important to note that the results showed similarities with other studies with full manuscripts.
Economic outcomes are dependent on pathology management and affect resource consumption during patient HCC management. The development of new systemic therapies in recent years [41], along with the availability of new diagnostic algorithms for HCC [42], could modify clinical practice guidelines due to earlier detection of the pathology. Another relevant issue is the influence of the radiologist's experience with liver images on determining treatment response [43]. Furthermore, personalised dosimetry with 90Y-TARE has shown significant clinical improvement in objective response rate and OS in patients with locally advanced HCC [44]. These parameters are related to resource consumption in clinical practice and may affect the results reported here.
Conclusion
This review suggests that 90Y-TARE contributes to the reduction of hospital resource and therefore reduces costs, improves patient outcomes, and improves the value and efficiency in hospitals. Overall, TARE is a cost-effective short- and long-term treatment for HCC, driven by increased LYG compared to other HCC therapies. Given the evidence highlighted in this review, 90Y-TARE is a cost-effective therapy for treating patients with liver neoplasms or HCC in the intermediate and advanced stages. Since clinical practice guidelines or new therapies could potentially impact these results, we recommend future economic evaluations focusing on 90Y-TARE from different cost perspectives.
Availability of data and materials
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request. The version contains additional information. The additional information of search strategy is in the Additional file 1.
Abbreviations
- AE:
-
Adverse events
- BC:
-
Base case
- BCLC:
-
Barcelona Clinic Liver Cancer
- BIA:
-
Budget-impact-analysis
- CA:
-
Cost-analysis
- CEA:
-
Cost-effectiveness-analysis
- CHEERS:
-
Consolidated Health Economic Evaluation Reporting Standards
- CI:
-
Confidence interval
- CIRSE:
-
Cardiovascular and Interventional Radiological Society of Europe
- CMA:
-
Cost-minimization-analysis
- CT:
-
Clinical trial
- CTT:
-
Conventional transarterial therapy
- CUA:
-
Cost-utility-analysis
- DEB-TACE:
-
Doxorubicin eluting bead transarterial chemoembolization
- EANM:
-
European Association of Nuclear Medicine
- ECIO:
-
European Conference on Interventional Oncology
- ECR:
-
European Congress of Radiology
- ESMO:
-
European Society of Medical Oncology
- EUNetHTA:
-
European Network for Health Technology Assessment
- HCC:
-
Hepatocellular carcinoma
- HTA:
-
Health technology assessment
- ICER:
-
Incremental cost-effectiveness ratio
- ICUR:
-
Incremental cost-utility ratio
- ISPOR:
-
International Society for Pharmacoeconomics and Outcomes Research
- LMG:
-
Life month gained
- LYG:
-
Life years gained
- NHS:
-
National Health System
- NICE:
-
National Institute for Health and Clinical Excellence
- NMB:
-
Net monetary benefit
- OECD:
-
Organization for Economic Co-operation and Development
- OS:
-
Overall survival
- PPP:
-
Purchasing power parity
- PRISMA:
-
Preferred Reporting items for Systematic Reviews and Meta-Analyses
- QALY:
-
Quality-adjusted life year
- REDETS:
-
Network of Health Technology Assessment Agencies
- RFA:
-
Radiofrequency ablation
- SIO:
-
Society of Interventional Oncology
- SNMMI:
-
Society of Nuclear Medicine and Molecular Imaging
- SOR:
-
Subgroup or patients with sorafenib
- TACE:
-
Transarterial chemoembolization
- TAE:
-
Transarterial embolization
- TARE:
-
Transarterial radioembolization
- TDABC:
-
Time-drive activity-based costing
- TS:
-
TARE plus sorafenib
- TTP:
-
Time to progression
- TTS sequence:
-
TARE, TACE and possibly sorafenib
- TKIs:
-
Tyrosine kinase inhibitors
- WTP:
-
Willingness-to-pay
- 90Y-TARE:
-
TARE with yttrium 90 microspheres
References
Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet Lond Engl. 2018;391:1301–14. https://doi.org/10.1016/S0140-6736(18)30010-2.
Reig M, Forner A, Ávila MA, Ayuso C, Mínguez B, Varela M, et al. Diagnosis and treatment of hepatocellular carcinoma. Update of the consensus document of the AEEH, AEC, SEOM, SERAM, SERVEI, and SETH. Med Clin (Barc). 2021;156:463.e1–463.e30. https://doi.org/10.1016/j.medcli.2020.09.022.
World Health Organization. Global Cancer Observatory (GCO). Cancer Today 2020. http://gco.iarc.fr/today/home. Accessed 2 Mar 2022.
Kohn CG, Singh P, Korytowsky B, Caranfa JT, Miller JD, Sill BE, et al. Humanistic and economic burden of hepatocellular carcinoma: systematic literature review. Am J Manag Care. 2019;25:SP61–73.
Salem R, Gordon AC, Mouli S, Hickey R, Kallini J, Gabr A, et al. Y90 radioembolization significantly prolongs time to progression compared with chemoembolization in patients with hepatocellular carcinoma. Gastroenterology. 2016;151:1155–1163.e2. https://doi.org/10.1053/j.gastro.2016.08.029.
Garlipp B, de Baere T, Damm R, Irmscher R, van Buskirk M, Stübs P, et al. Left-liver hypertrophy after therapeutic right-liver radioembolization is substantial but less than after portal vein embolization. Hepatol Baltim Md. 2014;59:1864–73. https://doi.org/10.1002/hep.26947.
Vilgrain V, Pereira H, Assenat E, Guiu B, Ilonca AD, Pageaux G-P, et al. Efficacy and safety of selective internal radiotherapy with yttrium-90 resin microspheres compared with sorafenib in locally advanced and inoperable hepatocellular carcinoma (SARAH): an open-label randomised controlled phase 3 trial. Lancet Oncol. 2017;18:1624–36. https://doi.org/10.1016/S1470-2045(17)30683-6.
Chow PKH, Gandhi M, Tan S-B, Khin MW, Khasbazar A, Ong J, et al. SIRveNIB: selective internal radiation therapy versus sorafenib in Asia-pacific patients with hepatocellular carcinoma. J Clin Oncol. 2018;36:1913–21. https://doi.org/10.1200/JCO.2017.76.0892.
Ricke J, Klümpen HJ, Amthauer H, Bargellini I, Bartenstein P, de Toni EN, et al. Impact of combined selective internal radiation therapy and sorafenib on survival in advanced hepatocellular carcinoma. J Hepatol. 2019;71:1164–74. https://doi.org/10.1016/j.jhep.2019.08.006.
European Society for Medical Oncology (ESMO). Updated treatment recommendations for hepatocellular carcinoma (HCC) from the ESMO Clinical Practice Guidelines. 2021. https://www.esmo.org/guidelines/gastrointestinal-cancers/hepatocellular-carcinoma/eupdate-hepatocellular-carcinoma-treatment-recommendations. Accessed 5 Nov 2021.
Boston Scientific. TheraSphereTM Y-90 glass microspheres 2021. https://www.bostonscientific.com/en-US/products/cancer-therapies/therasphere-y90-glass-microspheres.html. Accessed 2 Dec 2021.
Sirtex. SIR-Spheres® Y-90 resin microsphere 2021. https://www.sirtex.com/eu/clinicians/. Accessed 2 Dec 2021.
Terumo. QuiremSpheres® Microspheres 2021. https://www.terumo-europe.com/en-emea/products/quiremspheres%E2%84%A2-microspheres. Accessed 16 Dec 2021.
National Institute for Clinical Excellence (NICE). Selective internal radiation therapies for treating hepatocellular carcinoma. Guidance. 2021. https://www.nice.org.uk/guidance/ta688. Accessed 16 Dec 2021.
López Bastida J, Oliva J, Antoñanzas F, García-Altés A, Gisbert R, Mar J, et al. A proposed guideline for economic evaluation of health technologies. Gac Sanit. 2010;24:154–70. https://doi.org/10.1016/j.gaceta.2009.07.011.
Moher D, Liberati A, Tetzlaff J, Altman DG, for the PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. https://doi.org/10.1136/bmj.b2535.
Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372: n160. https://doi.org/10.1136/bmj.n160.
Organisation for Economic Cooperation and Development (OECD). Conversion rates—purchasing power parities (PPP). 2020. https://doi.org/10.1787/1290ee5a-en.
Husereau D, Drummond M, Petrou S, Carswell C, Moher D, Greenberg D, et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. Eur J Health Econ HEPAC Health Econ Prev Care. 2013;14:367–72. https://doi.org/10.1007/s10198-013-0471-6.
Rostambeigi N, Dekarske AS, Austin EE, Golzarian J, Cressman EN. Cost effectiveness of radioembolization compared with conventional transarterial chemoembolization for treatment of hepatocellular carcinoma. J Vasc Interv Radiol. 2014;25:1075–84. https://doi.org/10.1016/j.jvir.2014.04.014.
Rostambeigi N, Dekarske A, Austin E, Golzarian J, Cressman E. Simulation study on cost-effectiveness of radioembolization compared with trans-arterial chemoembolization for hepatocellular carcinoma [abstract]. J Vasc Interv Radiol. 2014;25:S104–5. https://doi.org/10.1016/j.jvir.2013.12.292.
Manas D, Bell JK, Mealing S, Davies H, Baker H, Holmes H, et al. The cost-effectiveness of TheraSphere in patients with hepatocellular carcinoma who are eligible for transarterial embolization. Eur J Surg Oncol. 2021;47:401–8. https://doi.org/10.1016/j.ejso.2020.08.027.
Rognoni C, Ciani O, Sommariva S, Tarricone R. Cost-effectiveness analysis of treatments involving radioembolization in intermediate-stage hepatocellular carcinoma. J Comp Eff Res. 2018;7:209–21. https://doi.org/10.2217/cer-2017-0050.
Chaplin S, Taylor M, Lapon J, White J. Economic evaluation of glass yttrium-90 microspheres versus sorafenib for the treatment of advanced hepatocellular carcinoma: cost effectiveness analysis in the United Kingdom. Cardiovasc Intervent Radiol. 2015;38:S279–80.
Palmer D, Ross P, Shah T, Yu D, Shergill S, Patterson K, et al. Cost effectiveness of selective internal radiation therapy (SIRT) with Y-90 resin microspheres versus sorafenib in Barcelona Clinic Liver Cancer (BCLC) stage C hepatocellular carcinoma patients in the UK. Ann Oncol. 2017;28:v239–40. https://doi.org/10.1093/annonc/mdx369.087.
Rognoni C, Ciani O, Sommariva S, Tarricone R. Real-world data for the evaluation of transarterial radioembolization versus sorafenib in hepatocellular carcinoma: a cost-effectiveness analysis. Value Health. 2017;20:336–44. https://doi.org/10.1016/j.jval.2016.09.2397.
Parikh N, Singal A, Kulik L, Hutton D. Cost-effectiveness of sorafenib versus selective internal radiation therapy for patients with advanced hepatocellular carcinoma. Hepatology. 2018;68(Suppl. 1):532A–3A.
Walton M, Wade R, Claxton L, Sharif-Hurst S, Harden M, Patel J, et al. Selective internal radiation therapies for unresectable early-, intermediate- or advanced-stage hepatocellular carcinoma: systematic review, network meta-analysis and economic evaluation. Health Technol Assess. 2020;24:1–264. https://doi.org/10.3310/hta24480.
Muszbek N, Remak E, Evans R, Brennan VK, Colaone F, Shergill S, et al. Cost-utility analysis of selective internal radiation therapy with Y-90 resin microspheres in hepatocellular carcinoma. Future Oncol Lond Engl. 2021;17:1055–68. https://doi.org/10.2217/fon-2020-1004.
Marqueen KE, Kim E, Ang C, Mazumdar M, Buckstein M, Ferket BS. Cost-effectiveness analysis of selective internal radiotherapy with yttrium-90 versus sorafenib in locally advanced hepatocellular carcinoma. JCO Oncol Pract. 2021;17:e266–77. https://doi.org/10.1200/OP.20.00443.
Colombo G, Cammà C, Attili A, Ganga R, Gaeta G, Franzini JM, et al. Patterns of treatment and costs of intermediate and advanced hepatocellular carcinoma management in four Italian centers. Ther Clin Risk Manag. 2015;11:1603. https://doi.org/10.2147/TCRM.S88208.
Hubert MM, Karellis A, Sherman M, Gill S, Beecroft R, Sampalis JS. Beyond budget silos-budget impact analysis of transarterial radioembolization with yttrium-90 glass microspheres for hepatocellular carcinoma from a hospital perspective. Value Health. 2016;19:A308. https://doi.org/10.1016/j.jval.2016.03.671.
Muszbek N, Evans R, Remak E, Brennan V, Colaone F, Shergill S. PCN98 cost-comparison analysis of selective internal radiation therapy (SIRT) and transarterial chemoembolisation (TACE) in unresectable hepatocellular carcinoma (HCC). Value Health. 2019;22:S455. https://doi.org/10.1016/j.jval.2019.09.295.
Ray CE, Battaglia C, Libby AM, Prochazka A, Xu S, Funaki B. Interventional radiologic treatment of hepatocellular carcinoma—a cost analysis from the payer perspective. J Vasc Interv Radiol. 2012;23:306–14. https://doi.org/10.1016/j.jvir.2011.11.016.
Ljuboja D, Ahmed M, Ali A, Perez E, Subrize MW, Kaplan RS, et al. Time-driven activity-based costing in interventional oncology: cost measurement and cost variability for hepatocellular carcinoma therapies. J Am Coll Radiol. 2021;18:S1546144021002945. https://doi.org/10.1016/j.jacr.2021.03.027.
Lucà MG, Nani R, Schranz M, De Giorgio M, Iegri C, Agazzi R, et al. Treatment of hepatocellular carcinoma: a cost analysis of yttrium-90 transarterial radioembolization versus sorafenib. Future Oncol. 2018;14:727–35. https://doi.org/10.2217/fon-2017-0566.
Rognoni C, Ciani O, Sommariva S, Bargellini I, Bhoori S, Cioni R, et al. Trans-arterial radioembolization for intermediate-advanced hepatocellular carcinoma: a budget impact analysis. BMC Cancer. 2018;18:715. https://doi.org/10.1186/s12885-018-4636-7.
Muszbek N, Evans R, Remak E, Brennan VK, Colaone F, Shergill S. Changes ion Health State Costs in Hepatocellular Carcinoma (HCC). ISPOR Int Soc Pharmacoeconomics Outcomes Res n.d. https://www.ispor.org/heor-resources/presentations-database/presentation/euro2019-3119/97618. Accessed 7 Apr 2021.
Pollock RF, Colaone F, Guardiola L, Shergill S, Brennan VK. A cost analysis of SIR-Spheres yttrium-90 resin microspheres versus tyrosine kinase inhibitors in the treatment of unresectable hepatocellular carcinoma in France, Italy, Spain and the UK. J Med Econ. 2020;23:593–602. https://doi.org/10.1080/13696998.2020.1731213.
Drummond M, Sculpher M, Torrance G, O’Brien B, Stoddart G. Methods for the economic evaluation of health care programmes, vol. 54. Oxford: Oxford University Press; 2002.
Granito A, Forgione A, Marinelli S, Renzulli M, Ielasi L, Sansone V, et al. Experience with regorafenib in the treatment of hepatocellular carcinoma. Ther Adv Gastroenterol. 2021;14:175628482110169. https://doi.org/10.1177/17562848211016959.
Renzulli M, Golfieri R. Proposal of a new diagnostic algorithm for hepatocellular carcinoma based on the Japanese guidelines but adapted to the Western world for patients under surveillance for chronic liver disease. J Gastroenterol Hepatol. 2016;31:69–80. https://doi.org/10.1111/jgh.13150.
Tovoli F, Renzulli M, Negrini G, Brocchi S, Ferrarini A, Andreone A, et al. Inter-operator variability and source of errors in tumour response assessment for hepatocellular carcinoma treated with sorafenib. Eur Radiol. 2018;28:3611–20. https://doi.org/10.1007/s00330-018-5393-3.
Garin E, Palard X, Rolland Y. Personalised dosimetry in radioembolisation for HCC: impact on clinical outcome and on trial design. Cancers. 2020;12:1557. https://doi.org/10.3390/cancers12061557.
Acknowledgements
Not applicable
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
All authors provided input into the writing, reviewing and revision of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
NEC and IO, are employees of Pharmacoeconomics & Outcomes Research Iberia (PORIB), a consultancy specialising in economic evaluation of health interventions, which has received private financial support from Boston Scientific in relation to the development of this work, including research, interpretation and writing of the manuscript. ARF has received consultancy and proctor fees from Boston Scientific. ICT has received lecture fee from Sirtex Medical. FMG, DF, JCA, NS, have no relevant financial or non-financial interests to disclose. AW, RB are employees at Boston Scientific Corp. NE, IO has received research support from Boston Scientific.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Terminology of searching strategy in PubMed.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Alonso, J.C., Casans, I., González, F.M. et al. Economic evaluations of radioembolization with Itrium-90 microspheres in hepatocellular carcinoma: a systematic review. BMC Gastroenterol 22, 326 (2022). https://doi.org/10.1186/s12876-022-02396-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12876-022-02396-6