
Abstract
Background
This study aimed to examine the impact of dietary compositions and patterns on nonalcoholic fatty liver disease (NAFLD) morbidity in Japanese men.
Methods
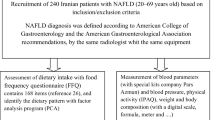
We conducted a cross-sectional study of 281 individuals who underwent comprehensive medical examinations during health screening. Dietary intake was assessed using a semi-quantitative food frequency questionnaire, and factor analysis was performed to detect dietary patterns. NAFLD was diagnosed by the presence of fatty liver on abdominal ultrasonography in nondrinkers (< 30 g/day), and patients were categorized into control (n = 192) and NAFLD groups (n = 89).
Results
Compared with the control group, the NAFLD group consumed fewer mushrooms. Three dietary patterns were identified, namely, a healthy pattern, a western pattern, and a snack pattern. The score of healthy pattern was negatively correlated with the risk of NAFLD. Compared with the lowest tertile of the healthy pattern, the middle tertile was associated with a lower risk of NAFLD after adjusting for age, physical activity, and smoking (odds ratio: 0.47, 95% confidence interval: 0.25–0.91). After further adjustments for body mass index, the middle tertile was associated with a lower risk of NAFLD (odds ratio: 0.46, 95% confidence interval: 0.23–0.92).
Conclusions
A healthy dietary pattern comprising frequent intake of seaweeds, vegetables, mushrooms, pulses, and potatoes and starches was associated with a lower risk of NAFLD in Japanese men. In our opinion, this healthy pattern closely resembles the Japanese Washoku diet, indicating that adherence to Washoku may help prevent NAFLD.
Similar content being viewed by others


Background
Nonalcoholic fatty liver disease (NAFLD) includes several forms of liver diseases, ranging from simple steatosis to nonalcoholic steatohepatitis that can progress to cirrhosis and eventually to hepatocellular carcinoma. NAFLD is regarded as a hepatic phenotype of the metabolic syndrome, and obesity is a well-known major risk factor for NAFLD [1]. Accordingly, increase in the overweight population has caused NAFLD to become one of the most common liver diseases worldwide. Several recent studies estimated the association of NAFLD with economic burden. The latter is expected to increase as the prevalence of obesity and diabetes increases [2, 3]. NAFLD is prevalent in approximately 25% of the global population and in around 10% to 30% of the Japanese population [4,5,6].
Given that obesity is primarily related to dietary composition, several studies have clarified the relationship between diet and NAFLD. Previous studies have shown that lower intake of nutrient-rich and healthy foods (such as foods containing vitamin C, folate, and calcium, as well as vegetables, fruits, dairy products, nuts, and seeds) is associated with a significantly higher risk of developing NAFLD [7, 8]. Currently, dietary intake is mainly evaluated using dietary pattern analysis as this realistically assesses the overall dietary intake of single nutrients and the total dietary impact. Recent studies on NAFLD were also conducted using the dietary pattern analysis [9, 10].
Dietary patterns vary widely among countries. In Japan, the traditional diet is called Washoku. In 2013, the Washoku diet was added to the list of intangible cultural heritages by the United Nations Educational, Scientific and Cultural Organization. “One soup and three dishes” is the basic style of the Washoku diet. Specifically, this style is composed of the dietary staple (rice), soup, and several side dishes [11]. A large variety of foods (especially vegetables, fish, fruits, seaweed, and soybean foods) are consumed because diverse dishes comprise this diet [12]. Moreover, taking small portion sizes of various foods contributes to satiety and helps people to avoid overeating [13]. Thus, the Washoku diet has been noted to be a healthy dietary pattern owing to its low-calorie and well-balanced components [13].
However, despite this healthy diet, the prevalence of NAFLD remains high in Japan. One of the reasons may be the continuous westernization of diet, which is confirmed in Japan [14]. To the best of our knowledge, no study has investigated the association between dietary patterns and NAFLD in Japan. Therefore, this study aimed to investigate the association between dietary patterns and the risk of NAFLD in Japanese men.
Methods
Study design and participants
The participants were 992 Japanese men who underwent comprehensive medical examinations for health screening, including dietary intake assessment. The study was conducted at the Mitsui Memorial Hospital (Tokyo, Japan) between August 2005 and July 2006. Dietary intake was assessed using a food frequency questionnaire (FFQ). Participants with missing data on body measurements, blood biochemical composition, blood pressure, medical history, lifestyle, and dietary intake were excluded. Patients with chronic liver disease and hepatic carcinoma, those positive for the hepatitis B or C virus, or those who consumed > 30 g/day ethanol equivalent of alcohol were also excluded. Ultimately, 281 participants were included in the analysis. They were categorized into two groups, according to the presence of NAFLD: the control group (n = 192) and the NAFLD (n = 89) group.
Clinical and laboratory assessments
All participants underwent an anthropometric assessment, as well as laboratory and radiological tests using standard methods. Information obtained included body mass index (BMI), body fat percentage, aspartate aminotransferase (AST), alanine aminotransferase (ALT), gamma-glutamyl transpeptidase (γ-GTP), total cholesterol (T-CHO), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), triglyceride (TG), systolic and diastolic blood pressure (SBP, DBP), fasting blood sugar (FBS), and hemoglobin A1c (HbA1c). Liver function was evaluated according to levels of high AST, ALT, γ-GTP, T-CHO, LDL-C, and TG in addition to the level of low HDL-C. Medical history, including hypertension and diabetes, and lifestyle, including physical activity and smoking behavior, were assessed using a self-administered questionnaire at the health screening. Participants’ levels of total physical activity were evaluated by determining the metabolic equivalent (MET) hours/day (METs score), which was calculated by multiplying the time spent on activities (/day) by MET intensity: walking slowly (2.0), walking quickly (4.0), light to moderate exercise (5.0), and strenuous exercise (7.0) for leisure-time physical activity [15]. The participants’ smoking behavior was categorized as follows: non-smoker, past smoker, and current smoker.
Assessment of dietary intake and patterns
Food and beverage consumption were assessed using a validated semi-quantitative FFQ [16, 17] that comprised 138 food and beverage items, and usual consumption of the listed foods during the past year was also evaluated. Frequency responses consisted of nine options: less than once per month, 1–3 times per month, 1–2 times per week, 3–4 times per week, 5–6 times per week, once per day, 2–3 times per day, 4–6 times per day, and 7 or more times per day. Further, standard portion sizes were assessed for each food item with three choices: medium (standard), small (50% or less), and large (not less than 150%). Factor analysis (i.e., the principal factor method) was then performed to determine participants’ dietary patterns from 20 food groups in the FFQ. The factors identified were rotated using promax rotation. Eigenvalues and scree plots were used to decide which factors remained. Only foods with a factor loading ≥|0.35| were included in this study. The dietary patterns were classified on the basis of interpretation of foods with high factor loadings for each dietary pattern. The factor scores for each dietary pattern were calculated for each of the participants by summing intakes of food items weighted by their factor loadings. We also categorized the participants as per adherence to each dietary pattern (based on the tertiles of the dietary pattern scores) into low, medium, and high adherence groups.
Assessment of fatty liver
Fatty liver was diagnosed using abdominal ultrasonography by experienced medical technologists or physicians, blinded to any relevant clinical information. NAFLD was diagnosed by the presence of fatty liver in nondrinkers (i.e., < 30 g/day) [18]. The median values (interquartile range [IQR]) of the ethanol equivalent of alcohol were 9.4 (0–20.0) and 0 (0–15.7) in the control and NAFLD groups, respectively.
Statistical analysis
For clinical and dietary data, between-group comparisons were performed using the Mann–Whitney test for continuous variables and the chi-square test for categorical variables. Associations between the dietary compositions or patterns and NAFLD were estimated from odds ratios (ORs) and 95% confidence intervals (CIs) using multiple logistic regression analysis. Dietary patterns were generated using factor analysis. Energy and nutrient intakes by tertile of dietary patterns were compared using the Kruskal–Wallis test. All statistical analyses were performed using SPSS version 22 (IBM Corp., Armonk, NY, USA). P < 0.05 was considered to indicate statistical significance. The minimum number of participants required was determined by power analysis (A post hoc power analysis, G*power, Version 3.1.9.2 and sample size calculation for logistic regression [19]). A total of 281 participants were included in the data analysis.
Results
Compared with the control group, the NAFLD group showed higher BMI, body fat percentage, SBP, DBP, FBS, and HbA1c, as well as worse liver function. However, there were no differences in levels of physical activity and total energy intake between the two groups. The clinical characteristics of the control and the NAFLD groups are shown in Table 1.
Table 2 shows the dietary intake by food group as assessed using the FFQ. The NAFLD group consumed significantly fewer mushrooms (control: 6.5 (3.8–11.7) g/day; NAFLD: 4.4 (3.0–6.4) g/day; P < 0.01). There were no significant differences in relation to the other food group.
To investigate the dose-dependent effect of mushrooms, we classified participants into four groups according to the quartile of mushrooms intake. The multivariate OR value for mushrooms intake is shown in Table 3. Compared to the highest quartile (Q4), mushroom intake in the lowest quartile (Q1) was significantly associated with a higher risk of NAFLD after adjusting for age, physical activity, and BMI (OR: 3.36, 95% CI: 1.47–7.66). As mushroom intake decreases (Q2, Q1), the inverse association between mushroom consumption and NAFLD was increased.
Three dietary patterns were identified by factor analysis, namely a healthy dietary pattern, a western dietary pattern, and a snack pattern (Table 4). The healthy dietary pattern was characterized by frequent intake of seaweeds, vegetables, mushrooms, pulses, and potatoes and starches. The western dietary pattern comprised fats and oils, meat, and seasonings and spices. The snack dietary pattern comprised sugars and starches, luxury beverages (tea, coffee, fruit juice, soft drinks, among other drinks.), and fruits. The proportion of total variance explained by the three dietary patterns was 37.8%.
Table 5 shows the associations between dietary patterns and the risk of NAFLD. The score of healthy pattern was negatively correlated with NAFLD. As compared with the lowest tertile of the healthy pattern, the middle tertile was associated with a lower risk of NAFLD after adjusting for age, physical activity, and smoking (OR: 0.47, 95% CI: 0.25–0.91). After further adjustments for BMI, the middle tertile was associated with a lower risk of NAFLD (OR: 0.46, 95% CI: 0.23–0.92). However, the highest tertile of the healthy pattern showed no significant association. There was also no significant association between other dietary patterns and NAFLD.
Energy and nutrient intakes by tertile of healthy patterns are shown in Table 6. The group with the highest dietary pattern scores (T3) showed higher energy and nutrient intake than other groups.
Discussion
Evidence of the association between dietary patterns and NAFLD in Japan is limited. In this study comprising adult Japanese men, we found three dietary patterns, namely, healthy, western, and snack patterns. The score of healthy dietary pattern, which included a high intake of vegetables, seaweeds, mushrooms, pulses, and potatoes and starches, was associated with a lower risk of NAFLD. To the best of our knowledge, this is the first study to evaluate associations between dietary pattern and NAFLD risk in Japanese men.
Our result corresponds to the previous findings that a dietary pattern consisting of high vegetable intake was associated with a decreased risk of NAFLD [9, 10, 20, 21]. The association between dietary pattern and NAFLD has been reported in various countries. In a Chinese study, the grains-vegetables pattern, characterized by high intake of vegetables, tubers, and mushrooms, was associated with a lower prevalence of NAFLD [21]. Similarly, in a Brazilian study [22] a healthy dietary pattern, composed of fruit, greens and vegetables, and margarine, was inversely associated with the prevalence of NAFLD. Furthermore, in a Greek study, there is a negative correlation between an unsaturated fatty acid dietary pattern and the risk of developing NAFLD [23]. A recent Korean study also reported that a simple meal pattern, characterized by a high intake of fruits, eggs, dairy products, and nuts, was inversely correlated with NAFLD [9]. Moreover, in that study, the traditional dietary pattern, characterized by a high intake of green vegetables, fish, mushrooms, fermented soybeans, and seaweed, was associated with an increased risk of NAFLD. This is in contrast to the findings of the current study and other previous studies. This could be because a traditional Korean diet features several kinds of high-salt foods such as kimchi and doenjang. Accordingly, another study of a Korean population reported that a high-salt dietary pattern was associated with an increased risk of NAFLD [24]. Therefore, high-salt intake may have a stronger effect on the risk of NAFLD than vegetable and mushroom intake. In present study, the group with the highest score of healthy pattern (T3) had high-salt intake, which could be the reason the risk of NAFLD was not attenuated in this group.
The NAFLD group in the current study consumed a low amount of mushrooms, and individuals in the lowest quartile of mushroom consumption was associated with a higher risk of NAFLD than individuals in the highest quartile after adjusting for age, physical activity, and BMI. Mushrooms contain many nutritional components such as dietary fibers, vitamins (e.g. vitamin D, niacin), minerals and polyphenols [25]. Bacteria that live in the intestines convert insoluble dietary fiber ferment to short chain fatty acids, such as butyrate. Short chain fatty acids play an important role in gluconeogenesis; therefore, they affect the development of NAFLD. A previous study demonstrated that butyrate may relieve inflammation and could be associated with lower prevalence of NAFLD [26]. Vitamin D has anti-inflammatory and anti-fibrotic effects [27]. Niacin inhibits fatty acid flux from adipose tissue to liver, reduces hepatic triglyceride synthesis and increases hepatic lipid oxidation [28]. Mushrooms provide antioxidants and anti-inflammatory agents, such as minerals, polyphenols, vitamins and polysaccharides [29, 30]. Those nutrients could protect from oxidative stress and inflammation, which are major risk factors of NAFLD [31, 32]. Animal experiments showed that mushrooms might have a protective benefit against NAFLD [33, 34]. Gil-Ramirez et al. reported that ergosterol-enriched extracts from mushrooms (doses were calculated taking into account the hypocholesterolemic minimal daily intake of plant sterols recommended by European Food Safety Authority) lowered hepatic triglyceride levels and modified the mRNA expression of cholesterol-related genes, thereby making them useful for limiting hepatic steatosis and preventing NAFLD [33]. Drori et al. also suggested that vitamin-D-enriched mushroom extracts were associated with significant attenuation of the rate of total body fat accumulation, along with a decrease in hepatic fat content, and had a protective effect against NAFLD [34]. Mushrooms contain vitamin D and insoluble dietary fiber abundantly. Collectively, these findings indicate that mushrooms may delay or prevent the development of NAFLD in humans also. A recent Chinese study has shown that higher mushroom intake was significantly associated with lower prevalence of NAFLD among Chinese adults [35]. This result is in agreement with our result. Further human researches are needed to validate these results.
Mushrooms (e.g., Lentinula edodes, Flammulina velutipes, and Hypsizygus marmoreus) are often used in the Japanese diet of Washoku in which they are often cooked along with other vegetables and seaweeds. High intake of mushrooms is considered an indicator of a healthy diet. The healthy pattern in the present study appears to resemble the ichiju-sansai (one soup and three side dishes) pattern of Washoku, suggesting that following the Washoku diet can help prevent NAFLD in Japanese men. However, the healthy pattern was associated with a decreased risk of NAFLD, and the effect was lost when a high amount of food was consumed regardless of whether it was a healthy diet. The risk of NAFLD was not attenuated in the highest tertile of food consumption within the healthy pattern, possibly because of the high energy and total fat intake (Table 6). This indicates that even a healthy diet should include consumption of food only in appropriate amounts.
Our study had some limitations. First, this study used a cross-sectional design. Thus, causal relations between dietary patterns and NAFLD could not be investigated. Long-term dietary data are needed to determine this relationship. Second, dietary, exercise and smoking behaviors were determined using self-reported questionnaires, which could be influenced by subjects’ biases, including under- and over-reporting. Third, we used only physical activity data for leisure-time. Participants’ physical activity for occupational work was unclear. Finally, NAFLD was diagnosed using ultrasonography instead of the gold standard method of liver biopsy. However, this ultrasonography is the optimal method for NAFLD diagnosis in the healthy population, as it is non-invasive. Despite these limitations, our study remains valuable, and to the best of our knowledge this is the first study to investigate the impact of dietary patterns on NAFLD among Japanese men. Further studies are needed to clarify our findings.
Conclusions
The score of healthy dietary pattern composed of mushrooms, vegetables, and seaweeds was associated with a decreased risk of NAFLD in Japanese men. The components of healthy dietary pattern (seaweeds, vegetables, and soybean foods) are often used in Washoku. Therefore, we believe that this healthy pattern closely resembles the diet of Washoku, which indicates that Washoku may help prevent or delay NAFLD in Japanese men. Furthermore, dietary counseling which includes recommendations for appropriate salt consumption should be implemented.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ALT:
-
Alanine aminotransferase
- AST:
-
Aspartate aminotransferase
- BMI:
-
Body mass index
- CI:
-
Confidence intervals
- DBP:
-
Diastolic blood pressure
- FBS:
-
Fasting blood sugar
- FFQ:
-
Food frequency questionnaire
- γ-GTP:
-
Gamma-glutamyl transpeptidase
- HbA1c:
-
Hemoglobin A1c
- HDL-C:
-
High-density lipoprotein cholesterol
- IQR:
-
Interquartile range
- LDL-C:
-
Low-density lipoprotein cholesterol
- MET:
-
Metabolic equivalent
- NAFLD:
-
Nonalcoholic fatty liver disease
- OR:
-
Odds ratio
- SBP:
-
Systolic blood pressure
- T-CHO:
-
Total cholesterol
- TG:
-
Triglycerides
References
Abenavoli L, Milic N, Di Renzo L, Preveden T, Medić-Stojanoska M, De Lorenzo A. Metabolic aspects of adult patients with nonalcoholic fatty liver disease. World J Gastroenterol. 2016;22:7006–16.
Younossi ZM, Blissett D, Blissett R, Henry L, Stepanova M, Younossi Y, et al. The economic and clinical burden of nonalcoholic fatty liver disease in the United States and Europe. Hepatology. 2016;64:1577–86.
Estes C, Anstee QM, Arias-Loste MT, Bantel H, Bellentani S, Caballeria J, et al. Modeling NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016–2030. J Hepatol. 2018;69:896–904.
Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64:73–84.
Kojima S, Watanabe N, Numata M, Ogawa T, Matsuzaki S. Increase in the prevalence of fatty liver in Japan over the past 12 years: analysis of clinical background. J Gastroenterol. 2003;38:954–61.
Eguchi Y, Hyogo H, Ono M, Mizuta T, Ono N, Fujimoto K, et al. Prevalence and associated metabolic factors of nonalcoholic fatty liver disease in the general population from 2009 to 2010 in Japan: a multicenter large retrospective study. J Gastroenterol. 2012;47:586–95.
Han JM, Jo AN, Lee SM, Bae HS, Jun DW, Cho YK, et al. Associations between intakes of individual nutrients or whole food groups and non-alcoholic fatty liver disease among Korean adults. J Gastroenterol Hepatol. 2014;29:1265–72.
Ferolla SM, Ferrari TC, Lima ML, Reis TO, Tavares WC Jr, Couto OF, et al. Dietary patterns in Brazilian patients with non-alcoholic fatty liver disease: a cross-sectional study. Clinics. 2013;68:11–7.
Chung GE, Youn J, Kim YS, Lee JE, Yang SY, Lim JH, et al. Dietary patterns are associated with the prevalence of nonalcoholic fatty liver disease in Korean adults. Nutrition. 2019;62:32–8.
Liu X, Peng Y, Chen S, Sun Q. An observational study on the association between major dietary patterns and non-alcoholic fatty liver disease in Chinese adolescents. Medicine. 2018;97:17(e0576).
Suzuki N, Goto Y, Ota H, Kito K, Mano F, Joo E, et al. Characteristics of the Japanese diet described in epidemiologic publications: a qualitative systematic review. J Nutr Sci Vitaminol. 2018;64:129–37.
Yui I, Yu S, Saeko S, Yui M, Kazushi Y, Tatsuya S, et al. Identification of characteristic components and foodstuffs in healthy Japanese diet and the health effects of a diet with increased use frequency of these foodstuffs. Mol Nutr Food Res. 2017;61:12(1700430).
Gabriel AS, Ninomiya K, Uneyama H. The role of the Japanese traditional diet in healthy and sustainable dietary patterns around the world. Nutrients. 2018;10:173.
Murakami K, Livingstone MBE, Sasaki S. Thirteen-year trends in dietary patterns among Japanese adults in the National Health and Nutrition Survey 2003–2015: continuous westernization of the Japanese diet. Nutrients. 2018;10:994.
Solovev A, Watanabe Y, Kitamura K, Takahashi A, Kobayashi R, Saito T, et al. Total physical activity and risk of chronic low back and knee pain in middle-aged and elderly Japanese people: the Murakami cohort study. Eur J Pain. 2020;24:863–72.
Tsubono Y, Takamori S, Kobayashi M, Takahashi T, Iwase Y, Iitoi Y, et al. A data-based approach for designing a semiquantitative food frequency questionnaire for a population-based prospective study in Japan. J Epidemiol. 1996;6:45–53.
Takachi R, Ishihara J, Iwasaki M, Hosoi S, Ishii Y, Sasazuki S, et al. Validity of a self-administered food frequency questionnaire for middle-aged urban cancer screenees: comparison with 4-day weighed dietary records. J Epidemiol. 2011;21:447–58.
Sanyal AJ, Brunt EM, Kleiner DE, Kowdley KV, Chalasani N, Lavine JE, et al. Endpoints and clinical trial design for nonalcoholic steatohepatitis. Hepatology. 2011;54:344–53.
Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49:1373–9.
Fakhoury-Sayegh N, Younes H, Heraoui GNHA, Sayegh R. Nutritional profile and dietary patterns of Lebanese non-alcoholic fatty liver disease patients: a case–control study. Nutrients. 2017;9:1245.
Yang CQ, Shu L, Wang S, Wang JJ, Zhou Y, Xuan YJ, et al. Dietary patterns modulate the risk of non-alcoholic fatty liver disease in Chinese adults. Nutrients. 2015;7:4778–91.
Adriano LS, Sampaio HA, Arruda SP, Portela CL, de Melo MLP, Carioca AA. Healthy dietary pattern is inversely associated with non-alcoholic fatty liver disease in elderly. Br J Nutr. 2016;115:2189–95.
Kalafati IP, Borsa D, Dimitriou M, Revenas K, Kokkinos A, Dedoussis GV. Dietary patterns and non-alcoholic fatty liver disease in a Greek case-control study. Nutrition. 2019;61:105–10.
Choi Y, Lee JE, Chang Y, Kim MK, Sung E, Shin H, et al. Dietary sodium and potassium intake in relation to non-alcoholic fatty liver disease. Br J Nutr. 2016;116:1447–56.
Valverde ME, Hernandez-Perez T, Paredes-Lopez O. Edible mushrooms: improving human health and promoting quality life. Int J Microbiol. 2015;2015:376387.
Xia Y, Zhang S, Zhang Q, Liu L, Meng G, Wu H, et al. Insoluble dietary fibre intake is associated with lower prevalence of newly-diagnosed non-alcoholic fatty liver disease in Chinese men: a large population-based cross-sectional study. Nutr Metab. 2020;17:4.
Romero-Gómez M, Zelber-Sagi S, Trenell M. Treatment of NAFLD with diet, physical activity and exercise. J Hepatol. 2017;67:829–46.
Linder K, Willmann C, Kantartzis K, Machann J, Schick F, Graf M, et al. Dietary niacin intake predicts the decrease of liver fat content during a lifestyle intervention. Sci Rep. 2019;9:1303.
Kozarski M, Klaus A, Jakovljevic D, Todorovic N, Vunduk J, Petrovic P, et al. Antioxidants of edible mushrooms. Molecules. 2015;20:19489–525.
Muszynska B, Grzywacz-Kisielewska A, Kala K, Gdula-Argasinska J, et al. Anti-inflammatory properties of edible mushrooms: a review. Food Chem. 2018;243:373–81.
Masarone M, Rosato V, Dallio M, Gravina AG, Aglitti A, Loguercio C, et al. Role of oxidative stress in pathophysiology of nonalcoholic fatty liver disease. Oxid Med Cell Longev. 2018;2018:9547613.
Tyrovolas S, Panagiotakos DB, Georgousopoulou EN, Chrysohoou C, Skoumas J, Pan W, et al. The anti-inflammatory potential of diet and nonalcoholic fatty liver disease: the ATTICA study. Ther Adv Gastroenterol. 2019;12:1–11.
Gil-Ramírez A, Caz V, Martin-Hernandez R, Marín FR, Largo C, Rodríguez-Casado A, et al. Modulation of cholesterol-related gene expression by ergosterol and ergosterol-enriched extracts obtained from Agaricus bisporus. Eur J Nutr. 2016;55:1041–57.
Drori A, Rotnemer-Golinkin D, Avni S, Drori A, Danay O, Levanon D, et al. Attenuating the rate of total body fat accumulation and alleviating liver damage by oral administration of vitamin D-enriched edible mushrooms in a diet-induced obesity murine model is mediated by an anti-inflammatory paradigm shift. BMC Gastroenterol. 2017;17:130.
Zhang S, Gu Y, Lu M, Fu J, Zhang Q, Liu L, et al. Association between edible mushroom intake and the prevalence of newly diagnosed non-alcoholic fatty liver disease: results from the TCLSIH Cohort Study in China. Br J Nutr. 2020;123:104–12.
Acknowledgements
We thank all the staff of the Mitsui Memorial Hospital for their outstanding support.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
CN contributed to the study conceptualization, formal analysis and writing-original draft. LX contributed to the study formal analysis and writing-review and editing. YI, RK and SM contributed to the study writing-review and editing. YY contributed to the study data curation and resources. TK contributed to the study project administration and supervision. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures used in this research were approved by the Ethical Committee of Kumamoto University (No. 324; March 31, 2016), and written informed consent was obtained from all subjects for publication of this information. This research was conducted in accordance with the stipulations of the Declaration of Helsinki for experiments involving humans.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Nakashita, C., Xi, L., Inoue, Y. et al. Impact of dietary compositions and patterns on the prevalence of nonalcoholic fatty liver disease in Japanese men: a cross-sectional study. BMC Gastroenterol 21, 342 (2021). https://doi.org/10.1186/s12876-021-01919-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12876-021-01919-x