
Abstract
Background
An English version of the Patient Perception of Patient-Centeredness (PPPC) scale was recently revised, and it is necessary to test this instrument in different primary care populations.
Aim
This study aimed to assess the validity and reliability of a Chinese version of the PPPC scale.
Design
A mixed method was used in this study. The Delphi method was used to collect qualitative and quantitative data to address the content validity of the PPPC scale by calculating the Content Validity Index, Content Validity Ratio, the adjusted Kappa, and the Item Impact Score. Confirmatory factor analysis (CFA) and exploratory factor analysis (EFA) were used to assess the construct validity of the PPPC scale through a cross-sectional survey. The internal consistency was also assessed.
Setting/participants
In the Delphi consultation, seven experts were consulted through a questionnaire sent by email. The cross-sectional survey interviewed 188 outpatients in Guangzhou city and 108 outpatients in Hohhot City from community health service centers or stations face-to-face.
Results
The 21 items in the scale were relevant to their component. The Item-level Content Validity Index for each item was higher than 0.79, and the average Scale-level content validity index was 0.97 in each evaluation round. The initial proposed 4-factor CFA model did not fit adequately. Still, we found a 3-factor solution based on our EFA model and the validation via the CFA model (model fit: \({\chi }^{2}=294.573\), P < 0.001, RMSEA = 0.044, CFI = 0.981; factor loadings: 0.553 to 0.888). Cronbach's α also indicated good internal consistency reliability: The overall Cronbach's α was 0.922, and the Cronbach's α for each factor was 0.851, 0.872, and 0.717, respectively.
Conclusions
The Chinese version of the PPPC scale provides a valuable tool for evaluating patient-centered medical service quality.
Similar content being viewed by others


What is already known about the topic?
Using the patient-centered clinical method conceptual framework to assess the quality of the patient-clinician relationship may improve patient-centered care quality in communication and shared decision-making.
However, no valid patient-centered care scale is yet available for use in primary healthcare settings in China.
What this paper adds
The Chinese version of the PPPC scale demonstrated rigorous validity and reliability of three distinct factors and covered the four components under the patient-centered clinical method conceptual framework.
Implications for practice, theory, or policy
The Chinese version of the Patient Perception of Patient-Centeredness scale is valuable for evaluating patient-centered medical service quality.
This leading study bridges the evidence gap in measuring patient-centered care quality in China.
Introduction
Patient-centered care is one of the components of the quality of care defined by the Institution of Medicine (IOM) [1]. The quality of patient-centered care improvement has been associated with various positive health system outcomes, such as effectively enhanced patient satisfaction, improved health-related outcomes(e.g., improvement of symptoms), reduced avoidable referrals, and diagnostic costs [2,3,4,5,6]. If the provider bridges the gap between clinical quality and patient perception, it could improve medical utilization and clinical quality [7]. Mohammed's systematic review found that patients can perceive ten domains of patient-centered care quality (communication, access, shared decision-making, provider knowledge and skills, physical environment, patient education, electronic medical record, pain control, discharge process, and preventive services) [8]. When doctors provide better doctor-patient communications, patients would experience more patient-centered care from doctors, and the reciprocal trust between doctors and patients may improve the effectiveness of treatment plans and, ultimately, clinical outcomes [9]. Therefore, the evaluation of patient-centered care quality can be constructed to focus on communication, accessibility, and quality [10].
The Patient-Centered Clinical Method (PCCM) [11] is most frequently cited in family medicine, [2] which has been used as a guide for practitioners working to improve the quality of patient-centered care that they deliver to patients through enhanced communication skills [9, 12]. Little et al.’s study showed that over 77% (599 out of 781 consecutive patients in the waiting room of three doctors’ surgeries) of patients endorsed and had expectations of care that were the elements of patient-centered care [11, 13]. According to the PCCM, patient-centered concepts incorporate four interactive components used in the setting of primary care [11]: 1) exploring health, disease, and the illness experience, 2) finding common ground, 3) understanding the whole person, and 4) enhancing the patient-clinician relationship. These four components also encompassed patient-clinician relationship aspect quality: communication and shared design making [8]. Hence, existing literature acknowledged that using the PCCM conceptual framework to assess the quality of the patient-clinician relationship may improve patient-centered care quality in communication and shared decision-making. However, in low- and middle-income countries, due to limited time and human resources, [14] providers are more likely to focus on improving clinical and health system quality to enhance patient-centered care quality rather than pay attention to patient perspective.
Currently, no valid patient-centered care scale is available for use in primary healthcare settings in low- and middle-income countries [2, 12]. Developed based on the PCCM conceptual framework [11], the Patient Perception of Patient-Centeredness (PPPC) scale was widely used in many countries in different patient groups and healthcare settings to assess patient-centered care quality [4,5,6, 9, 15,16,17,18,19,20]. Most of the patient-centered care scales reflected only two or three of the four commonly used domains [2]. In the latest version, Ryan et al. revised the PPPC scale to reflect the four widely used domains of the clinicians' interactive activities in primary care settings. This revised PPPC scale was used to assess patient-centered care characteristics and a practical tool for providers to improve their interactions with patients for patient-centered care practice improvements [9]. In this study, we chose a 21-item PPPC scale which contained 18 items from the Ryan et al. version and three items from the original 14-item version [5] that were not included in the revised version to conduct the content validity and construct validity assessment to reflect the quality of patient-centered care in public health care settings more comprehensively.
Methods
Study design and procedures
This study was separated into four stages (Fig. 1) and used a mixed method. In stage one, three working groups were set up to prepare the scale localization and validation processes. In stage two, the scale development group translated the 21-item PPPC-R scale into Chinese and conducted two rounds of face-to-face outpatient interviews to complete the face validity assessment. The outpatients were invited directly by asking for their participation willingness in the outpatient waiting room. We also conducted a round translate back process to refine the scale. In the third stage, we invited seven experts from different disciplines, including one medical psychologist, one general practitioner, one public health physician, two epidemiologists, and two health management panelists, who evaluated the scale's content validity through online questionnaires sent by email separately. The researchers invited these experts through their work net. In the fourth stage, we followed the cross-cultural adaptation process [21, 22] and the COnsensus-based Standards for the selection of health Measurement INstrument (COSMIN) guideline [23] to conduct our study. The detailed scale localization validation procedures were presented in Additional file 1: Appendix 1, including both qualitative and quantitative approaches.

Procedures of PPPC-CN scale localization and validation
Settings, sampling, and investigate processes
For construct validity evaluation and internal consistency reliability, the sample size needs to be 10 times the number of items. Therefore, at least 210 respondents were needed [24]. We estimated a 90% response rate to account for potential non-response. Therefore, 223 respondents were needed. By using convenience sampling in urban and suburban regions in Guangzhou and Hohhot cities, seven community health service centers were selected (institutions’ list presented in Additional file 1: Appendix 2). From July 20 to 26, 2019, the outpatients visited the internal medical physicians or general practitioners in selected community health service centers, and those aged≥18 years were eligible. Anyone with hearing or language impairment was excluded. When the participants left the consultation room, our investigator asked about their willingness to participate in our survey. If they were willing to participate after our investigator informed the content of the informed consent, they would be enrolled in our study. After they finished the survey, we provided them with a towel as a gift(cost RMB 5 yuan) and thanked their participation. Our investigators used a REDCap [25] based online form to complete the one-to-one, face-to-face survey.
Statistical analysis
The Content Validity Index (I-CVI), Content Validity Ratio (CVR), the adjusted Kappa, and the Item Impact Score (IIS) were used to assess the content validity [26]. Because the item in PPPC-R was designed under the PCCM conceptual framework [5], we used confirmatory factor analysis (CFA) to test whether the proposed four domains, which were 1) exploring health, disease, and the illness experience, 2) finding common ground, 3) understanding the whole person, and 4) enhancing the patient-clinician relationship could be imposed as a 4-factor CFA model by using our sample. Suppose this structure does not fit the data well. In that case, we would then use the exploratory factor analysis (EFA) to 1) identify the number of factors and 2) determine which item corresponds to each factor. The CFA model and EFA model were tested using Mplus Version 7.0 with the weighted least squares means and variance (WLSMV) estimator to account for the categorical, ordinal nature of the items and the fact that distributions of the item responses were skewed [27]. The number of factors was determined by the characteristic roots (≥ 1) or the cumulative explained variance (≥ 50%). The scree plot was also used as a guide to choose the number of factors. A threshold factor loading greater than 0.30 was used to decide to accept an item as belonging to a factor [28]. If one item was loaded into two factors in the EFA model, the one with a higher loading value would be chosen [27]. The following model fit indices and their criteria were used to determine the best model [24, 29]: -comparative fit index (CFI) greater than 0.90; α the Turker Lewis Index (TLI) greater than 0.90; β approximate error root mean square (RMSEA) and its 90% confidence interval, RMSEA less than 0.06 indicates good; χchi-square/degree of freedom (χ2/df) less than 3.0. The Cronbach's α consistency coefficient was calculated to determine the scale's internal consistency as a whole and each factor, respectively [30, 31]. For the whole scale and sub-domain of the scale, we calculate Cronbach's α. When a value of more than 0.7 was acceptable [27]. Response patterns were also presented, which were the proportion of each item's different choices. The item has better discrimination when the item has endorsement rates between 0.2 and 0.8 [27].
Descriptive statistics were performed by SPSS 22.0 to assess the general participant characteristics. Means and variances were adopted to describe normal distribution data. Medians and quartiles were used to describe non-normally distributed data. The group difference was tested using the t-test or ANOVA for normally distributed data, and the Wilcoxon rank-sum test or Kruskal–Wallis test for non-normally distributed data; P ≤ 0.05 indicates statistical significance.
Results
Adaptation and content validation
In stage 2, after translation, researchers launched two rounds of interviews to contextualize the PPPC-CN scale. Seven outpatients were willing to accept face-to-face interviews to complete the scale-v1 or scale-v3 and provide their opinions of their understanding of each item at public healthcare institutions in Guangzhou and Hohhot City. The main changes made on the scale-v4 were based on feedback from eight outpatients in the second round of interviews, and the researcher revised the scale consistently and achieved the initial localization of the scale, that is, the item expressing and connotation in Mandarin matched local health system and service and context. Revision details are presented in Additional file 1: Appendix 3.
Seven experts and seven outpatients participated in the content validation and face validation consultations. The results of the offline independent assessment of the validation of the scale by Delphi panelists and target users (outpatients) in stage 3 are presented in Table 1. In both rounds of content validity assessment, the I-CVI for each item was more than 0.79, and the S-CVI/AVE was 0.97 in each evaluation round. The results indicated that the scale items were relevant to the factor they belong to, and the scale was relevant to the measurement purpose. However, during the first round of evaluation, three items were unclear, and 12 items were rated as "useful, but not essential" by one to three experts, with CVR scores below 0.99 for these items, suggesting that they should be eliminated. In the second evaluation round, two items were considered unclear, and nine out of the 12 items mentioned above recommended to eliminate were considered "essential". Only three items were rated as "useful but essential" by one expert. However, in the second evaluation round, there was one "essential" item identified as "useful but not essential" by one expert and three items rated as "useful but not essential" by two experts. At the same time, seven patients who had seen a doctor in the CHC clinic in the previous month were willing to participate in the scale’s face validity evaluation. The evaluation results showed that two items' IIS < 1.5, suggesting that they were unimportant and should be eliminated. Based on these comments, we added some minor revisions to the expression of the item and then got the scale-v6. However, we did not eliminate any item assessed as "useful but not essential" or items with IIS < 1.5. After each round of evaluation, we refined the items' phrasing without modifying the components to which the items belonged. We improved the efficiency by conducting translation and content validity analysis simultaneously. Finally, before conducting field surveys, all items in the scale-v6 were assessed under appropriate components and items.
Construct validity assessment
Characteristics of study participants
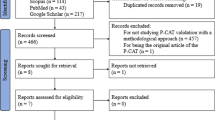
Our study used the scale-v6 to complete the field survey in stage 4. There were 296 (63.4%, 467 were invited in total) outpatients who completed one-to-one, face-to-face interviews using the 21-item adapted scale (scale-v6), 188 in Guangzhou city and 108 in Hohhot city. The information on the institution is presented in Additional file 1: Appendix 2). There was no statistical difference in mean age, gender, and the proportion of education level between the two cities' participants (Additional file 1: Appendix 4). Among the study participants, most outpatient individuals in Guangzhou visited clinicians for follow-up consultations, and nearly 70% of outpatients visited general practitioners to complete their consultations. The two main reasons for their clinical visits were getting a common cold and seeking care for prescribed medication for hypertension treatment.
Factor analysis
Our initial CFA model used data from 296 outpatients. However, the initial constrained 4-factor CFA model did not fit well [27]: \({\chi }^{2}=455.61\), P < 0.001, \({\chi }^{2}/df=2.435\), RMSEA = 0.072 (90%CI: 0.064 ~ 0.081), CFI = 0.906, TLI = 0.891. Though the CFI was greater than 0.90, the TFI was less than 0.90, suggesting that the model did not fit well. The correlations and loadings used to define factors were statistically significant (P < 0.01). Then, we used the same data for the EFA. Bartlett's spherical test result presented KMO = 0.931. Three factors were extracted according to the characteristic roots, greater than 1 in the scree plot, and the cumulative explained variance is 54.95% (Additional file 1: Appendix 5). All 21 items were allocated into three factors. Correlations among factors were 0.453 for F1 with F2, 0.558 for F1 with F3, and 0.510 for F2 with F3. Correlations and loadings used to define factors are statistically significant (P < 0.05). The factor loadings range from 0.337 to 0.874. The loading for the item is shown in Table 2. This 3-factor solution was conceptually reasonable based on this EFA model and had a good model fit with \({\chi }^{2}=192.756\), P = 0.011, \({\chi }^{2}/df=1.283\), RMSEA = 0.031 (90%CI:0.016 ~ 0.043), CFI = 0.993, TLI = 0.990. To confirm whether the final EFA model fits well, we use the CFA to validate it. The CFA model also had a good model fit with \({\chi }^{2}=294.573\), P < 0.001, \({\chi }^{2}/df=1.584\), RMSEA = 0.044 (90%CI: 0.035 ~ 0.054), CFI = 0.981, TLI = 0.979. Figure 2 presents the relatively high loadings, ranging from 0.553 to 0.888. Correlations among the factors ranged from 0.838 to 0.844 (Fig. 2). Table 3 presents the commonality of items belonging to the components in the original scale and our new 3-factor scale.

The final CFA result of a 3-factor structure for the 21-item Chinese version PPPC-R scale (standardized parameter estimates, P<0.001)
Response patterns and reliability
Table 4 presents the 21-item means and standard deviations and response patterns. All items present high endorsement rates in alternatives 1 and 2. No option has an endorsement proportion over 0.95. However, alternative 4 has the lowest endorsement proportion (lower than 0.05). The overall Cronbach's α value for the 21 items was 0.922, and the Cronbach's α value for each factor was 0.851, 0.872, and 0.717, respectively.
Discussion
Main findings
In this study, we translated a 21-item PPPC scale developed by Ryan et al. [9] into Chinese and validated it with a study sample of 296 outpatients of Guangzhou and Hohhot city to generate a tool for evaluating the patient-centered care quality in outpatients from primary healthcare settings in China. Although the 21 items did not completely align with the four components under the PCCM conceptual framework, the Chinese version of the PPPC scale demonstrated rigorous validity and reliability of three distinct factors and covered the four PCCM components. This pioneering study addressed a subjective assessment of patient-centered care measures in China [9] and bridged the evidence gap in applying patients’ perceptions of measuring the patient-centered care quality.
The scale-v6 was assessed under appropriate components through adaptation and content validation and could comprehensively reflect an underlying highly related, progressive, and interactive relationship of patient-centered service. That is when the physician is “exploring health, disease, and the illness experience”, if the physician “understands the whole person” (of the patient), they are likely to “find common ground” (with the patient) gradually and eventually “enhance the patient-clinician relationship”, [2, 9] to improve health outcomes of the patient [2, 5, 32]. Although our interviews were conducted inside the medical facilities, interviewees only met interviewers in person during the whole interview process, with no physicians or other medical staff on-site to ensure that interviewees’ responses were not affected.
Our final CFA results showed that the 21 items formed a 3-factor scale (Table 4). Specifically, the physician learned about the disease’s progression through communication with the patient (F1). During the interactive discussion about treatment plans (F2), they gradually learned about the patient’s personal and family situations with compassion, improving the patient's perception of care and respect from the physician and ultimately enhancing the patient-clinician relationship (F3).
Comparison with previous scales
Compared with the results from Ryan et al., [9] F1 in our results contained most items under the component of “health, disease, and the illness experience”, except item 11, which is item 8 in the 18-item PPPC-R scale. Other items stayed consistent with the results from Ryan et al. Our results also aligned with findings from testing the 18-item scale used by Nguyen et al. [4] in the primarily Francophone areas in Canada. From patients' perspective, components 1 and 2 (exploring health, disease, and the illness experience; understanding the whole person) may be closely related and necessary during appointments with physicians, and learning the causes and development of diseases is a mandatory procedure. The combination of most items in these two components may account for health care processes as a whole. This finding suggests that patients from different geographic settings may have similar experiences with a consultation procedure during medical visits.
Items in F2 and F3 in this study differed from Ryan’s study [9] but were similar to those in Nguyen et al. [4]. In this study, F2 contained the items from the PCCM’s four components. Interviewees may understand a progressive relationship among the seven items beneath F2 as follows: after physicians learn about disease development and causes, they start to discuss treatment plans with patients (items 11, 12, and 13); patients can perceive and evaluate the extent of attention paid and compassion shown by physicians during appointments (items 14, 15, 1, 19). Short appointments may restrict further communication, and physicians would formulate treatment plans based on preliminary basic inquiries [14]. As patient-centered approaches become more popular, more general practitioners in primary care settings have adopted the Reason-Ideas-Concerns-Expectations (RICE) approach for inquiry training [33]. This can be traced back to the exact origin of Ideas-Concerns-Expectations (ICE) [34, 35]. The ICE approach also included exploring disease causes during inquiries to improve patient communication and reinforce mutual trust in the patient-clinician relationship. With improved health literacy among the Chinese population, [36] many patients have gained basic health knowledge. They wish to discuss treatment or care plans with healthcare providers [37]. Physicians need to communicate with patients and understand patient concerns to learn about patient expectations regarding treatment outcomes. Meanwhile, patients can feel physicians' full attention and compassion, encouraging more patient-clinician communications. Therefore, the items under F2 can reflect the extent of patient-clinician interactions during medical visits.
The five items in F3 in this study belong to three components in the PCCM. Item 8 reflected the opportunity for the patient to ask questions. Item 16 reflected the comfort of discussing health problems with the physician. Item 17 evaluated the respect from the physician felt by the patient when the patient is expressing personal opinions. Items 20 and 21 assessed the physician’s listening and the patient’s trust in the physician. These five items together indicated the patient’s subjective feelings during the communication with the physician. When patients have more opportunities to ask questions, and as their perceived empowerment enhances, [38] they can express their attitudes and opinions more freely. Patients will acquire more trust in physicians if they receive attentive listening, leading to improved patient-clinician relationships.
F3 in the study by Ryan et al. reflected the patient’s role in the diagnosis and treatment process. However, neither this study nor Nguyen et al. [4] arrived at the same finding. One possible explanation is that outpatients may not be aware of the need to consult with physicians and participate in the treatment plan decision-making (Additional file 1: Appendix 4). In addition, due to restricted time for inquiries, [14] patients may not be able to express opinions adequately or have an in-depth discussion about treatment plans. As a result, they tend to follow decisions by physicians.
Recommendations for future scale development
When constructing response options for each item, it is critical to distinguish them from each other to reflect the interviewees’ genuine intentions accurately [27]. We analyzed the response patterns in this study and found that few interviewees chose the lowest ratings (D option, endorsement proportion < 0.05), which was close to the result in Ryan et al. [9]. As patient-centered care becomes more widely recognized in healthcare settings, physicians’ service quality is anticipated to improve, and extremely unsatisfying physician service will become rare [38]. Another possible explanation for the relatively high rating is that patients may have a low expectation of health services from primary care facilities. Although our interviews were conducted inside the medical facilities, interviewees only met interviewers in person during the whole interview process, without physicians or other medical staff, to ensure that interviewees’ responses were not affected. Overall, it is unlikely that the option settings were biased, and we concluded that they were appropriate for this scale.
Also, factors need to be distinguished from each other. If factors are not distinct enough to measure a singular characteristic, Cronbach’s α for assessing internal consistency would sharply decline when the number of items is reduced [27]. Our internal consistency analysis for all three factors suggested a modest decline compared with the overall internal consistency as a whole. However, Cronbach’s α scores for each of the three factors were greater than 0.7. The three factors in this scale can both synthetically and independently reflect the patient-centered care service quality from the perspectives of patients.
Limitations
Three limitations need to be considered for this study. First, previous studies have suggested that PPPC could be more beneficial for patients with experience with multiple medical diagnoses and treatments than for evaluating the patient experience of a single medical appointment [9]. Although we asked participants why they came to the health facility, whether it was their first visit or follow-up check, we did not collect information about their previous medical consultation experiences and encounters related to other illnesses in that health facility. This may affect the results of factor analysis. Second, the facilities selected for this study were chosen through convenience sampling. Although we intended to include diversity in the study sample, such as the regional economy (i.e., developed or undeveloped), facility location (i.e., urban or suburban), and scale (i.e., community health center or health service station), the sample representativeness remains questionable. Randomized sampling should be considered in future research to improve the generalizability of research findings. Third, we did not split our data into two to conduct the EFA and CFA separately because of the sample size limitation. In our future study, we would like to test the 3-factor model further in larger and more diverse samples. Fourth, the PPPC-CN calculated an overall mean score [9] which presented that the lower the score, the better the patient-centeredness care quality. However, this inverse scoring method may not be intuitive [39]. Future design may consider reassigning the scores to achieve a direct scoring scheme.
Conclusions
The PPPC-CN scale, developed based on the PCCM framework, provides a valuable instrument tool for evaluating patient-centered medical service quality from patients' perspectives. The PCCM framework has represented a progressive relationship among four interacting components to improve the patient-clinician relationship during medical consultations. Future research needs to examine new items that should be designed to achieve a more robust and separately mapping of the questionnaire to the four components of the PCCM framework or use separate scales to assess each component.
Availability of data and materials
This study does not share the original data. If there are any special needs, researchers could send an application to caiyiyuan@gmc.edu.cn.
References
Institute of Medicine. Crossing the quality chasm: A new health care system for the 21st century. Washington: National Academy Press; 2001.
Hudon C, Fortin M, Haggerty JL, Lambert M, Poitras ME. Measuring patients’ perceptions of patient-centered care: a systematic review of tools for family medicine. Ann Fam Med. 2011;9(2):155–64.
McMillan SS, Kendall E, Sav A, et al. Patient-centered approaches to health care: a systematic review of randomized controlled trials. Med Care Res Rev. 2013;70(6):567–96.
Nguyen TN, Ngangue PA, Ryan BL, et al. The revised Patient Perception of Patient-Centeredness Questionnaire: Exploring the factor structure in French-speaking patients with multimorbidity. Health Expect. 2020;23(4):904–9.
Stewart M, Brown JB, Donner A, et al. The impact of patientcentered care on outcomes. J Fam Pract. 2000;49(9):796–804.
Stewart M, Ryan BL, Bodea C. Is patient-centred care associated with lower diagnostic costs. Healthc Policy. 2011;6(4):27–31.
Hanefeld J, Powell-Jackson T, Balabanova D. Understanding and measuring quality of care: dealing with complexity. Bull World Health Organ. 2017;95(5):368–74.
Mohammed K, Nolan MB, Rajjo T, et al. Creating a patient-centered health care delivery system: a systematic review of health care quality from the patient perspective. Am J Med Qual. 2016;31(1):12–21.
Ryan BL, Brown JB, Tremblay PF, Stewart M. Measuring patients’ perceptions of health care encounters: examining the factor structure of the revised Patient Perception of Patient-Centeredness (PPPC-R) questionnaire. J Patient Cent Res Rev. 2019;6(3):192–202.
Patient Centered Care. Focus on low and middle income countries and proposition of new conceptual model. J Med Surg Res. 2020;7(1):755–63.
Stewart M, Weston W MIR, McWillliam CL FT. Patient-Centered Medicine: Transforming the Clinical Method 3rd edition. London: Radcliffe Publishing Ltd; 2014.
Winn K, Ozanne E, Sepucha K. Measuring patient-centered care: An updated systematic review of how studies define and report concordance between patients’ preferences and medical treatments. Patient Educ Couns. 2015;98(7):811–21.
Little P, Everitt H, Williamson I, et al. Preferences of patients for patient centred approach to consultation in primary care: observational study. BMJ. 2001;322(7284):468–72.
Irving G, Neves AL, Dambha-Miller H, et al. International variations in primary care physician consultation time: a systematic review of 67 countries. BMJ Open. 2017;7(10):e017902.
Clayton MF, Dudley WN, Musters A. Communication with breast cancer survivors. Health Commun. 2008;23(3):207–21.
Gorman JR, Drizin JH, Smith E, Flores-Sanchez Y, Harvey SM. Patient-Centered Communication to Address Young Adult Breast Cancer Survivors’ Reproductive and Sexual Health Concerns. Health Commun. 2021;36(13):1743–58.
Ishikawa H, Hashimoto H, Roter DL, Yamazaki Y, Takayama T, Yano E. Patient contribution to the medical dialogue and perceived patient-centeredness. An observational study in Japanese geriatric consultations. J Gen Intern Med. 2005;20(10):906–10.
Meredith L, Stewart M, Brown JB. Patient-centered communication scoring method report on nine coded interviews. Health Commun. 2001;13(1):19–31.
Reinders ME, Blankenstein AH, Knol DL, de Vet HC, van Marwijk HW. Validity aspects of the patient feedback questionnaire on consultation skills (PFC), a promising learning instrument in medical education. Patient Educ Couns. 2009;76(2):202–6.
Stewart M, Brown JB, Hammerton J, et al. Improving communication between doctors and breast cancer patients. Ann Fam Med. 2007;5(5):387–94.
Mohle Peter, Dorer Brita, de Jong Julie, Hu Mengyao (2016). Adaptation. Guidelines for Best Practice in Cross-Cultural Surveys. Ann Arbor, MI: Survey Research Center, Institute for Social Research, University of Michigan. Retrieved March, 25, 2022, from http://ccsg.isr.umich.edu/. Guidelines for Best Practice in Cross-Cultural Surveys.
Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine (Phila Pa 1976). 2000;25(24):3186–91.
Mokkink LB, Terwee CB, Patrick DL, et al. The COSMIN study reached international consensus on taxonomy, terminology, and definitions of measurement properties for health-related patient-reported outcomes. J Clin Epidemiol. 2010;63(7):737–45.
Boateng GO, Neilands TB, Frongillo EA, Melgar-Quiñonez HR, Young SL. Best practices for developing and validating scales for health, social, and behavioral research: a primer. Front Public Health. 2018;6:149.
Harvey LA. REDCap: web-based software for all types of data storage and collection. Spinal Cord. 2018;56(7):625.
Zamanzadeh V, Ghahramanian A, Rassouli M, Abbaszadeh A, Alavi-Majd H, Nikanfar AR. Design and implementation content validity study: development of an instrument for measuring patient-centered communication. J Caring Sci. 2015;4(2):165–78.
DL Streiner GRN, Cairney J J. Health measurement scales: a practical guide to their development and use. 2015.
Peterson RA. A meta-analysis of variance accounted for and factor loadings in exploratory factor analysis. Mark Lett. 2000;11(3):261–75.
Wu Q, Ye X, Wu Y, Zhao L. Development and Psychometric Evaluation of the Patient Engagement in Health Care Questionnaire. J Nurs Care Qual. 2020;35(3):35–40.
Kimberlin CL, Winterstein AG. Validity and reliability of measurement instruments used in research. Am J Health Syst Pharm. 2008;65(23):2276–84.
Zhang J, Zhao L, Zhao D, et al. Reliability and validity of the Chinese version of the Test for Respiratory and Asthma Control in Kids (TRACK) in preschool children with asthma: a prospective validation study. BMJ Open. 2019;9(8):e025378.
Rathert C, Wyrwich MD, Boren SA. Patient-centered care and outcomes: a systematic review of the literature. Med Care Res Rev. 2013;70(4):351–79.
Jing W, Ren J. Diagnosis and treatment thinking of case introduction in general practic (In Chinese). Beijing: People’s Medical Publishing House Co; 2001.
Matthys J, Elwyn G, Van Nuland M, et al. Patients’ ideas, concerns, and expectations (ICE) in general practice: impact on prescribing. Br J Gen Pract. 2009;59(558):29–36.
Schrans D, Boeckxstaens P, De Sutter A, et al. Is it possible to register the ideas, concerns and expectations behind the reason for encounter as a means of classifying patient preferences with ICPC-2. Prim Health Care Res Dev. 2018;19(1):1–6.
Nie X, Li Y, Li C, Wu J, Li L. The association between health literacy and self-rated health among residents of China aged 15–69 years. Am J Prev Med. 2021;60(4):569–78.
Jiang S, Street RL Jr. The effects of patient-centered communication, social capital, and internet use on patient empowerment: a cross-sectional study in China. Glob Health Promot. 2019;26(4):33–43.
Jiang S. Pathways linking patient-centered communication to health improvement: a longitudinal study in China. J Health Commun. 2019;24(2):156–64.
Ree E, Wiig S, Manser T, Storm M. How is patient involvement measured in patient centeredness scales for health professionals? A systematic review of their measurement properties and content. BMC Health Serv Res. 2019;19(1):12.
Acknowledgements
We sincerely thank all the Delphi panelists: Bing Deng, Jing Gu, Chun Hao, Li Kuang, Shaolong Wu, Xueji Wu, and Mi Yao. We thank all the investigators for their dedication and hard work. We thank all the community coordinators; without your support, we can not complete this study smoothly.
Funding
The China National Natural Science Foundation (grant 72164005), the National Key R&D Program of China (2021ZD0113405), the China National Natural Science Foundation (grant 71974211), the Swiss Agency for Development and Cooperation (grant 81067392), and the China Medical Board (grants 16–260, 18–301, 18–300, 19–310, and 20–368).
Author information
Authors and Affiliations
Contributions
Y.Y. Cai, P.F. Guo, and J. Tu contributed equally to this article. Y. Y. Cai, J. Tu and D(R). Xu conceptualized the study. Y.Y Cai, S.X. Zhao, X.F. Li, X.H. Wang and N. Zhang coordinated the implementation of this study in Guangzhou and Hohhot City. P.F. Guo, Y. R. Li, and Y.Y. Cai conducted the data analysis. M.Y. Hu and E. R. Melipillán provided the sampling methods and checked the analysis methods. L.R Liu, B. L. Ryan, J. Liao, R. Dev, T.Y. Huang, R.L. Huang, L. Kuang, R.N. Huang, and W.J. He coordinated with Y.Y. Cai to refine the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study obtained the institution review board approval from Sun Yat-Sen University [No.2019(005)]. All patient participants have provided informed consent before data collection. All methods presented in the Methods section of the study were following relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Appendix 1. Detailed procedures of this study. Appendix 2. Healthcare settings. Appendix 3. Scale translation and localization for items that are difficult to understand for interviewees. Appendix 4. Characteristics of study participants. Appendix 5. Factor analysis to determinant the number of factors.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Cai, Y., Guo, P., Tu, J. et al. Contextualizing the revised Patient Perception of Patient-Centeredness (PPPC-R) scale in primary healthcare settings: a validity and reliability evaluation study. BMC Prim. Care 25, 11 (2024). https://doi.org/10.1186/s12875-023-02227-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12875-023-02227-x