
Abstract
Background
A major challenge in updating clinical guidelines is to efficiently identify new, relevant evidence. We evaluated the efficiency and feasibility of two new approaches: the development of restrictive search strategies using PubMed Clinical Queries for MEDLINE and the use of the PLUS (McMaster Premium Literature Service) database.
Methods
We evaluated a random sample of recommendations from a national guideline development program and identified the references that would potentially trigger an update (key references) using an exhaustive approach.
We designed restrictive search strategies using the minimum number of Medical Subject Headings (MeSH) terms and text words required from the original exhaustive search strategies and applying broad and narrow filters. We developed PLUS search strategies, matching Medical Subject Headings (MeSH) and Systematized Nomenclature of Medicine (SNOMED) terms with guideline topics. We compared the number of key references retrieved by these approaches with those retrieved by the exhaustive approach.
Results
The restrictive approach retrieved 68.1 % fewer references than the exhaustive approach (12,486 versus 39,136), and identified 89.9 % (62/69) of key references and 88 % (22/25) of recommendation updates. The use of PLUS retrieved 88.5 % fewer references than the exhaustive approach (4,486 versus 39,136) and identified substantially fewer key references (18/69, 26.1 %) and fewer recommendation updates (10/25, 40 %).
Conclusions
The proposed restrictive approach is a highly efficient and feasible method to identify new evidence that triggers a recommendation update. Searching only in the PLUS database proved to be a suboptimal approach and suggests the need for topic-specific tailoring.
Similar content being viewed by others

Background
Clinical guidelines, like systematic reviews and other evidence summaries, require periodic reassessment of research evidence to remain valid [1–4]. Current guidance usually recommends revision and update within two to three years of their publication [5, 6]. New evidence to update clinical guidelines is generally identified using the original exhaustive search strategies [7].
A major challenge for guideline developers is to efficiently screen for new, relevant evidence that justifies a clinical guideline update. Unfortunately, little empirical work has been conducted to date to test the effectiveness and efficiency of searching processes [7]. More than a decade ago, Shekelle et al. developed a strategy based on retrieving reviews, editorials, and commentaries in high impact general journals and specialised journals, complemented with a survey by clinical experts [8]. Gartlehner et al. compared a modified version of this strategy versus an exhaustive search strategy [9]. The results so far have shown that restrictive approaches are promising, but more information is needed about the timing and type of search [7].
Similarly, researchers are testing alternative search strategies to update systematic reviews [10–13]. Haynes et al. developed the McMaster Premium Literature Service (PLUS) database, from the McMaster Health Knowledge Refinery [14, 15]. PLUS contains a searchable subset of pre-appraised primary studies and systematic reviews from more than 120 journals and it can identify key articles needed to update systematic reviews [14, 15]. Clinical Queries search filters in MEDLINE and EMBASE have also shown a high sensitivity to detect key articles [11].
We designed a study to evaluate the efficiency and feasibility of two approaches to identify the need to update clinical guidelines recommendations: 1) restrictive search strategies using PubMed Clinical Queries search filters for MEDLINE and 2) the use of PLUS database.
Methods
Design
We conducted a descriptive study of search strategies to identify the references that update recommendations from clinical guidelines. We developed three search strategies to identify the need to update the recommendations: an exhaustive approach, a restrictive approach, and a PLUS approach.
The sample was obtained from a previous study and included a stratified random sample of recommendations from the Spanish National Health System Clinical Guidelines Program [1, 16]. The selection process involved two phases: 1) we stratified guidelines by topic and by year of publication; when multiple guidelines per strata were available, we randomly selected one; 2) we performed a stratified random sampling of recommendations by guideline topic and by turnover (number of pertinent references linked per recommendation in the updating process).
1) Exhaustive approach
Guideline methodologists with experience designing search strategies developed exhaustive literature search strategies for each clinical question: 1) based on the original searches; and 2) applying the filters of the original study. An example of the exhaustive search strategy is available in Additional file 1. We also contacted clinical experts to identify new studies. We obtained a reference database of clinical questions. We screened the references and assessed them qualitatively as: 1) Pertinent references: Randomised controlled trials or systematic reviews related to the topic of the clinical guideline; 2) Relevant references: pertinent references that could be used when considering an update to a recommendation, but that would not necessarily trigger a potential update; and 3) Key references: relevant references that would potentially trigger an update because of their impact on the population, the intervention, the comparison, the outcome, the quality of the evidence, the direction and/or the strength of the recommendation. Using the results of the reference screening we classified recommendations as: 1) need for updating: with one or more key references linked; or 2) still valid: without key references linked.
A more complete description of this approach is available in the previously published protocol and survival analysis results [1, 16].
2) Restrictive approach
Guideline methodologists, trained by researchers with experience designing search strategies, developed restrictive search strategies for each clinical question using the PubMed Clinical Queries search filters for the MEDLINE database. We considered clinical questions that had at least two PICO (population, intervention, comparator or outcome) components. We developed the restrictive search strategies considering the minimum number of Medical Subject Headings (MeSH) terms and text words required from the original exhaustive searches strategies. The search strategies were designed in four stages [Fig. 1]: 1) Development: we selected keywords from the clinical questions and identified Medical Subject Headings (MeSH) terms and text words in titles; 2) Validation: we evaluated whether each search retrieved all the original references for its corresponding recommendation; 3) Refinement: If a search did not retrieve all the original references, we selected and searched less specific Medical Subject Headings (MeSH) and/or text words in the title or abstract; and 4) Application of each of a broad and a narrow treatment Clinical Queries filter (www.ncbi.nlm.nih.gov/pubmed/clinical), and a systematic review filter [17]. We used the same date limits as with the exhaustive approach (from the complete year in which the original exhaustive searches was completed onwards). An example of a restrictive search strategy is available in Additional file 1.

Restrictive approach algorithm. Figure01_RestrictiveApproachAlgorithm. Microsoft PowerPoint presentation
3) PLUS approach
An information specialist from the Health Information Research Unit developed a PLUS search strategy for each guideline topic. We matched Medical Subject Headings (MeSH) and Systematized Nomenclature of Medicine (SNOMED) indexing terms in the PLUS database with clinical guideline topics. Both primary and review papers were included. To take into account the time delay associated with the critical appraisal process (CAP) the articles go through, we ran the PLUS searches strategies from the beginning of the year in which the original exhaustive searches were run, until approximately three months beyond the latest date of the exhaustive searches. An example of a PLUS search strategy is available in Additional file 1.
Outcome
Our primary outcome was the number of key references identified by each alternative approach.
Statistical methods
We performed a descriptive analysis of the data. We calculated absolute and relative frequencies or median and range, as appropriate.
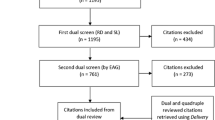
Two investigators independently retrieved the key references (identified in the exhaustive approach) in each of the alternative approach results. We analysed the number of key references in: 1) the results of restrictive search strategies per clinical question; 2) restrictive search strategies results per clinical guideline (clustering all references identified by clinical question) [Fig. 2]; and 3) results of PLUS strategies per clinical guideline. We did not identify additional pertinent, relevant or key references from the alternative approaches. We did not develop restrictive search strategies for clinical questions with less than two of the four PICO components, prognosis or diagnostic clinical questions. In these instances we used the updated exhaustive search strategies.

References analysis. Figure02_ReferencesAnalysis. Microsoft PowerPoint presentation
We identified the recommendations that needed an update (with one or more key references) retrieved by each alternative approach. We compared the recommendations identified with those that were not identified according to clinical guideline topic (cancer, cardiovascular disease, mental health or metabolic disease), strength of recommendation (A, B, C, D or good practice point [18]), clinical purpose (prevention, screening, diagnosis, treatment or other), and turnover. Each recommendation was classified according to the number of linked pertinent references: none, ≤ median number (low turnover), or > median number (high turnover). We used Pearson’s chi-square test or Fisher’s exact test, as appropriate.
We recorded the number of hours spent on designing each approach and the number of researchers involved.
We accepted p values of less than 0.05 as significant in all calculations. We performed the analyses using SPSS 21.0 (SPSS Inc., Chicago, Illinois).
Results
We included a cohort of four clinical guidelines from the Spanish National Health System Clinical Guidelines Programme, corresponding to 87 clinical questions and 249 recommendations [19–22]. After the random selection process, the final recommendation sample included 43 clinical questions and 113 recommendations.
Exhaustive approach results
This approach retrieved a total of 39,136 references from the four clinical guidelines included. From the recommendations sample, we identified a total of 69 key references and 25 recommendations that potentially needed an update [Table 1].
Restrictive approach results
We applied the restrictive approach to 88.5 % (77/87) clinical questions from the included clinical guidelines, corresponding to 85 % (96/113) of the recommendations from our recommendation sample. We excluded eight questions that did not present a minimum of two PICO components (population, intervention, comparator or outcome) and one diagnostic question.
The restrictive searches covered a mean of 4.6 years (range 3.9 – 5.1 years) from 2008–2009 to 2011 – 2012 [Table 2].
For the clinical guidelines included, we retrieved a total of 40,021 references using the broad filter and 9,958 references using the narrow filter [Table 2]. We retrieved more key references when we clustered results of references per guideline rather than per question (40 [87 %] and 39 [84.8 %] compared with 26 [56.5 %] and 25 [54.3 %] using the broad and narrow filters, respectively) [Table 2, Additional file 2]. Similarly, clustered results of references per guideline identified a higher number of recommendations that were considered to potentially need an update (18 [90.0 %] and 17 [85 %] compared with 15 [75 %] and 14 [70 %] respectively [Table 2].
When we used exhaustive search strategies for the clinical questions not developed by the restrictive approach (narrow filter and clustering by all questions), we retrieved a total of 12,486 references, and we identified a total of 62 (89.9 %) key references and 22 (88.0 %) recommendations that potentially needed an update [Table 4].
The restrictive approach (narrow filter and clustering by all questions) failed to identify seven key references (15.2 %): four (57.1 %) references were systematic reviews and three references (42.9 %) were congress abstracts (not indexed in MEDLINE) [Fig. 3].

Key references not identified by restrictive approach. Figure03_RefNotIdentifiedRestrictive. Microsoft PowerPoint presentation
The recommendations that potentially needed an update not identified by the restrictive approach were similar to those that were identified in terms of topic, strength of the recommendations, clinical purpose, and turnover [Additional file 3].
PLUS approach results
The PLUS searches covered a median of 5.0 years (range 4.1 – 5.3 years) from 2008–2009 to 2011 – 2012 [Table 3].
For the clinical guidelines included, we retrieved a total of 4,486 references (range 137 – 3,059) [Table 3]. For the recommendation sample, we retrieved 18 (26.1 %) key references; these references potentially update 10 (40 %) recommendations [Table 3, Additional file 2].
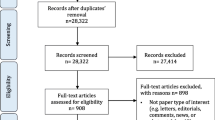
The PLUS approach failed to identify 51 key references (73.9 %); most (41 references, 80.4 %) were from journals not included in PLUS database [Fig. 4].

Key references not identified by PLUS approach. Figure04_RefNotIdentifiedPLUS. Microsoft PowerPoint presentation
Recommendations with a high turnover were more likely to be identified by the PLUS approach. The remaining factors (clinical guideline topic, strength of the recommendations, and clinical purpose) were not significantly associated with the need to update [Additional file 3].
Resource use
Three guideline methodologists spent a total of 174 h in designing and running the restrictive search strategies [Table 4]. The PLUS search strategies were developed by an information specialist who designed and ran the searches in 28 h [Table 4].
Discussion
We evaluated two search strategies to identify signals for updating recommendations and compared them to an exhaustive search strategy using a random sample of recommendations from a cohort of clinical guidelines from a national guideline development program.
The restrictive approach (using a narrow PubMed Clinical Queries filter, clustering results per clinical guideline and imputing exhaustive search results for clinical questions not developed) retrieved 68.1 % fewer references than the exhaustive approach, and identified most of the key references (62/69, 89.9 %) and recommendations updates (22/25, 88.0 %). We developed search strategies for each clinical question but obtained better results by considering the results across all questions included in a clinical guideline. The restrictive approach proved to be relatively simple to develop, not needing the expertise of information retrieval specialists. Over half of the very few missing key references with this approach were systematic reviews. Three references were missed due to a mistake in the design of restrictive searches, and one was missed by the filter used [17], reflecting the need to pay more attention to the design and quality check of search strategies. Additional searches for systematic reviews in specific databases, like Epistemonikos, could prove useful [www.epistemonikos.org/]).
Our results show that PLUS approach retrieved 88.5 % fewer references than the exhaustive approach but identified a substantially lower number of key references (18/69, 26.1 %) and potential updates (10/25, 40 %) than the restrictive approach. These results were similar independently of the searches being performed by a PLUS information specialist (using search strategies) or directly using the PLUS interface using topic synonyms (post-hoc analysis). This poor performance was mainly due to most of these key references (80.4 %) being from journals not included in PLUS database.
The PLUS approach performed differently across topics with major depression performing best (66.7 % of key references retrieved) and prostate cancer worst (14.3 %). This poor performance in the prostate cancer guideline is explained by the fact that the PLUS database does not include a large number of urology journals. This resource includes a limited number of journals with a stronger focus on a limited number of specialties and health topics. Given these findings and building on previous research in the systematic reviews and clinical guidelines fields, post-hoc we explored a potential approach of tailoring the PLUS approach by adding a limited number of journals for each specialty (e.g. those with a higher impact factor) [8, 9, 12, 13]. However, missing key references were published in a highly heterogeneous sample of journals, with only 3.4 % being in the first decile [Fig. 4].
The two search strategies we tested were far less time consuming than the exhaustive search strategy. The restrictive approach needs initial tailoring and takes each original guideline, question, search and references into account. In contrast, the PLUS approach could be potentially executed directly in its interface simply using topic synonyms from clinical guidelines.
Our results in the context of previous research
Only one previous study of clinical guidelines compared a different type of restrictive approach versus an exhaustive approach [9]. However, this study considered prevention topics as the unit of analysis rather than the individual recommendations. Furthermore, the authors restricted the search to MEDLINE, using publication types (review articles, editorials, guidelines and commentaries) and limiting the search to core and specialty clinical journals [9].
A recent evaluation of NICE clinical guidelines for interventional procedures also showed that updated recommendations that required a modification generally had a greater increase in their evidence base (number of patients included in observational studies published) than non-updated recommendations [23]. Our results are consistent with this finding, showing a higher efficiency of the PLUS approach in recommendations with a higher turnover.
There is indirect evidence about the performance of PLUS for clinical guidelines from a previous study that evaluated the updating of systematic reviews [11]. Only 13 out of 87 systematic reviews (14.9 %) included all the new studies in PLUS. In 39 (44.8 %) reviews there was no statistically significant difference between PLUS and non-PLUS new studies (ROR: 0.99; 95 % confidence interval: 0.87-1.14). Thirty-five updated reviews (40.2 %) had no new studies indexed in PLUS (although conclusions were seldom altered by addition of new studies) [11]. Despite these results in systematic reviews, the PLUS database did not perform similarly in the context of clinical guidelines. However, we did not routinely determine the change in effect sizes with key references, so we could not assess their quantitative relationship. Neither did we assess whether references identified in the PLUS database could have reliably signalled the need to update for topics that were in the journals that are included.
The same study by Hemens et al. confirmed the high sensitivity of Clinical Queries filters for MEDLINE and EMBASE in detecting randomized controlled trials [11]. This is consistent with our results showing that incorporating Clinical Queries filters (to identify randomized controlled trials) and Montori’s et al. filter (to identify systematic reviews) significantly reduces the citation screening burden [17].
Strengths and limitations
We used a rigorous and explicit methodology building on previous research in this area, improving its deficiencies, and implementing an innovative solution. We also used the exhaustive approach as a standard, improving the validity of the results and, hence, the strength of our inferences. We independently screened and extracted the data in pairs and included methodologists and panel members from the original guidelines as far as possible. Finally, we laid out a structured framework (e.g., outcome definitions) that could prove useful in the future for other researchers in the field.
Our study has some limitations. We did not assess all references retrieved by each alternative approach, so we were not able to evaluate whether other key references were identified by any of these approaches. Our sample is limited to recommendations from four guidelines topics. However, this potential limitation is mitigated because our sample covers broad areas such as cancer, cardiovascular diseases, mental health and lifestyle and behavioural issues. Additionally, we based our exhaustive search strategies on searches specifically designed during the original guidelines development. A post-hoc analysis revealed several mistakes and inconsistencies in search strategies that could have been avoided through peer review process [24]. However, the validation of the accuracy of the original search strategies was beyond the scope of our study. We are unable to estimate how this issue could affect the recall of the exhaustive search strategies, although we think that these deficiencies are minor and that they do not alter our conclusions. We included only randomised controlled trials and systematic reviews and did not incorporate observational studies, diagnostic questions or evidence about values and preferences or resource use considerations. Finally, some authors had conflicts of interest due to their involvement in the PLUS database and Clinical Queries filter development. However, they did not participate in the identification of key references.
Conclusions
Our results have important implications both for the updating of guidelines and for future research in this field. The proposed method of developing restrictive search strategies, using PubMed Clinical Queries filters in the MEDLINE database, provides a feasible and efficient method for guideline developers to identify significant new studies that are likely to trigger a recommendation update. Searching only in the PLUS database was a suboptimal approach that needs topic specific tailoring.
Our results highlight the need for additional methodological research in this field. For this future work, investigators are likely to find our framework helpful.
References
Martínez García L, Sanabria AJ, García Alvarez E, Trujillo-Martín MM, Etxeandia-Ikobaltzeta I, Kotzeva A, et al. The validity of recommendations from clinical guidelines: a survival analysis. CMAJ. 2014;186(16):1211–9.
Alderson LJ, Alderson P, Tan T. Median life span of a cohort of national institute for health and care excellence clinical guidelines was about 60 months. J Clin Epidemiol. 2014;67(1):52–5.
Shojania KG, Sampson M, Ansari MT, Ji J, Doucette S, Moher D. How quickly do systematic reviews go out of date? A survival analysis. Ann Intern Med. 2007;147(4):224–33.
Banzi R, Cinquini M, Liberati A, Moschetti I, Pecoraro V, Tagliabue L, et al. Speed of updating online evidence based point of care summaries: prospective cohort analysis. BMJ. 2011;343:d5856.
Vernooij RW, Sanabria AJ, Solà I, Alonso-Coello P, Martínez García L. Guidance for updating clinical practice guidelines: a systematic review of methodological handbooks. Implement Sci. 2014;9:3.
Becker M, Neugebauer EA, Eikermann M. Partial updating of clinical practice guidelines often makes more sense than full updating: a systematic review on methods and the development of an updating procedure. J Clin Epidemiol. 2014;67(1):33–45.
Martínez García L, Arévalo-Rodríguez I, Solà I, Haynes RB, Vandvik PO, Alonso-Coello P, et al. Strategies for monitoring and updating clinical practice guidelines: a systematic review. Implement Sci. 2012;7:109.
Shekelle PG, Ortiz E, Rhodes S, Morton SC, Eccles MP, Grimshaw JM, et al. Validity of the agency for healthcare research and quality clinical practice guidelines: how quickly do guidelines become outdated? JAMA. 2001;286(12):1461–7.
Gartlehner G, West SL, Lohr KN, Kahwati L, Johnson JG, Harris RP, et al. Assessing the need to update prevention guidelines: a comparison of two methods. Int J Qual Health Care. 2004;16(5):399–406.
Gartlehner G, West SL, Lohr KN, Kahwati L, Johnson JG, Harris RP, et al. Surveillance search techniques identified the need to update systematic reviews. J Clin Epidemiol. 2008;61(8):755–62.
Hemens BJ, Haynes RB. McMaster Premium Literature Service (PLUS) performed well for identifying new studies for updated cochrane reviews. J Clin Epidemiol. 2012;65(1):62–72. e1.
Sagliocca L, De Masi S, Ferrigno L, Mele A, Traversa G. A pragmatic strategy for the review of clinical evidence. J Eval Clin Pract. 2013;19(4):689–96.
Shekelle PG, Motala A, Johnsen B, Newberry SJ. Assessment of a method to detect signals for updating systematic reviews. Syst Rev. 2014;3:13.
Haynes RB, Cotoi C, Holland J, Walters L, Wilczynski N, Jedraszewski D, et al. Second-order peer review of the medical literature for clinical practitioners. JAMA. 2006;295(15):1801–8.
Holland J, Haynes RB, McMaster PLUS, Team Health Information Research Unit. McMaster Premium Literature Service (PLUS): an evidence-based medicine information service delivered on the Web. AMIA Annu Symp Proc. 2005;340:4.
Martínez García L, Sanabria AJ, Araya I, Lawson J, Haynes RB, Rigau D, et al. Strategies to assess the validity of recommendations: a study protocol. Implement Sci. 2013;8(1):94.
Montori VM, Wilczynski NL, Morgan D, Haynes RB, Hedges Team. Optimal search strategies for retrieving systematic reviews from Medline: analytical survey. BMJ. 2005;330(7482):68.
Guidelines by topic. Edinburgh (Scotland): Scottish Intercollegiate Guidelines Network — Healthcare Improvement Scotland; 2013. Available: www.sign.ac.uk/guidelines/published/index.html (accessed 2014 Oct 1).
Working Group on the Management of Major Depression in Adults. Clinical practice guideline on the management of major depression in adults, National plan for the SHN of the MHCA. Axencia de avaliación de tecnoloxías sanitarias de Galicia (avalia-t). Madrid: Clinical Practice Guidelines in the Spanish SHN: avalia-t No 2006/06; 2008.
Working Group of the Guideline for the Prevention and Treatment of Childhood and Juvenile Obesity. Iberoamerican Cochrane Centre, coordinator; Clinical Practice Guideline for the Prevention and Treatment of Childhood and Juvenile Obesity; CPGs: Quality Plan for the Spanish National Healthcare System of the Spanish Ministry for Health and Social Policy; Catalan Agency for Health Technology Assessment; 2009. Clinical Practice Guideline: CAHTA no. 2007/25
Working group of the Clinical Practice Guideline on Prostate Cancer Treatment. Clinical practice guidelines on prostate cancer treatment, National plan for the NHS of the MSC. Aragon institute of health sciences (I + CS). Madrid: Clinical Practice Guidelines in the NHS I + CS No 2006/02; 2008.
Development group of the stroke prevention Guideline. Quality plan for the national health system of the ministry of health and consumer affairs; Catalan agency for health technology assessment and research. Madrid: Clinical Practice Guideline: AATRM Number 2006/15; 2008.
Lyratzopoulos G, Barnes S, Stegenga H, Peden S, Campbell B. Updating clinical practice recommendations: is it worthwhile and when? Int J Technol Assess Health Care. 2012;28(1):29–35.
Sampson M, McGowan J, Cogo E, Grimshaw J, Moher D, Lefebvre C. An evidence-based practice guideline for the peer review of electronic search strategies. J Clin Epidemiol. 2009;62(9):944–52.
Acknowledgements
The authors thank Mercedes Cabañas (Técnicas Avanzadas de Investigación en Servicios de Salud [TAISS], Madrid, Spain) and Joanna Kelly (Healthcare Improvement Scotland, Glasgow, UK) for their support in developing and running the exhaustive literature searches, and Carolyn Newey for her help editing the manuscript.
Laura Martínez García is a doctoral candidate at the Pediatrics, Obstetrics and Gynecology, and Preventive Medicine Department, Universitat Aunònoma de Barcelona, Barcelona, Spain.
Data sharing
The dataset is available from the corresponding author at laura.martinez.garcia@cochrane.es.
Funding
This project is funded by research grants from the Instituto de Salud Carlos III (FIS PI10/00346 to Pablo Alonso-Coello) and from the Canadian Institutes of Health Research (R. Brian Haynes). Laura Martínez García and Andrea Juliana Sanabria are funded by Río Hortega research contracts from the Instituto de Salud Carlos III (CM11/00035 and CM12/00168 respectively). Pablo Alonso-Coello is funded by a Miguel Servet research contract from the Instituto de Salud Carlos III (CP09/00137).
Members of the updating guidelines working group
Martínez García L; Sanabria AJ; Araya I; Lawson J; Solà I; Vernooij RWM; López D; García Álvarez E; Trujillo-Martín MM; Etxeandia-Ikobaltzeta I; Kotzeva A; Rigau D; Louro-González A; Barajas L; Díaz del Campo P; Estrada MD; Gracia J; Salcedo-Fernandez F; Haynes RB; Alonso-Coello P; Álvarez Ariza M; Argente Oliver J; Armario García P; Arrieta Antón E; Balaguer Santamaría A; Borque Fernando A; Buñuel Álvarez JC; Cervera Álvarez A; De Las Heras Liñero ME; Dopico L; Eddy Ives LS; Escó Barón R; Ferreira González I; Ferrer F; Gil Sanz MJ; Lago Deibe FI; Martí Canales JC; Martínez Rubio A; Martos Moreno GA; Mejuto Marti T; Morales Ortiz A; Rioja Sanz LA; Rioja Zuazu J; Rodríguez González A; Rodríguez-Arias Palomo JL; Sáenz Cusí A.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Competing interests
Laura Martínez García, Andrea Juliana Sanabria, David Rigau, Leticia Barajas-Nava, Ivan Solà and Pablo Alonso-Coello have received research grants from Instituto de Salud Carlos III (FIS PI10/00346). R. Brian Haynes and Jennifer Lawson have received research grants from the Canadian Institutes of Health Research. R. Brian Haynes and Jennifer Lawson have been involved in developing the McMaster PLUS Project and RBH originated the development of Clinical Queries, so did not participate in identifying key references or potential update recommendations. No other competing interests were declared.
Authors’ contributions
LMG, AJS, IA, PAC, DR and IS conceived the idea of the study. IA, JL, IS, RWMV and DL designed and/or ran searches strategies. EGA, MMTM, IEI, AK, DR, ALG, LBN, PDC and MDE screened the references. LMG and AJS performed the statistical analysis. LMG and PAC drafted the manuscript. All of the authors revised the manuscript critically for important intellectual content and approved the final version submitted for publication.
Additional files
Additional file 1:
Search strategies examples. We reported an example of exhaustive strategy, restrictive strategy, PLUS strategy. (PDF 82 kb)
Additional file 2:
Key references by approach. We reported key references by strategy, according to their clinical guidelines and linked to recommendation. (PDF 62 kb)
Additional file 3:
Additional tables. We reported complementary results (PDF 40 kb)
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Martínez García, L., Sanabria, A., Araya, I. et al. Efficiency of pragmatic search strategies to update clinical guidelines recommendations. BMC Med Res Methodol 15, 57 (2015). https://doi.org/10.1186/s12874-015-0058-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12874-015-0058-2