
Abstract
Background
Renal dysfunction is one of the adverse effects observed in methamphetamine (MET) or tramadol abusers. In this study, we aimed to review articles involving intoxication with MET or tramadol to assess the occurrence of renal dysfunction.
Methods
Two researchers systematically searched PubMed, Scopus, Web of Sciences, and Google Scholar databases from 2000 to 2022. All articles that assessed renal function indexes including creatine, Blood Urea Nitrogen (BUN), and Creatine phosphokinase (CPK) in MET and tramadol intoxication at the time of admission in hospitals were included. We applied random effect model with Knapp-Hartung adjustment for meta-analysis using STATA.16 software and reported outcomes with pooled Weighted Mean (WM).
Results
Pooled WM for BUN was 29.85 (95% CI, 21.25–38.46) in tramadol intoxication and 31.64(95% CI, 12.71–50.57) in MET intoxication. Pooled WM for creatinine in tramadol and MET intoxication was respectively 1.04 (95% CI, 0.84–1.25) and 1.35 (95% CI, 1.13–1.56). Also, pooled WM for CPK was 397.68(376.42-418.94) in tramadol and 909.87(549.98-1269.76) in MET intoxication. No significance was observed in publication bias and heterogeneity tests.
Conclusion
Our findings showed that tramadol or MET intoxication is associated with a considerably increased risk of renal dysfunction that may result in organ failure.
Similar content being viewed by others

Background
Amphetamines refer to both amphetamine (AMPH) and methamphetamines (MET) that are used extra-medically. The main effect site of amphetamines is the central nervous system (CNS) and they can induce an increased sense of alertness, heightened energy and curiosity, elevated mood and attention, and increased interest in environmental stimuli [1]. Acute and long-term MET consumption may result in abnormal findings on examination of the body systems including cardiovascular, CNS, gastrointestinal, and skin [2]. Direct effects of MET and its active metabolites on renal function have been rarely reported. However, acute renal failure (ARF) attributed to MET use is often associated with hyperthermia and/or hemodynamic instability [3]. MET also may cause rhabdomyolysis and related nephropathies such as necrotizing angiitis, acute interstitial nephritis or tubular necrosis, resulting in renal injury [4, 5].
Tramadol, a synthetic opioid analgesic, is widely used across the world [6] and its primary adverse effects are nausea and vomiting, vertigo, fatigue, dry mouth, sweating, and orthostatic hypotension [7]. Tramadol stimulates presynaptic release of serotonin and suppresses serotonin reuptake, resulting in serotonin syndrome [8]. Tramadol overdose can lead to seizure, increase in Creatine phosphokinase (CPK), acute RF, hepatic failure, cardiac arrhythmias and dysfunction [9, 10]. Renal complications attributed to tramadol overdose have been rarely reported [11] and it seems that tramadol-induced seizure can cause renal failure, resulting in elevation of Blood Urea Nitrogen (BUN) and creatinine levels [12].
Regarding the increased use of MET and tramadol in recent years and lack of information about pooled effect size in renal dysfunction, we aimed to conduct a systematic review and meta-analysis of published studies related to renal dysfunction induced by tramadol or MET intoxication in patients presented to the emergency department (ED).
Methods
Information sources and search
We conducted comprehensive research to retrieve all published literature on the topic. For this purpose, we selected the databases\search engine of Scopus, Web of Science, PubMed, and Google Scholar. Also, to deepen the search for related literature, besides reference lists of the included studies, the citations of each selected article in Google Scholar were examined to find possible related articles. The search was performed up to 15 May 2022. We applied two restrictions on the search and selection of studies. The first restriction was in the selection of English-language articles, and the second restriction was the date of publication, which included meta-analysis studies published after 2000. In writing the strategy search, we used both free and controlled (Medical Subject Headings (MeSH) terms. The sample terms of search strategies were as follows: (amphetamine, methamphetamine, tramadol, toxic, overdose, abuser, intoxication, creatine, creatine phosphokinase, creatine kinase, urea, blood urea nitrogen).
Eligibility criteria
The research question in the PICO structure for this review includes; (Patients: intoxicated patients referred to the hospital emergency department), Intervention/Exposure: use of tramadol or MET, Comparison; there is no comparison group in this review, Outcomes; the values of renal function indexes including BUN, creatine, and CPK. Creatinine and BUN are nitrogenous end products of metabolism that are handled primarily by glomerular filtration. They are screening tests of renal function and are valuable in evaluating renal disease. CPK is an intracellular element released by the muscular cell wall into the bloodstream following damage. Many conditions can cause derangement in CPK levels, including rhabdomyolysis, heart disease, kidney disease, or even certain medication. Elevated CPK levels are repeatedly associated with acute renal failure and the need for renal replacement therapy in patients with rhabdomyolysis. We excluded studies with individuals or addicts who have not been intoxicated or existed for other research purposes, case study design, animal studies and children’s study population, and narrative and systematic articles.
Study selection, data items, and Data Collection
Studies were selected by observational design (prospective, retrospective), cross-sectional and case series. In the screening step, duplicate documents were initially managed, and then the recovered documents were screened in terms of the title and abstracts of the published paper. All the literature review, article selection, and data extraction were done by two independent reviewers (A. A, and A. Z). Kappa agreement rate was 84% between reviewers. Disagreements about study selection were resolved via consensus or consultation with third reviewer (K.E). All procedures were performed without blinding and the reviewers were aware of the study information. Relevant information was extracted using a customized datasheet. Basic information (first author, publication year, country, study design, intoxication agent, mean age, sex, and sample sizes) and clinical outcomes of poisoned patients including BUN, creatinine, and CPK at the admission time to ED were extracted. The reviewers contacted authors of eligible studies when additional data was needed.
Risk of bias of included studies
The methodological qualities of included studies were evaluated by two independent reviewers (H.BG and M.S). The Newcastle Ottawa Scale (NOS) was used to evaluate the quality of the methodology [13]. This tool consists of 7 questions in 3 sections (selection, comparability, and outcome) including representativeness of the sample, sample size, non-respondents, ascertainment of the exposure, comparability, assessment of the outcome, statistical test. The quality of each NOS item is marked with a star and total awarded stars (up to ten) indicated the quality of methodology in selected studies. Assessing risk of bias for included studies was based on the JBI critical appraisal tools [14].
Synthesis of results
The mean pooled estimation of renal function indexes was assessed using weighted mean (WM) with a 95% confidence interval (CI). We used random effect model with Knapp-Hartung adjustment method in all analyses for meta-analysis [15]. Knapp-Hartung is used to estimate uncertainty in meta-analysis when the number of studies is small and heterogeneity between studies is low. If the unit of clinical indexes was different, it was converted to a common unit (mg/dl). Also, if the outcomes in the studies were reported in different forms (median and interquartile range (IQR) or mean and standard error (SE), they were converted to mean and standard deviation (SD). Heterogeneity was estimated according to the I2 and chi-square tests and the existence of publication bias was assessed by Egger’s and Begg’s test. Meta-regression and sensitivity analysis were performed to find the source of heterogeneity and robustness of results. Also, GRADE (Grading of Recommendations Assessment, Development and Evaluation) was reported for assessing certainty or confidence in the effect size [16]. The STATA version 16 was used for statistical analysis.
Results
Study selection and characteristics
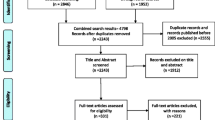
After removing duplicated studies from the various research databases, 1875 documents remained. For the screening based on study hypotheses, it was necessary to read the full text for the final decision in 31 studies, and 8 studies remained finally after this process. Moreover, one related study was included by reviewing citations received from Google Scholar, which included a total of 9 studies to extract data. Figure 1 shows the screening and selection processes of studies.

PRISMA flow diagram of the study selection
Figure 1. PRISMA flow diagram of the study selection.
Demographic information of the studies is described in Table 1. According to the table, there were 4 studies for intoxication with tramadol and 5 studies for MET. The sample size of the total study population was 1884, with an average age of 29.95. Among the papers, 5 studies were conducted in Iran [8, 12, 17,18,19], and 4 studies were done in other nations including United States [20], Australia [21], Thailand [22], and Egypt [23]. In all studies, the percentage of intoxicated men was higher than women. The characteristics of the included studies in the meta-analysis are summarized in Table 1. The results of the methodological quality assessment estimated by NOS were between 7 and 10 stars, which were from acceptable to good quality.
The risk of bias assessment based on the JBI checklist is reported in Table 2.
Synthesis of results and risk of Bias
Overall estimation of renal dysfunction
The pooled estimate of WM for renal function indexes is shown in Table 3, indicating that estimated WM for BUN (31.64 vs. 29.85), creatinine (1.35 vs. 1.04), and CPK (909.87 vs. 397.68) was higher in patients with MET intoxication compare to tramadol.
Heterogeneity and publication bias
Heterogeneity was not seen in all meta-analyses (I2 = 0.0%, and chi-square p > 0.05) except in estimated BUN for MET intoxication. Publication bias was calculated with Egger’s and Begg’s tests and publication bias was not found (p > 0.05) (Table 3).
Meta-regression and sensitivity analysis
According to the results of the heterogeneity test in Table 3, the heterogeneity assumption was approved for all variables except for BUN in MET intoxication. Among the reported variables that contributed probably to heterogeneity, age was considered as a covariate but did not decrease the heterogeneity values in the meta-regression model.
Sensitivity analysis showed that the pooled weighted effect size in all outcomes did not depend on the effect of each study, and the overall effect size did not change after the omission of each study (Fig. 2).

Sensitivity analysis in robustness evaluation of BUN effect size
Certainty meta-analysis
According to the GRADE approach, certainty in the evidence of observational studies in systematic review and meta-analysis started at a low level. Consequently, certainty in outcomes related to the effect size of the evidence started at a low level, as indicated in Table 4.
Discussion
We performed this systematic review and meta-analysis to assess renal function indexes in tramadol and MET-intoxicated patients presenting to the ED of hospitals. The main purpose of the study was to summarize BUN, creatine, and CPK in the blood sample of intoxicated subjects. Our findings of pooled estimate analysis indicated a higher WM for BUN in tramadol and MET intoxication compared to the normal range but WM for creatinine remained within the normal range. Regarding CPK, estimated WM was notably higher in both intoxication with tramadol and MET when compared to the normal range.
Renal dysfunction is a relatively usual condition in intensive care units and several large epidemiologic investigations have reported that nephrotoxic drugs are contributing factors in 19–25% of cases of renal dysfunction in critically hospitalized patients [24]. Serum creatinine has routinely been used to diagnose renal dysfunction, which is defined as an increase in serum creatinine of at least 0.3 mg/dL or 1.5 times baseline [25, 26]. In addition, BUN is another serum marker of renal function, however, it may be altered by non-renal parameters such as catabolic condition, upper gastrointestinal bleeding, hypovolemia, and treatment with high-dose steroids [27, 28]. Serum CPK level also is another efficient biomarker for renal dysfunction in case of chemical intoxication owing to its easy availability and serial monitoring of its level throughout treatment that can predict the prognosis of patients [29].
Amphetamines-induced rhabdomyolysis has been mentioned in several case reports as an adverse effect of MET on the kidney [30]. Rhabdomyolysis is typified by the breakdown of the muscles and release of the intracellular components such as CPK, lactate dehydrogenase, and transaminases into the bloodstream [31]. The pooled WM for CPK in our meta-analysis was 909.87 for MET intoxication which was higher than the normal range (10–120 mcg/L) but lower than the reference value for rhabdomyolysis occurrence (1500 to over 100,000 units/L), indicating some degree of renal injury. Furthermore, pooled WM for creatinine and BUN in MET intoxication was 1.35 (reference range: 0.7–1.3 mg/dL) and 31.64 (reference range: 6–24 mg/dL), respectively. BahramiMotlagh et al., reported total mean CPK of 1471.1 ± 863 units/L in MET body suffers which was higher compared to our pooled WM for CPK. The reason is that some of MET body suffers in their study had ingested MET with heroin, opium, and methadone [17]. Also, mean total CPK reported by Rahimi et al. (1067.9 ± 2981.9 units/L) was higher than our pooled WM for CPK that may be because of positive history of addiction in most of the cases in their study [18]. Furthermore, they observed significant associations between agitation, seizure, and CPK level with mortality due to poisoning with amphetamines [14]. Prior investigations reported that intoxicated patients with CPK serum levels of 10,000 IU/L and higher are at increased risk of nephrotoxicity and renal dysfunction [32].
Tramadol is available in various forms with a 50 mg orally standard therapeutic dose, and 400 mg is the maximum recommended daily dose [33, 34]. Tramadol is spread to the liver, spleen, lungs, brain, and kidneys. The most frequently reported adverse effects of tramadol reported by intoxication are nausea, vomiting, CNS depression, seizure, dizziness, agitation, tachycardia, hypertension, reduced appetite, headache, itching, pruritus and rash, and gastric irritation, and skin eruption [35]. Intoxication with tramadol may also lead to multiple organ failure, coma, cardiopulmonary arrest, and death [36]. In our analysis, the pooled WM for CPK in tramadol intoxication was 397.68 which was relatively higher than the normal range. Regarding creatinine and BUN, the pooled WM respectively was 1.04 and 29.85. However, Mohammadpour et al. reported mean BUN of 38.23 ± 8.3 mg/dL in tramadol toxicity which is relatively higher in comparison with pooled WM for BUN in our analysis. In this regard, they observed the highest concentration of tramadol (491.90 vs. 374.42 QUOTE g/ml) and BUN level (53.33 vs. 23.37 mg/dl) in the seizure group compared to nonseizure cases [12]. A prior experimental investigation found only minimal renal histopathologic changes limited to tubular cells with chronic therapeutic doses of tramadol. In addition, BUN and creatinine levels remained unchanged in intoxication. However, Atici et al. reported a significant increase in creatinine and BUN levels in tramadol intoxication with seizure compared to non-seizure intoxication [11]. Tramadol consumption leads to muscle damage by causing seizures and therefore increased serum levels of CPK could be due to acute renal failure from tramadol poisoning or indirectly following seizure and rhabdomyolysis [12].
Limitations
In our study, final analysis was substantially limited in the number and quality of studies available. The main limitation of the study is the lack of information regarding dose of consumed drugs by patients in the studies. Also, some patients in the reviewed articles may have different history of substance use, which possibly affects the results of study. Another limitation is that the level of renal index (e.g. CPK) in some cases has not been adjusted for the seizure and authors in some articles described only patients’ clinical conditions, which makes it difficult to generalize the results. Lastly, owing to the disparity of results in different countries, more comprehensive research is proposed to make a better conclusion regarding association of tramadol or MET intoxication with changes in renal function indexes.
Conclusion
In conclusion, this systematic review and meta-analysis suggests that tramadol and MET intoxication is associated with a significant rise in renal function indexes. Moreover, our pooled analysis showed that WM of CPK was higher mainly in MET poisoners compared to tramadol. Through this study we indicated that excessive use and intoxication with tramadol and MET increase risk of renal dysfunction and failure. Therefore, clinicians and health care staff in EDs should suspect renal injury in poisoners with MET and tramadol, especially if routine renal indexes are abnormal.
Data Availability
All data generated or analyzed during this study are available from the corresponding author on reasonable request.
Abbreviations
- MET:
-
Methamphetamine
- BUN:
-
Blood Urea Nitrogen
- CPK:
-
Creatine phosphokinase
- WM:
-
Weighted Mean
- AMPH:
-
Amphetamine
- CNS:
-
Central Nervous System
- ARF:
-
Acute Renal Failure
- ED:
-
Emergency Department
- MeSH:
-
Medical Subject Headings
- NOS:
-
Newcastle Ottawa Scale
- CI:
-
Confidence Interval
- IQR:
-
Interquartile Range
- SD:
-
Standard Deviation
- SE:
-
Standard Error
- GRADE:
-
Grading of Recommendations Assessment, Development and Evaluation
References
Mokhtari T, Sheikhazadi A, Hassanzadeh G, Safari M, Sheikhbahaei F, Faghir-Ghanesefat H, et al. Potential adverse effects of amphetamines on kidney; a narrative review on current knowledge. J Ren Injury Prev. 2018;7(4):218–23.
Weng T-I, Chen H-Y, Chin LW, Chou H-H, Wu M-H, Chen G-y et al. Comparison of clinical characteristics between meth/amphetamine and synthetic cathinone users presented to the emergency department. Clin Toxicol. 2022;1–7.
Schep LJ, Slaughter RJ, Beasley DMG. The clinical toxicology of metamfetamine. Clin Toxicol. 2010;48(7):675–94.
Ago M, Ago K, Hara K, Kashimura S, Ogata M. Toxicological and histopathological analysis of a patient who died nine days after a single intravenous dose of methamphetamine: a case report. Leg Med. 2006;8(4):235–9.
Richards JR, Laurin EG. Methamphetamine toxicity. StatPearls [Internet]: StatPearls Publishing; 2021.
Nakhaee S, Amirabadizadeh A, Brent J, Miri-Moghaddam E, Foadoddini M, Farrokhfall K, et al. Tramadol and the occurrence of seizures: a systematic review and meta-analysis. Crit Rev Toxicol. 2019;49(8):710–23.
Ahmadimanesh M, Shadnia S, Rouini MR, Sheikholeslami B, Nasab SA, Ghazi-Khansari M. Correlation between plasma concentrations of tramadol and its metabolites and the incidence of seizure in tramadol-intoxicated patients. Drug Metabolism and Personalized Therapy. 2018;33(2):75–83.
Tashakori A, Afshari R. Tramadol overdose as a cause of serotonin syndrome: a case series. Clin Toxicol. 2010;48(4):337–41.
Afshari R, Tashakori A, Shakiba A, editors. Tramadol overdose induced CPK rise, haemodynamic and electocardiographic changes and seizure. Clinical toxicology. New York: Informa Healthcare.Vanderbilt Ave; 2008. Ny 10017 Usa.
Habibollahi P, Garjani A, Vahdati SS, Seyyed-Reza SE, Parnianfard N, Zakeri R. Characteristics of patients with tramadol use or abuse: a systematic review and Meta-analysis. Eurasian J Emerg Med. 2020;19(3):127.
Atici S, Cinel I, Cinel L, Doruk N, Eskandari G, Oral U. Liver and kidney toxicity in chronic use of opioids: an experimental long term treatment model. J Biosci. 2005;30(2):245–52.
Mohammadpour A, Ashkezari MD, Farahmand B, Shokrzadeh M. Demographic characteristics and functional performance of the kidneys and hearts of patients with acute tramadol toxicity. Drug Res. 2019;69(04):207–10.
Modesti P, Reboldi G, Cappuccio F. Newcastle-Ottawa Quality Assessment Scale (adapted for cross sectional studies). PLoS ONE. 2016;11(1):e0147601.
Munn Z, Barker TH, Moola S, Tufanaru C, Stern C, McArthur A, Stephenson M, Aromataris E. Methodological quality of case series studies: an introduction to the JBI critical appraisal tool. JBI Evid synthesis. 2020;18(10):2127–33.
Jackson D, Law M, Rücker G, Schwarzer G. The Hartung-Knapp modification for random‐effects meta‐analysis: a useful refinement but are there any residual concerns? Stat Med. 2017;36(25):3923–34.
Schünemann H, Brożek J, Guyatt G, Oxman A. Handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach. Updated October. 2013;2013.
Bahrami-Motlagh H, Hassanian-Moghaddam H, Zamini H, Zamani N, Gachkar L. Correlation of abdominopelvic computed tomography with clinical manifestations in methamphetamine body stuffers. Radiol Med. 2018;123(2):98–104.
Rahimi M, Lookzadeh S, Sadeghi R, Soltaninejad K, Shadnia S, Pajoumand A et al. Predictive factors of mortality in acute amphetamine type stimulants poisoning; a review of 226 cases. Emergency. 2018;6(1).
Rahimi HR, Soltaninejad K, Shadnia S. Acute tramadol poisoning and its clinical and laboratory findings. J Res Med sciences: official J Isfahan Univ Med Sci. 2014;19(9):855.
Richards JR, Wang CG, Fontenette RW, Stuart RP, McMahon KF, Turnipseed SD. Rhabdomyolysis, methamphetamine, amphetamine and MDMA use: Associated factors and risks. J Dual Diagnosis. 2020;16(4):429–37.
Isoardi KZ, Mudge DW, Harris K, Dimeski G, Buckley NA. Methamphetamine intoxication and acute kidney injury: a prospective observational case series. Nephrology. 2020;25(10):758–64.
Suriyaprom K, Tanateerabunjong R, Tungtrongchitr A, Tungtrongchitr R. Alterations in malondialdehyde levels and laboratory parameters among methamphetamine abusers. J Med Association Thailand = Chotmaihet thangphaet. 2011;94(12):1533–9.
Ismail MA, Mahmoud SF, Khedr MA, Mohammed MK. Assessment of cases of Acute Tramadol Toxicity as Regards Clinical, Laboratory and Management Procedures in some University Hospitals in Cairo. Egypt J Hosp Med. 2018;72(1).
Perazella MA, Rosner MH. Drug-induced acute kidney injury. Clin J Am Soc Nephrol. 2022;17(8):1220–33.
Van Biesen W, Vanholder R, Lameire N. Defining acute renal failure: RIFLE and beyond. Clin J Am Soc Nephrol. 2006;1(6):1314–9.
Bellomo R, Kellum JA, Ronco C. Defining and classifying acute renal failure: from advocacy to consensus and validation of the RIFLE criteria. Intensive Care Med. 2007;33(3):409–13.
van Meer L, Moerland M, Cohen AF, Burggraaf J. Urinary kidney biomarkers for early detection of nephrotoxicity in clinical drug development. Br J Clin Pharmacol. 2014;77(6):947–57.
Griffin BR, Faubel S, Edelstein CL. Biomarkers of Drug-Induced kidney toxicity. Ther Drug Monit. 2019;41(2):213–26.
Bhattacharyya K, Phaujdar S, Sarkar R, Mullick OS. Serum creatine phosphokinase: a probable marker of severity in organophosphorus poisoning. Toxicol Int. 2011;18(2):117–23.
Cervellin G, Comelli I, Lippi G. Rhabdomyolysis: historical background, clinical, diagnostic and therapeutic features. Clin Chem Lab Med. 2010;48(6):749–56.
Zutt R, Van Der Kooi A, Linthorst G, Wanders R, De Visser M. Rhabdomyolysis: review of the literature. Neuromuscul Disord. 2014;24(8):651–9.
Pajoum A, Fahim F, Akhlaghdoust M, Zamani N, Amirfirooz Z, Dehdehasti M. Rhabdomyolysis and Acute Poisoning; a brief report. Emerg. 2018;6(1):e56–e.
Grond S, Sablotzki A. Clinical pharmacology of tramadol. Clin Pharmacokinet. 2004;43(13):879–923.
Gong L, Stamer UM, Tzvetkov MV, Altman RB, Klein TE. PharmGKB summary: tramadol pathway. Pharmacogenet Genomics. 2014;24(7):374.
Nakhaee S, Hoyte C, Dart RC, Askari M, Lamarine RJ, Mehrpour O. A review on tramadol toxicity: mechanism of action, clinical presentation, and treatment. Forensic Toxicol. 2021;39(2):293–310.
Mehrpour O, Sharifi M, Zamani N. Tramadol poisoning. In: Andreazza AC, Scola G, editors. Toxicology studies cells, drugs and environment. BoD, Books on Demand; 2015.
Acknowledgements
We appreciate the methodological consultants of the Trauma and Injury Research Center of Iran University of Medical Sciences, especially Mr. Pouya Hedayati, who was involved in managing the review process and planning activities. Other people who were involved in this study were included in the list of authors of the manuscript.
Funding
We must first mention that this study and also the authors did not receive any grants from any agencies or organizations.
Author information
Authors and Affiliations
Contributions
The authors’ responsibilities were as follows AA, KE, and SS designed the study; AA, AZ, and KE screened and selected the studies; AA and AZ extracted the data; MS, HBG, and AA assessed the risk of bias; YM and AA analyzed the data; AA, HBG, AZ, and MS drafted the manuscript; YM, SS and KE modified the final manuscript; and all authors: read and approved the final manuscript.
Corresponding authors
Ethics declarations
Identification code in prospero
CRD42022321523.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
At all the stages of the study; searching and selecting articles, data extraction, analysis and interpretation of results, all ethics in research and data originality were preserved. Finally, authors declare that they have no competing interests associated with this manuscript.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Amanollahi, A., Mehrabi, Y., Sedighi, M. et al. Assessment of renal function indexes in methamphetamine or tramadol intoxication adults to the emergency departments: a systematic review and meta-analysis. BMC Emerg Med 23, 89 (2023). https://doi.org/10.1186/s12873-023-00855-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12873-023-00855-1