
Abstract
Background
The association of hypertension (HTN) and different types of dietary amino acids is not yet clear. The aim of the present study was to investigate the association of branch chain amino acids (BCAAs) and the prevention of HTN.
Methods
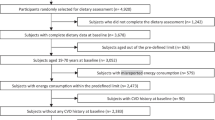
This cross-sectional study was conducted on 4184 people aged 35 to 70 using data from the Sabzevar Persian cohort study in Sabzevar, Iran. Data on dietary intake of BCAAs including leucine, isoleucine, and valine were obtained using a validated Food Frequency Questionnaire (FFQ). Multivariable logistic regression analysis assessed the link between HTN and BCAAs.
Results
The results showed that participants with HTN had a higher total protein and BCAAs intake than participants with normal BP (P < 0.01). A marginally significant association was found between the risk of HTN with the total intake of BCAAs (OR = 1.018, CI95%: 1.001–1.035, P = 0.04), leucine (OR = 1.040, CI95%:1.002–1.080, P = 0.03), isoleucine (OR = 1.068, CI95%:1.001–1.140, P = 0.04), and valine (OR = 1.060, CI95%:1.003–1.121, P = 0.04). However, the association disappeared after adjusting the total protein and calorie intake.
Conclusions
The results indicated that the dietary intake of BCAAs may be associated with the risk of HTN. Future longitudinal research is warranted.
Similar content being viewed by others


Introduction
Hypertension (HTN) is a chronic disease characterized by elevated blood pressure (BP) [1], which is typically the cause of numerous cardiovascular disorders such as coronary artery disease, stroke, and heart failure [2]. HTN affects more than one billion adults worldwide [3], and the global number of people living with HTN will reach two billion by 2025 [4]. The prevalence of hypertension among adults is higher in low and middle-income countries (LMICs), affecting 31.5% of the population (1.04 billion people), compared to high-income countries (HICs), where it affects 28.5% of the population (349 million people) [5]. According to the American College of Cardiology/American Heart Association (ACC/AHA), in 2017, approximately 46% of Americans have HTN [6]. In China, a significant increase was reported in the prevalence of HTN among adults aged 20 years and older, from 25.7% in 2007 to 31.5% in 2017 [7]. Based on findings of the population-based national surveys in Iran, the prevalence of HTN increased from 14.66% in 2009 to 32.03% in 2021 [5].
HTN is affected by many factors including lifestyle [8], overweight [9], and dietary components such as sodium [10]. Dietary modifications are considered a beneficial strategy in the treatment of HTN [11, 12]. The association between dietary proteins and HTN has recently received increased attention due to their potential role in cardiovascular function [13]. Dietary protein intake was reported to be associated with both systolic and diastolic BP [13, 14]. However, data regarding the possible effects of different types of dietary protein on HTN are inconsistent [14, 15].
BCAAs comprising leucine, isoleucine, and valine have an aliphatic side-chain with a branch, a unique structure that allows them to be metabolized primarily in the muscles rather than the liver, unlike other amino acids [16]. These amino acids are abundant in animal proteins such as meat, fish, dairy products, and eggs, as well as in legumes, which are plant sources of dietary protein. An adequate intake of BCAAs is required for body protein synthesis, production of energy, and several metabolic functions [17, 18], glucose metabolism, and regulation of some pivotal pathways [19, 20].
BCAAs have been previously reported to be inversely related to BP [21]. On the other hand, some other studies have suggested that higher levels of circulating BCAAs are positively associated with HTN [14, 22]. Alterations in BCAAs metabolism leading to aggregation of BCAAs and their byproducts are associated with significant metabolic disorders such as insulin resistance and an increased risk of HTN [23, 24]. In addition, BCAAs intake diminishes brain tyrosine and tryptophan uptake and may decrease catecholamine and serotonin synthesis, adversely affecting central BP regulation [25, 26].
Although many studies have examined the relationship between individual essential amino acids in the form of plant or animal protein categories with BP [27, 28], the association of different types of BCAAs with HTN is not yet clear. Considering the high prevalence of hypertension in adults worldwide [4] and to test whether the BCAAs could be positively and negatively related to BP, the present study was conducted to investigate the association of BCAAs with the risk of HTN.
Methods
Study population
This cross-sectional study was carried out on Iranian adults using Sabzevar Persian cohort data, which was performed from January 2017 to May 2020 on 4184 people including 1239 people with HTN and 2945 people without HTN in Sabzevar, Iran. Inclusion criteria included age between 35 and 70 years, no family history of HTN, no history of kidney diseases, no treatment with drugs affecting BP, and no history of BCAAs supplementation. Exclusion criteria included the inability to collect the required data.
Data collection
The Persian cohort questionnaires collected data on general and socio-demographic factors, medical status, and dietary intake through interviews and physical examinations. The SECA 755 mechanical column scale and SECA 204 mobile stadiometer were used to measure weight and height without shoes in light clothes to the nearest 100 g and 0.5 cm, respectively. The participants’ BMI was then calculated as weight (kg)/height2 (m2) [29].
The Persian cohort food frequency questionnaire (FFQ) was used to evaluate dietary intake, and its validity and reliability have already been confirmed [30]. The collected data on dietary intake was assessed using the Nutritionist IV software regarding dietary calories, total protein, and BCAAs. In this study, the amount of food consumed by each person during the last year was assessed, and the total amount of BCAAs intake was estimated using the amount of BCAAs in each food item based on the USDA food database.
BP was measured in the morning after 10 min rest period twice in each arm supported at heart level in a seated position of the participants with their back supported and legs uncrossed in a quiet room after ten-minute intervals, using Richter auscultator mercury sphygmomanometers (MTM Munich, Germany) with appropriately adjusted cuff size [29]. The participants were advised to avoid coffee (and other sources of caffeine) before checking their BP. The average of the measurements was used in the analyses.
Statistical analysis
The independent t-test or Mann-Whitney test (for non-parametric variables) was used to compare quantitative data, and the chi-square test was used to compare qualitative variables between the participants with and without HTN. Hypertension was defined as systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥ 90 mmHg [31]. A logistic regression test was used to assess the association between HTN as a categorical variable and dietary intake of BCAAs as a continuous variable. The confounders were adjusted using different models of logistic regression including the crude model (Model 1), adjusted for age and gender (Model 2), further adjustments for education, marital status, job, physical activity, BMI, and diabetes (Model 3), and additional adjustments for the intake of energy, protein and other amino acids (Model 4). Kolmogorov-Smirnov test assessed the normal distribution of data, and all analyses were performed using SPSS version 21, considering the significant level at P < 0.05.
Results
In total, 4184 people including 2945 people with normal BP and 1239 with HTN participated in the study. The participants with HTN had higher age (53.45 ± 8.3 vs. 47.46 ± 8.35 y), height (163.32 ± 9. 5 vs. 161.75 ± 9.1 cm), weight (78.01 ± 14. 2 vs. 72.51 ± 12.8 kg), body mass index (BMI) (29.23 ± 4.7 vs. 27.76 ± 4. 7 kg/m2), right arm systolic BP (RSBP) (134.12 ± 13 vs. 106.23 ± 10. 6 mmHg), and right arm diastolic BP (RDBP) (All P < 0.01). Also, the patients with HTN had higher occupation and diabetes and lower education compared to the participants without HTN (Table 1).
Regarding dietary intake of the participants, patients with HTN had a higher intake of calorie (2549.93 ± 818.39 vs. 2477.77 ± 770.36 kcal/d), total protein (79.98 ± 26.79 vs. 78.14 ± 25.74 g/d), carbohydrate (425.44 ± 144.70 vs. 407.77 ± 135.06 g/d), isoleucine (3.12 ± 1.05 vs. 3.05 ± 1.01 g/d), leucine (5.36 ± 1.82 vs. 3.75 ± 1.33 g/d), valine (3.67 ± 1.23 vs. 3.06 ± 1.01 g/d), and lower intake of fats (64.31 ± 25.06 vs. 64.58 ± 25.06 g/d) and cholesterol (256.17 ± 121.66 vs. 261.19 ± 120.39 mg/d) compared to the participants without HTN (All P < 0.01) (Table 2).
Multivariate logistic regression analysis found that HTN had a marginally positive association with total intake of BCAAs and the intake of different types of BCAAs (All P < 0.05) (Table 3, Model 1). After adjusting for age and gender, the association between HTN and total intake of BCAAs (OR = 1.03, CI95%: 1.01–1.05, P = 0.01), leucine (OR = 1.06, CI95%:1.01–1.11, P = 0.01), isoleucine (OR = 1.11, CI95%:1.02–1.19, P = 0.01), and valine (OR = 1.09, CI95%:1.02–1.16, P = 0.01) remained significant (Model 2). The results did not change after additional adjustments for education, marital status, job, diabetes, physical activity, and BMI (Model 3). The associations disappeared after further adjustments for energy intake, total protein intake, and other amino acids (Model 4).
Discussion
The results of the present study indicated that participants with HTN had a higher intake of total protein and BCAAs than participants with normal BP. Moreover, there was a significant positive association between BP and higher dietary intake of BCAAs. However, the association disappeared after the adjustment of the total protein and calorie intake. Higher intake of BCAAs may increase the risk of HTN through increased consumption of dietary proteins. The present study’s results regarding the association between BCAAs and high BP are consistent with some previous studies [21, 32,33,34,35,36]. For example, Teymoori et al. in a population-based prospective study on 4288 adults reported a positive relationship between the dietary amino acids including BCAAs and increased risk of HTN [32]. Two Asian studies also reported similar findings of a positive relationship between BCAAs and Aromatic Amino Acids (AAAs) with HTN [35, 36]. The ratio of the intake of different types of amino acids can also influence the risk of HTN. Teymoori et al. in a recent study on the ratio of different dietary amino acids found that the Leucine–Serine/Threonine–Tryptophan ratio was positively associated with the risk of HTN [33].
Moreover, the observation of previous studies that high levels of circulating BCAAs are positively associated with increased risk of HTN is in line with our results [23, 37,38,39]. On the other hand, animal proteins as rich sources of BCAAs are frequently reported to be associated with HTN [40,41,42]. Nevertheless, in contrast with the results of this study, Jennings et al., in the Twin UK cohort study, found that higher intakes of BCAAs were associated with decreased risk of HTN [43]. Moreover, a Chinese study observed no association between HTN and serum BCAAs levels [44]. A possible cause of these contradictory results is that the effects of BCAAs on BP may be influenced by the total amount of dietary protein, calorie intake, and the level of other nutrients. For example, whey protein is rich in both lactokinins and BCAAs, the first of which has inhibitory properties on the angiotensin-converting enzyme and BCAAs may have an adverse effect on BP; thus, whey protein intake may have both positive and negative impact on hypertension [45].
The exact mechanism of the effect of BCAAs on BP is not clear. Various biochemical mechanisms may explain the observed findings of the impact of BCAAs on BP. It has been shown that alterations in BCAAs metabolism, leading to the aggregation of BCAAs and their byproducts, are linked to striking metabolic derangements such as insulin resistance, the latter being related to an increased risk of HTN [23, 24]. The accumulation of BCAAs and their byproducts can cause impairments in the function of the mammalian target of rapamycin complex 1 (mTORC1) and overstimulation of adenosine monophosphate-activated protein kinase (AMPK), which subsequently leads to insulin resistance and plays a key role in the development of HTN. Also, AAAs and BCAAs have hydrophobic residues that can be relevant to binding bioactive peptides to the angiotensin-converting enzyme, which is crucial in controlling BP [46].
Moreover, high serum levels of serine and BCAAs can play a role in HTN by reducing the entry of threonine, tryptophan, and glutamic acid into the brain, consequently diminishing the synthesis of BP-beneficial neurotransmitters [47, 48]. For example, BCAAs reduce tyrosine and tryptophan transport and serotonin synthesis [48] by competing with tryptophan for entrance to the brain [49]. Serotonin is the primary metabolite of tryptophan, which has a vasodilatory effect through nitric oxide (NO) production [50]. Decreased or impaired serotonin synthesis has been reported in patients with HTN, and a previous study reported a link between increased BP and decreased serotonin synthesis [51]. BCAAs (especially leucine) and their metabolites can also affect BP through adverse effects on insulin sensitivity [52]. Indeed, salt absorption in the proximal tubule is enhanced in humans with insulin resistance due to the preservation of the stimulatory effect of insulin (compensatory hyperinsulinemia) on salt reabsorption in the kidney proximal tubule, resulting in a state of salt overload and HTN [24, 52].
The strengths of current study were a large sample size within a population-based study, allowing generalization of findings to the whole population. However, this study had some limitations. First, despite adjusting for a wide range of variables, the effect of some unknown and unmeasured confounders may have remained. Second, the lack of analysis of the serum BCAAs concentrations and reliance on dietary intake of BCAAs ignores essential factors such as the levels of protein cleavage and amino acid absorption in the gut lumen. Third, the utilization of an FFQ for dietary intake assessment constitutes a limitation due to potential recall bias and the inherent inaccuracies associated with self-reported dietary data, which can compromise the reliability and validity of the findings. More longitudinal studies are needed to confirm the results of the present study.
Conclusion
In conclusion, the provided data suggest that higher intakes of BCAAs are associated with a higher risk of HTN. If these results are confirmed, a lower intake of BCAAs-rich foods can be considered as a dietary recommendation against HTN. Further research based on direct measurements of amino acids in plasma should be prompted to achieve better and more realistic findings. Clinical trial studies are also needed to confirm these findings and determine the interplay between amino acid metabolism and HTN and whether a high level of these amino acids affects the risk of chronic diseases, especially high BP.
Data availability
Datasets used and analyzed during the current study are available from the corresponding author on reasonable requests.
References
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA. 2003;289(19):2560–71.
Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJ, Group CRAC. Selected major risk factors and global and regional burden of disease. Lancet. 2002;360(9343):1347–60.
Beaney T, Schutte AE, Stergiou GS, Borghi C, Burger D, Charchar F, et al. May Measurement Month 2019: the global blood pressure screening campaign of the International Society of Hypertension. Hypertension. 2020;76(2):333–41.
Feng Y, Guan S, Xu Y, Chen W, Huang X, Wang X et al. Effects of the two-Dimensional structure of Trust on Patient Adherence to Medication and non-pharmaceutical treatment: a cross-sectional study of rural patients with essential hypertension in China. Front Public Health. 2022;10.
Mills KT, Bundy JD, Kelly TN, Reed JE, Kearney PM, Reynolds K, et al. Global disparities of hypertension prevalence and control: a systematic analysis of Population-Based studies from 90 countries. Circulation. 2016;134(6):441–50.
Muntner P, Carey RM, Gidding S, Jones DW, Taler SJ, Wright JT Jr, et al. Potential US population impact of the 2017 ACC/AHA high blood pressure guideline. Circulation. 2018;137(2):109–18.
Li Y, Teng D, Shi X, Teng X, Teng W, Shan Z, et al. Changes in the prevalence of obesity and hypertension and demographic risk factor profiles in China over 10 years: two national cross-sectional surveys. Lancet Reg Health-Western Pac. 2021;15:100227.
Pickering TG. Mental stress as a causal factor in the development of hypertension and cardiovascular disease. Curr Hypertens Rep. 2001;3(3):249–54.
Chiang BN, Perlman LV, Epstein FH. Overweight and hypertension: a review. Circulation. 1969;39(3):403–21.
Coleman TG, Guyton AC. Hypertension caused by salt loading in the dog. Circul Res. 1969;25(2):153–60.
Geleijnse JM, Grobbee D, Kok F. Impact of dietary and lifestyle factors on the prevalence of hypertension in western populations. J Hum Hypertens. 2005;19(3):S1–4.
Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 Practice guidelines for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. Blood Press. 2018;27(6):314–40.
Teunissen-Beekman KF, van Baak MA. The role of dietary protein in blood pressure regulation. Curr Opin Lipidol. 2013;24(1):65–70.
–van der Altorf W, Engberink MF, Brink EJ, van Baak MA, Bakker SJ, Navis G, et al. Dietary protein and blood pressure: a systematic review. PLoS ONE. 2010;5(8):e12102.
Rebholz CM, Friedman EE, Powers LJ, Arroyave WD, He J, Kelly TN. Dietary protein intake and blood pressure: a meta-analysis of randomized controlled trials. Am J Epidemiol. 2012;176(suppl7):S27–43.
Gorissen SH, Phillips SM. Branched-chain amino acids (leucine, isoleucine, and valine) and skeletal muscle. Nutrition and skeletal muscle: Elsevier; 2019. pp. 283–98.
Zazpe I, Ruiz-Canela M. Effect of branched-chain amino acid supplementation, dietary intake and circulating levels in cardiometabolic diseases: an updated review. Curr Opin Clin Nutr Metabolic Care. 2020;23(1):35–50.
Holeček M. Branched-chain amino acids in health and disease: metabolism, alterations in blood plasma, and as supplements. Nutr Metabolism. 2018;15(1):1–12.
Burrage LC, Nagamani SC, Campeau PM, Lee BH. Branched-chain amino acid metabolism: from rare mendelian diseases to more common disorders. Hum Mol Genet. 2014;23(R1):R1–8.
Fernstrom JD. Branched-chain amino acids and brain function. J Nutr. 2005;135(6):S1539–46.
Flores-Guerrero JL, Groothof D, Connelly MA, Otvos JD, Bakker SJ, Dullaart RP. Concentration of branched-chain amino acids is a strong risk marker for incident hypertension. Hypertension. 2019;74(6):1428–35.
Liu Y, Zhang C, Zhang Y, Jiang X, Liang Y, Wang H, et al. Association between excessive dietary branched-chain amino acids intake and hypertension risk in Chinese population. Nutrients. 2022;14(13):2582.
Batch BC, Shah SH, Newgard CB, Turer CB, Haynes C, Bain JR, et al. Branched chain amino acids are novel biomarkers for discrimination of metabolic wellness. Metabolism. 2013;62(7):961–9.
Soleimani M. Insulin resistance and hypertension: new insights. Kidney Int. 2015;87(3):497–9.
Fernstrom JD. Large neutral amino acids: dietary effects on brain neurochemistry and function. Amino Acids. 2013;45(3):419–30.
Choi S, DiSilvio B, Fernstrom MH, Fernstrom JD. Effect of chronic protein ingestion on tyrosine and tryptophan levels and catecholamine and serotonin synthesis in rat brain. Nutr Neurosci. 2011;14(6):260–7.
Poggiogalle E, Fontana M, Giusti AM, Pinto A, Iannucci G, Lenzi A, et al. Amino acids and hypertension in adults. Nutrients. 2019;11(7):1459.
Richter CK, Skulas-Ray AC, Champagne CM, Kris-Etherton PM. Plant protein and animal proteins: do they differentially affect cardiovascular disease risk? Adv Nutr. 2015;6(6):712–28.
Poustchi H, Eghtesad S, Kamangar F, Etemadi A, Keshtkar A-A, Hekmatdoost A, et al. Prospective epidemiological research studies in Iran (the PERSIAN Cohort Study): rationale, objectives, and design. Am J Epidemiol. 2018;187(4):647–55.
Eghtesad S, Hekmatdoost A, Faramarzi E, Homayounfar R, Sharafkhah M, Hakimi H et al. Validity and reproducibility of a food frequency questionnaire assessing food group intake in the PERSIAN Cohort Study. Front Nutr. 2023;10.
Van De Borne P. Guidelines for the management of arterial hypertension. Acta Cardiol. 2014;69(1):53–4.
Teymoori F, Asghari G, Mirmiran P, Azizi F. Dietary amino acids and incidence of hypertension: a principle component analysis approach. Sci Rep. 2017;7(1):16838.
Teymoori F, Asghari G, Farhadnejad H, Mirmiran P, Azizi F. Do dietary amino acid ratios predict risk of incident hypertension among adults? Int J Food Sci Nutr. 2019;70(4):387–95.
Siomkajło M, Rybka J, Mierzchała-Pasierb M, Gamian A, Stankiewicz-Olczyk J, Bolanowski M, et al. Specific plasma amino acid disturbances associated with metabolic syndrome. Endocrine. 2017;58:553–62.
Yamaguchi N, Mahbub M, Takahashi H, Hase R, Ishimaru Y, Sunagawa H, et al. Plasma free amino acid profiles evaluate risk of metabolic syndrome, diabetes, dyslipidemia, and hypertension in a large Asian population. Environ Health Prev Med. 2017;22:1–8.
Yang R, Dong J, Zhao H, Li H, Guo H, Wang S, et al. Association of branched-chain amino acids with carotid intima-media thickness and coronary artery disease risk factors. PLoS ONE. 2014;9(6):e99598.
Flores-Guerrero JL, Groothof D, Connelly MA, Otvos JD, Bakker SJL, Dullaart RPF. Concentration of branched-chain amino acids is a strong risk marker for Incident Hypertension. Hypertension. 2019;74(6):1428–35.
Perng W, Rifas-Shiman SL, Hivert MF, Chavarro JE, Oken E. Branched chain amino acids, androgen hormones, and metabolic risk across early adolescence: a prospective study in Project viva. Obes (Silver Spring). 2018;26(5):916–26.
Magnusson M, Lewis GD, Ericson U, Orho-Melander M, Hedblad B, Engström G, et al. A diabetes-predictive amino acid score and future cardiovascular disease. Eur Heart J. 2013;34(26):1982–9.
Tzoulaki I, Brown IJ, Chan Q, Van Horn L, Ueshima H, Zhao L, et al. Relation of iron and red meat intake to blood pressure: cross sectional epidemiological study. BMJ. 2008;337:a258.
Wang YF, Yancy WS Jr., Yu D, Champagne C, Appel LJ, Lin PH. The relationship between dietary protein intake and blood pressure: results from the PREMIER study. J Hum Hypertens. 2008;22(11):745–54.
Tielemans SM, Kromhout D, Altorf-van der Kuil W, Geleijnse JM. Associations of plant and animal protein intake with 5-year changes in blood pressure: the Zutphen Elderly Study. Nutr Metab Cardiovasc Dis. 2014;24(11):1228–33.
Jennings A, MacGregor A, Pallister T, Spector T, Cassidy A. Associations between branched chain amino acid intake and biomarkers of adiposity and cardiometabolic health independent of genetic factors: a twin study. Int J Cardiol. 2016;223:992–8.
Hu W, Sun L, Gong Y, Zhou Y, Yang P, Ye Z et al. Relationship between branched-chain amino acids, metabolic syndrome, and cardiovascular risk profile in a Chinese population: a cross-sectional study. International journal of endocrinology. 2016;2016.
Pal S, Ellis V. Acute effects of whey protein isolate on blood pressure, vascular function and inflammatory markers in overweight postmenopausal women. Br J Nutr. 2011;105(10):1512–9.
Martin M, Deussen A. Effects of natural peptides from food proteins on angiotensin converting enzyme activity and hypertension. Crit Rev Food Sci Nutr. 2019;59(8):1264–83.
Tovar A, Tews JK, Torres N, Harper AE. Some characteristics of threonine transport across the blood-brain barrier of the rat. J Neurochem. 1988;51(4):1285–93.
Wessels AG, Kluge H, Hirche F, Kiowski A, Schutkowski A, Corrent E, et al. High leucine diets stimulate cerebral branched-chain amino acid degradation and modify serotonin and ketone body concentrations in a pig model. PLoS ONE. 2016;11(3):e0150376.
Fernstrom JD, Wurtman RJ. Brain serotonin content: physiological regulation by plasma neutral amino acids. Science. 1972;178(4059):414–6.
McKean CM. The effects of high phenylalanine concentrations on serotonin and catecholamine metabolism in the human brain. Brain Res. 1972;47(2):469–76.
Guicheney P, Baudouin-Legros M, Valtier D, Meyer P. Reduced serotonin content and uptake in platelets from patients with essential hypertension: is a ouabain-like factor involved? Thromb Res. 1987;45(4):289–97.
McCormack SE, Shaham O, McCarthy MA, Deik AA, Wang TJ, Gerszten RE, et al. Circulating branched-chain amino acid concentrations are associated with obesity and future insulin resistance in children and adolescents. Pediatr Obes. 2013;8(1):52–61.
Acknowledgements
The research was financially supported by Sabzevar University of Medical Sciences, Sabzevar, Iran.
Funding
The research was funded by Sabzevar University of Medical Sciences, Sabzevar, Iran (Code 402043).
Author information
Authors and Affiliations
Contributions
ZS, BA, PA, AA, MM, MT, MSM, ZM, SHT, NV and SD designed the study, involved in the data collection, analysis, and drafting of the manuscript. SD, SKH, MGH and MGH were involved in the design of the study, analysis of the data, and critically reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethical Committee of the Research Ethics Committee of the sabzevar University of Medical Sciences, Sabzevar, Iran. (code: IR.MEDSAB.REC.1400.040). All procedures of the studies involving human participants were by the ethical standards of the institutional and/or national research committee and the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. All participants signed informed consent forms. Informed consent was obtained from the adolescents and their parents to participate in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Salimi, Z., Aminnezhad Kavkani , B., Allahyari, P. et al. Branched-chain amino acids and the risk of hypertension; a persian cohort-based study. BMC Cardiovasc Disord 24, 397 (2024). https://doi.org/10.1186/s12872-024-04045-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-024-04045-0