
Abstract
Clinical risk factors associated obesity and smoking, as well as their combined effect, are not fully understood. This study aims to determine sex differences in risk factors in a population of acute ischemic stroke (AIS) patients who are obese and with a history of previous or current smoking.
Methods
A retrospective analysis of risk factors in male and female AIS patients with baseline data of obesity and current or previous history of smoking, smoking, and obesity alone was determined. The primary predictor and outcome are risk factors associated with male and female AIS patients. Baseline risk factors were analyzed using a multivariate regression analysis to determine specific risk factors linked with the combined effect of obesity and current or previous history of smoking’’.
Results
Male obese AIS patients who are current or previous smokers were more likely to be older patients(OR = 1.024, 95% CI, 1.022–1.047, P = 0.033) that present with coronary artery disease (OR = 1.806, 95% CI, 1.028–3.174, P = 0.040), a history of alcohol use (OR = 2.873, 95% CI, 1.349–6.166, P = 0.006), elevated serum creatinine (OR = 4.724, 95% CI, 2.171–10.281, P < 0.001) and systolic blood pressure (OR = 1.029, 95% CI, 1.011–1.047, P < 0.002). Females were more associated with depression (OR = 0.432, 95% CI, 0.244–0.764, P = 0.004), previous TIA (OR = 0.319, 95% CI, 0.142–0.714, P < 0.005), and higher levels of HDL (OR = 0.938, 95% CI, 0.915–0.962, P < 0.001).
Conclusion
Our results reveal sex differences in risk factors in obese AIS patients with a current or past history of smoking. This finding emphasizes the need to develop management strategies to improve the care of obese AIS patients who are either current or former smokers.
Similar content being viewed by others


Introduction
Despite substantial progress in research focusing on sex differences in comorbidities influencing outcomes in male and female post-stroke patients who smoke [1,2,3], there are still major research gaps in stroke risk factors specific for male and female smokers and obese individuals. While several studies have shown that smoking is not associated with an increase in body weight [4], smoking is known to be associated with central obesity [5, 6]. Interestingly, only males that are former smokers were reported to be at risk of central obesity [5]. Obesity and smoking have each been linked to cerebrovascular diseases including stroke [7, 8]. In addition, obese individuals who are smokers present with a risk of circulatory and cerebrovascular diseases with increased mortality by 7- to 10-fold for smokers compared to normal-weight and non-smokers [9]. Both smoking and obesity have been linked to increased incidence of stroke in both male and female AIS patients [10, 11], but sex differences in obese AIS patients with a current or previous history of smoking are not fully understood.
While stroke ranks as the fourth leading cause of death among individuals aged 20 to 59, it emerges as the second leading cause of death in females aged 60 and over [12, 13]. Among those aged 45–74, males exhibit a higher rate of stroke and mortality. However, beyond the age of 74, females tend to surpass males in both stroke incidence and mortality [14, 15]. Females often present with worse baseline function, more comorbidities, poorer post-stroke outcomes, and an overall greater risk for stroke compared with males [16, 17]. In addition, stroke severities, and deaths linked to a stroke are less in males than females [18]. The higher severity and death rate in females is linked to the older age of females at stroke onset and the fact that females present with longer life expectancy compared with males [19, 20].
Prospective studies provided evidence for the effects of risk factors on the risk of stroke, and most of the risk factors are at the disadvantage of females [21, 22]. For example, diabetes causes more risk of stroke in females than in males [23, 24]. Similarly, a history of atrial fibrillation was associated with a higher risk of stroke in females compared with males [21, 25]. In terms of smoking and obesity, more than 25% of males and 6% of females are reported to smoke every day [26, 27], and smoking alone or in combination with obesity poses a major risk for stroke for both males and females compared with non-obese or smoking individuals [28, 29]. While obesity is reported to be more prevalent in females than males [30, 31], males tend to smoke at higher rates than females [32, 33].
Given that there is a stronger association between more risk factors and the severity of stroke in females compared with males [34], it is possible that risk factors for ischemic stroke in individuals with a combination of obesity and smoking may not be equally distributed between females and males. One possibility is that obese females may present with more risk factors when compared with obese male AIS patients with a current or previous history of smoking. Therefore, the first objective of this study is to identify the risk factors in obese male and female AIS patients with a current or previous history of smoking.
Since obese males and females with a history of smoking may not present with similar risk factors in the general AIS population, our second objective is to determine specific risk factors contributing to sex differences in obese AIS patients with a history of smoking. Understanding these sex-related risk factors can facilitate the development of targeted support and personalized care to manage risk factors in obese AIS patients with a current or previous history of smoking.
Methods
Study population
This retrospective study utilized data obtained from the Prisma Health Acute Ischemic Stroke (AIS) cohort. The study protocol was reviewed and approved by the institutional review board of the PRISMA Health Institutional Committee for Ethics. Brain imaging (MRI, MRA, CT, CTA, etc.) was used to validate cases of ischemic stroke and to exclude cases with intracerebral or subarachnoid hemorrhagic stroke. We used data for patients classified as obese based on the BMI guidelines established by the World Health Organization (WHO) with individuals with a BMI of (> 30) being classified as obese and individuals with a BMI (< 30) falling into the categories of underweight, normal weight, or overweight [35]. Patients were classified as smokers based on whether the history of smoking was current, i.e. immediately before stroke or previous history before stroke. Therefore, smokers in this study are those with a current or previous history of smoking before admission for treatment of ischemic stroke. Data on clinical variables, demographic factors, and comorbidities were obtained from the registry.
Demographic factors including gender, age, ethnicity, and race were considered in this study. Additionally, past medical history of the patient population was also obtained covering conditions such as atrial fibrillation, coronary artery disease (CAD), carotid stenosis, depression, diabetes, a history of substance abuse, hypertension, migraine, heart failure (HF), hormone replacement therapy (HRT), dyslipidemia, family history of stroke, obesity, prior stroke, prior TIA, prosthetic heart valve, peripheral vascular disease (PVD), chronic renal disease, sickle cell, and sleep apnea. Ambulatory data from the patients were also collected with scores ranging from 0 to 3 0 denoting undocumented ambulation ability, 1 indicating an inability to ambulate, 2 denoting ability to ambulate with assistance, and 3 denoting the ability to ambulate independently. These scores were assigned to patients before, during, and after discharge. Any improvement was documented and defined as an increase in ambulatory status from patient admission to discharge.
Statistical analysis
Statistical Analyses were performed using Statistical Package for Social Sciences version 29.0 for Mac (SPSS, Chicago, IL). The normality of data distribution was assessed using the Kolmogorov-Smirnov test. Continuous variables with normal distribution were presented as mean ± SD, and comparisons between male and female patients were determined using the student-t-test. Non-normally distributed variables were analyzed using the Mann‐Whitney U test. Categorical variables were described using frequencies, and group differences were assessed using the χ2 test or Student T-Test. Patients were categorized into three groups (smokers, obesity, and smokers and obese), and univariate analysis was used to determine sex differences in risk factors for each group. The power analysis was computed using PASS 2023, version 23.0.2. For 2807 females, the power was 91.23% and d = 0.24, while 2662 males produced a power of 90% and d = 0.20.
The primary analysis in our study was sex-associated risk factors in male and female patients as outcome, performed using logistic regression models (with medical history, and laboratory values. as predictors in all models). Models were developed for each of the 4 AIS groups including,1) the whole AIS population, 2) smoking, 3) obesity, and 4) smoking combined with obesity stroke population. Our logistic regression models identified risk factors associated with male or female AIS patients within each of the stroke groups, including variables such as smoking, obesity, and the combined effects of obesity with a current or previous history of smoking. We assessed multicollinearity using Hosmer-Lemeshow tests while determining the sensitivity and specificity of the models through overall classified percentage and the area under the receiver operating curve (AUROC). Odds Ratios (ORs) for gender-specific risk factors in male and females were determined at 95% confidence intervals (CIs). The significance level for all tests was set at P < 0.05.
Results
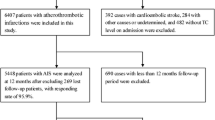
A total of 5,469 individuals diagnosed with ischemic stroke, were identified. Of this, 2,662 were males and 2,807 were females (Table 1). Male patients were more likely to present with a history of coronary artery disease, carotid artery stenosis, alcohol use, sleep apnea, and tobacco use (P < 0.001). Conversely, females presented with a higher likelihood of presenting with atrial fibrillation, depression, heart failure, hypertension, and migraines (P < 0.05). Males were more likely to be treated with cholesterol reducers (P < 0.05 while females were more likely to be treated with antihypertensive medications and antidepressants (P < 0.05). Females were likely to be older, and present with higher BMI compared with males (P < 0.05). Males were likely to present with higher levels of serum creatinine (P < 0.05), while females were likely to present with higher total cholesterol, HDL, and LDL (P < 0.05). Vital signs including higher diastolic blood pressure were more likely to be associated with males(P < 0.05). Females presented with a higher incidence of heart rate (P < 0.05) while males presented with improved ambulation (P < 0.05) when compared with females.
Table 2 presents the risk factors of AIS patients stratified by sex and obesity with current or previous history of smoking, obesity, and smoking alone. Obese AIS with a history of smoking that are males were more likely to present with coronary artery disease and alcohol use (P < 0.05). However, females were more likely to present with depression and migraines and were more likely to be treated with diabetic medications and antidepressants (P < 0.05). Males were more likely to present with higher serum creatinine levels (P < 0.05), while females were more likely to present with higher total cholesterol, and HDL levels (P < 0.05). Systolic and diastolic blood pressure were higher in males (P < 0.05 )when compared with females in the obese AIS patients with a history of smoking.
Obese male AIS patients with a history of smoking were more likely to present with coronary artery disease and alcohol use P < 0.05). On the other hand, females were more likely to present with depression, diabetes, migraine, and previous TIA (P < 0.05).
In addition, females were more likely to take hypertensive medications, diabetic medications, and antidepressants, presenting with a higher total cholesterol level and HDL (P < 0.05). Males were more likely to present with a higher serum creatinine level, INR, systolic, and diastolic blood pressure and were more likely to present with improved ambulation (P < 0.05) when compared with females.
Obese female AIS patients were more likely to be older and presented with higher BMI when compared with males (P < 0.05). Males were more likely to present with CAD, and a history of alcohol and tobacco use (P < 0.05) while females were more likely to present with higher levels of depression, heart failure, and migraine (P < 0.05). Females were more likely to present with higher total cholesterol, HDL, and LDL (P < 0.05). Males were more likely to present with higher serum creatinine (P < 0.05) while females were more likely to be taking hypertensive medications and antidepressants (P < 0.05).
Figure 1 presents the results of the adjusted analysis for the entire AIS population. BMI (OR = 0.977, 95% CI, 0.966–0.988, P = < 0.001), atrial fibrillation (OR = 0.759, 95% CI, 0.610–0.945, P = 0.014), depression (OR = 0.473, 95% CI, 0.346–0.553, P = 0.014), heart failure (OR = 0.607, 95% CI, 0.465–0.792, P < 0.001), hypertension (OR = 0.745, 95% CI, 0.616–0.900, P = 0.002), migraine (OR = 0.320, 95% CI, 0.191–0.535, P < 0.001), total cholesterol (OR = 0.996, 95% CI, 0.994–0.998, P < 0.001), HDL (OR = 0.960, 95% CI, 0.953–0.966, P < 0.001), heart rate (OR = 0.984, 95% CI, 0.979–0.988, P < 0.001), and NIHSS > 7 (OR = 0.709, 95% CI, 0.602–0.835, P < 0.001) were all significantly associated with females. Coronary artery disease (OR = 1.675, 95% CI, 1.407–1.994, P < 0.001), alcohol use (OR = 3.960, 95% CI, 2.664–5.887, P < 0.001), smoking (OR = 1.442, 95% CI, 1.206–1.724, P < 0.001), serum creatinine (OR = 1.269, 95% CI, 1.146–1.405, P < 0.001), diastolic blood pressure (OR = 1.025, 95% CI, 1.021–1.030, P < 0.001), TPA administration (OR = 1.196, 95% CI, 1.007–1.421, P = 0.041), ambulation improvement (OR = 1.185, 95% CI, 1.010–1.391, P = 0.037), and sleep apnea (OR = 2.825, 95% CI, 1.810–4.409, P < 0.001) were all associated with the males. Our model indicates a strong discriminative capability (Area Under the Curve (AUC) = 0.758, 95% CI, 0.742–0.775, P < 0.001).

Risk factors associated with male and female AIS patients for the entire AIS population include smoking + obesity, smoking, and obesity. Odd ratios (OD) below 1 denote factors associated with female while above 1 denotes factors associated with male patients. *Indicates statistical significance (P < 0.05) with a 95% confidence interval
Figure 2 presents risk factors for obese AIS population with a history of smoking. Coronary artery disease (OR = 1.806, 95% CI, 1.028–3.174, P = 0.040), a history of alcohol use (OR = 2.873, 95% CI, 1.349–6.166, P = 0.006), serum creatinine (OR = 4.724, 95% CI, 2.171–10.281, P < 0.001), age (OR = 1.024, 95% CI, 1.022–1.047, P = 0.033), and systolic blood pressure (OR = 1.029, 95% CI, 1.011–1.047, P < 0.002) were significantly associated with males. Depression (OR = 0.432, 95% CI, 0.244–0.764, P = 0.004), previous TIA (OR = 0.319, 95% CI, 0.142–0.714, P < 0.005), and higher levels of HDL (OR = 0.938, 95% CI, 0.915–0.962, P < 0.001) were associated with females. The discriminative capability of the model was strong (AUC = 0.769, 95% CI, 0.729–0.809, P < 0.001).

Risk factors associated with obese AIS population with a history of smoking. Odd ratios (OD) below 1 denotes factors associated with female while above 1 denotes factors associated with male patients. *Indicates statistical significance (P < 0.05) with a 95% confidence interval
Figure 3 presents risk factors for AIS patients with a history of smoking only. Coronary artery disease (OR = 2.033, 95% CI, 1.385–2.984, P < 0.001), a history of alcohol (OR = 1.906, 95% CI, 1.207–3.007, P = 0.006), serum creatinine (OR = 5.325, 95% CI, 3.225–8.711, P < 0.001), and diastolic blood pressure (OR = 1.022, 95% CI, 1.013–1.031, P < 0.001) were associated with males. Depression (OR = 0.391, 95% CI, 0.251–0.610, P < 0.001), previous TIA (OR = 0.0.438, 95% CI, 0.256–0.749, P = 0.003), diabetic medication (OR = 0.591, 95% CI, 0.396–0.882, P = 0.010), total cholesterol (OR = 0.995, 95% CI, 0.991–0.998, P = 0.002), HDL (OR = 0.978, 95% CI, 0.967–0.989, P = 0.002), and heart rate (OR = 0.990, 95% CI, 0.980–0.999, P = 0.025) were associated with females. The discriminative capability of the model was strong (AUC = 0.754, 95% CI, 0.727–0.781, P < 0.001).

Risk factors associated with AIS patients with a history of smoking only. Odd ratios (OD) below 1 denotes factors associated with female while above 1 denotes factors associated with male patients. *Indicates statistical significance (P < 0.05) with a 95% confidence interval
Figure 4 presents the risk factors of obese AIS patients. Coronary artery disease (OR = 1.720, 95% CI, 1.335–2.216, P < 0.001), a history of alcohol (OR = 4.726, 95% CI, 2.701–8.268, P < 0.001), LDL (OR = 1.009, 95% CI, 1.001–1.017, P = 0.030), and diastolic blood pressure (OR = 1.022, 95% CI, 1.015–1.028, P < 0.001) were associated with males. Age (OR = 0.985, 95% CI, 0.976–0.993, P < 0.001), BMI (OR = 0.929, 95% CI, 0.910–0.948, P < 0.001), depression (OR = 0.495, 95% CI, 0.376–0.653, P < 0.001) heart failure (OR = 0.606, 95% CI, 0.417–0.881, P = 0.009), migraine (OR = 0.339, 95% CI, 0.188–0.612, P < 0.001), total cholesterol (OR = 0.989, 95% CI, 0.983–0.996, P = 0.003), HDL (OR = 0.950, 95% CI, 0.940–0.961, P < 0.001), and heart rate (OR = 0.981, 95% CI, 0.974–0.987, P < 0.001) were associated with females. The model has a strong discriminative capability (AUC = 0.768, 95% CI, 0.747–0.788 P < 0.001).

Risk factors associated with obese AIS patients only. Odd ratios (OD) below 1 denotes factors associated with female while above 1 denotes factors associated with male patients. *Indicates statistical significance (P < 0.05) with a 95% confidence interval
In general, we observed differences and similarities (Table 3). In terms of similarities, for men, coronary artery disease and alcohol use were observed in obese AIS patients with a history of smoking. In contrast, an increase in serum creatine was only observed in obese AIS patients with a history of smoking. Moreover, an increase in diastolic blood pressure was observed among AIS patients with a history of smoking or obesity. In terms of differences, an increase in age was only observed in obese AIS patients with a history of smoking. In contrast, an elevated LDL was only observed in obese male AIS patients that present. In contrast, an increase in systolic blood pressure was only observed in obese AIS patients with a history of smoking. For females, depression was observed in obese AIS patients with a history of smoking. In addition, a previous history of TIA was observed in obese AIS patients with a history of smoking. Elevated HDL was observed in obese AIS patients with a history of smoking. An increase in heart rate and total cholesterol was observed among obese AIS patients with or without a history of smoking. In terms of differences, the use of diabetic medication was only observed in AIS patients with a history of smoking. In contrast, BMI, heart failure, and migraine were observed among obese female AIS patients.
Discussion
This study produced several results. First, in obese AIS patients with a history of smoking, that present with coronary artery disease, a history of alcohol use, higher serum creatinine and systolic blood pressure were more likely to be males. In contrast, depression, previous TIA, and higher levels of HDL were associated with females.
Second, among AIS patients that are current or previous smokers, but not obese, coronary artery disease, alcohol use, elevated serum creatinine, and diastolic blood pressure were associated with males, while depression, previous TIA, use of diabetic medication, elevated total cholesterol, and heart rate were associated with females.
Third, in obese AIS patients without a history of smoking, coronary artery disease, alcohol use, LDL, and diastolic blood pressure were associated with males, while older patients with higher BMI and a history of depression, heart failure, migraine, and elevated total cholesterol. HDL and heart rate were more likely to be females.
Our results for obese male AIS patients with a history of smoking have been reported by other studies for stroke patients with CAD [36, 37], alcohol use [38], serum creatinine [39], age [40], and systolic blood pressure [41]. Coronary artery disease (CAD) is indeed more prevalent in males than in females [42], and this has been attributed to several factors, including the protective effects of sex hormones such as estrogen in females [43]. Estrogen is known to have antioxidative and anti-inflammatory properties that can slow down the progression of atherosclerotic plaque, a key factor in the development of CAD [44]. This is significant because atherosclerosis is a key underlying process in the development of CAD. Estrogen’s influence on plasma lipids and lipoproteins is also beneficial, as it can lead to a more favorable lipid profile, further reducing the risk of atherosclerosis [45]. This protective effect may contribute to reducing the incidence of CAD in female obese AIS with a history of smoking compared with males.
We observed that obese male AIS patients that present with a history of smoking were more likely to be associated with a history of alcohol use. Males are more likely to use alcohol as a coping mechanism for stress, which can lead to higher rates of alcohol use and related problems [46]. Societal norms and expectations can influence drinking behaviors. For example, heavy drinking may be more socially acceptable for males, leading to higher rates of alcohol use and related problems. Therefore, compared with males, more females are lifetime abstainers, drink less, and are less likely to develop alcohol-related disorders [47], although females who drink in excess develop more clinical issues [48]. Moreover, males are more likely to be treated in emergency departments for alcohol use problems [49]. These findings support our current result in alcohol use being associated with obese male AIS patients with a history of smoking. In addition, different factors, including alcohol pharmacokinetics as well as its effect on nervous system functioning and the level of sex hormones, may interact with alcohol use in a complex manner [50], and contribute to the observed difference in male and female patients. It is important to point out that while these trends can be observed at the population level, individual experiences with alcohol use and its related problems can vary widely. Future studies on mechanisms underlying the biology and psycho-sociocultural differences in alcohol use, obesity, and smoking will help in the development of appropriate care for male and female obese AIS patients with a history of smoking.
Elevated serum creatine level was linked with obese male AIS patients with a history of smoking. An association between increased risk of cerebrovascular disease and elevated serum creatine levels has been reported [51, 52]. These studies focused on specific groups, such as patients with stroke [53], and myocardial infarction [53], in all of whom cerebrovascular and coronary heart disease are the primary causes of mortality. The authors suggested that an increased level of creatinine has a major impact on vascular diseases [54], implying that serum creatinine predicts survival in patients with stroke [55]. In our current study, elevated serum creatine was associated with AIS males who are obese and present with a history of smoking. This result indicates the relationship between serum creatinine and stroke events in AIS male patients who are obese and present with a history of smoking. Our finding indicates that an elevated serum creatinine concentration may represent a marker for subtle renal damage and may constitute an additional risk factor for the combined effect of obesity and smoking on male stroke patients. Therefore, monitoring serum creatinine concentration is crucial, especially for male stroke patients with a history of smoking and obesity.
Elevated systolic blood pressure was linked with male AIS patients who present with a history of smoking, while diastolic blood pressure was linked with obese AIS patients with or without a history of smoking, but not in patients who presented with the combined effect of obesity and smoking. Hypertension guidelines include both systolic and diastolic blood pressure (DBP) targets [56, 57]. It has been shown that although systolic blood pressure (SBP) had a greater effect, systolic and diastolic blood pressures each independently affect stroke outcomes [58]. Accordingly, elevated levels of SBP and DBP were associated with an increased risk of ischemic stroke in both sexes [59]. In general, the link between BP and severity of stroke is controversial [60, 61]. While some studies show that neither SBP nor DBP projected stroke severity [62], others suggest that only SBP [63] or DBP [64] were associated with worse neurologic outcomes. Our current study indicates that higher SBP was associated with male, obese AIS patients and present with a history of smoking, while DBP was associated with obese AIS patients with or without a history of smoking. Therefore, future studies may help determine the relationship between SBP, DBP, and obese AIS patients with a history of smoking.
We observed that LDL was only linked with obese male AIS patients, and not with AIS patients with the combined effect of smoking and obesity or smoking alone. Stroke is a multifactorial disease and is associated with several risk factors including atherosclerosis of the cerebral circulation, linked with the abnormalities of serum lipids and lipoproteins [65, 66]. Such aberrations include an increase in triglyceride levels, downregulation of high-density lipoproteins (HDL) cholesterol concentrations, and elevated low-density lipoproteins (LDL) levels [67]. In particular, LDL consists of many distinct subcomponents including LDL-1 to LDL-7 LDL, of which LDL-3 and LDL-4 are known risk factors for AIS [68]. Our finding that LDL was associated with male obese AIS patients underscores the importance of LDL and its sub-components in the assessment and management of these patients. Therefore, monitoring and managing these lipid levels is crucial in the prevention and treatment of stroke, particularly in male obese AIS patients.
An important finding in this study is that among patients with AIS, those who are obese and present with a history of smoking, either individually or in combination are more likely to experience depression. Depression is known to elevate morbidity in ischemic stroke patients [69]. Regardless of age, females exhibit higher rates of depression than males [70]. Females are more likely to be treated with depression even during stroke when compared with males [71]. Furthermore, females tend to experience poorer functional outcomes after ischemic stroke [72]. Therefore, given the higher rates of depression and worse outcomes after stroke in females, it is not surprising that female AIS patients who are obese and present with a history of smoking or obesity were associated with depression in our current study. This finding underscores the need for targeted interventions to manage depression, especially in female stroke patients and those with risk factors like obesity and smoking.
We observed that female obese AIS patients that present with or without a history of smoking were more likely to be associated with a baseline previous TIA. A previous history of TIA is a major predictor of subsequent ischemic stroke [73]. In general, the incidence of TIA varies and is stratified by age distribution. For example, among males between the ages of 65 to 69, TIA is lower (< 2.6%) when compared with those between 75 and 79 years of age(> 3.5%) [74]. For females that are between 65 and 69 years of age, the prevalence of TIA is 1.6%, while females between 75 and 79 years of age presented with a higher proportion (> 4.0%) [75]. In general, a higher prevalence of TIA is reported in females when compared with males [75] and this supports our current results in female AIS patients with a combined effect of obesity and smoking, and smoking alone. Future studies that focus on the management of TIA and related risk factors by sex are necessary to reduce TIA incidence in male and female patients.
We observed an association between elevated total cholesterol (TC) and female AIS patients with a history of smoking while higher levels of HDL were associated with obese AIS patients with a history of smoking. TC has been identified as an independent predictor of poor outcomes in patients with AIS as documented by several studies [76,77,78]. Furthermore, there is a significant association between sex and serum levels of TC, LDL-C, and HDL-C in stroke patients [79, 80]. Findings indicate that females with AIS present with higher serum levels of all three subclasses, including TC and HDL, compared to males [81], suggesting a sex-dependent relationship between TC and HDL serum levels. Moreover, females with higher TC present with an increased risk for AIS compared to females whose cholesterol is lower [82]. The current study indicates a higher level of HDL-cholesterol and LDL-cholesterol in obese female AIS patients with baseline history of smoking. This result highlights the complex interplay between cholesterol levels, obesity, smoking history, and sex in the context of AIS.
An increase in heart rate was associated with female AIS patients with a history of smoking or obesity, while an increase in heart failure (HF) was associated with obese female AIS patients. An increase in heart rate is a biological variable that can predict heart failure and cardiovascular diseases [83]. This suggests a link between increased heart rate and HF, which can be extended to vascular diseases, including stroke [84]. Heart failure manifests differently in males and females, and females are at a higher risk than males [85]. While ischemia is the primary cause in males, hypertension and diabetes contribute more to HF in females [85]. Our current finding indicates that an increase in HF was associated with female AIS patients with a history of smoking, or obesity. Further investigation into the pathophysiology and management approaches for individuals with a history of ischemic stroke considering males and females and taking into account their history of smoking, obesity, and baseline elevation in heart rate and heart failure will represent an advancement towards precision medicine and improvement of clinical research.
We observed that female AIS patients, that present with a history of smoking were more likely to be treated with diabetic medication. Diabetes significantly increases the risk of ischemic stroke, and this risk is higher in females compared to males [86]. Uncontrolled diabetes can lead to hyperglycemia, which can result in various outcomes, including mild, moderate, or severe intracerebral hemorrhage [87]. Notably, diabetes shows a stronger association with ischemic stroke in females compared with males [88], and the risk starts at lower fasting blood glucose levels for females [89]. AIS patients with diabetes that receive continuous diabetic medications both before stroke onset and after admission have improved functional outcomes [90]. This finding supports our current result highlighting the use of diabetes medication among female AIS, especially considering the stronger association between incident ischemic stroke in females compared with males [88].
There was an association between higher BMI and female AIS patients. Higher BMI or obesity is linked to a higher risk of ischemic stroke [91]. This positive association between higher BMI and ischemic stroke incidence has been reported in both males and females [92]. Although higher BMI is linked to a higher risk of ischemic stroke in both sexes, the association is notably stronger in females when compared to males [92]. This finding strengthens our current result indicating that female AIS patients are more likely to have a higher BMI.
In our study, we found that female AIS patients with a history of obesity were more likely to be associated with migraine. A similar trend has been reported for stroke patients [93]. Migraine is associated with an increased risk of ischemic stroke among males and females, but females are particularly more affected by migraine, especially considering that the condition is predominantly diagnosed in females [94]. The sex-related differences in migraine also carry clinical significance, as the incidence, duration, and disability associated with migraine tend to be higher in females [95]. Taken together, existing studies support our current result regarding the association of obese female AIS patients with baseline migraine.
An important finding in this study is that older male AIS patients were associated with male and female AIS patients with a combined effect of obesity and smoking, while older female AIS patients were more likely to be associated with patients with a current or previous history of smoking. Aging is a major risk factor for stroke and the risk increases every 10 years after age 55 years [96]. More than half of ischemic strokes occur in individuals who are ≥ 65 years old, and stroke-related mortality increases with age [96]. The death rates from stroke are expected to increase in people aged ≥ 65 years in the next 10 years [97]. Moreover, the general lifetime risk for stroke in males is proposed to be 1 in 6 and 1 in 5 for females [98], with males presenting with greater rates at young age and females at older ages. In our current study, the proportion of AIS with a history of smoking or obesity who are older (e.g. ≥80) is small compared with younger age groups, indicating that age, when combined with two or more chronic conditions such as obesity and smoking, are important risk factors in male and female stroke patients. Therefore, smoking and obesity either alone or combined, may potentially interact with conventional cardiovascular risk factor(s) to increase the risk, severity, and outcome in male and female AIS patients.
Limitations
This study has many notable limitations. Data for smoking was obtained from self-report. While there is evidence supporting the validity of self-reported smoking [99], there is a tendency of bias because of under- or overreporting of smoking behaviors. Additionally, factors such as quantity, duration, and continuation of smoking habits were not included and could potentially have an impact on the results. Another limitation is that all patient data on clinical characteristics, risk factors, comorbidities, etc. were collected from a single institution and the results of this study cannot be generalized to other institutions. Moreover, our data is cross-sectional thus, limiting causal inferences. The retrospective nature of our study did not separate current and previous smokers in the database of the stroke registry, making it difficult to identify those who are current or previous smokers. This study has notable strengths. A major strength is the ability to determine risk factors that are associated with the combined effect of obesity with a current or previous history of smoking in male and female AIS patients. Our findings have implications for the future development of precise medicine for the care of male and female AIS patients with the combined effect of obesity with a current or previous history of smoking.
Conclusion
Despite significant advancements in research focusing on sex differences in comorbidities associated with stroke, as well as the identification of specific risk factors influencing treatment outcomes in both female and male AIS patients, there are still notable gaps in research. Existing data on stroke often fail to distinguish between sex and gender integrating both influences without recognizing that sex and gender are not binary concepts. Experimental designs and data collection do not differentiate between sex and gender identity. Consequently, many findings on sex differences reflect a combined effect of both sex and gender [100] supporting the observed differences between male and female AIS patients in our current study. Our findings showed differences and similarities in risk factors for male and female patients. Precisely, we identified specific risk factors unique to male and female patients that when managed could enhance the care of AIS patients with a combined effect of obesity with a current or previous history of smoking. These findings highlight the need for the development of management strategies targeting AIS patients with a combined effect of obesity and smoking or smoking.
Data availability
Materials are available on request from the corresponding author.
Abbreviations
- AIS:
-
Acute ischemic stroke
- BMI:
-
Body mass index
- AUROC:
-
Area under the receiver operating curve
- aPTT:
-
Active partial thromboplastin time
- BBB:
-
Blood-brain barrier
- CVD:
-
Cardiovascular disease
- CAD:
-
Coronary artery disease
- CAS:
-
Carotid artery disease
- CRD:
-
Chronic renal disease
- CT:
-
Computer tomography
- INR:
-
International normalized ratio
- MRI:
-
Magnetic resonance image
- TIA:
-
Trans ischemic attack
- rtPA:
-
Recombinant tissue plasminogen activator
- OD:
-
Odd ratio
- HDL-C:
-
High-density lipoprotein
- LDL-C:
-
Low-density lipoprotein
- TC:
-
Total cholesterol
- TGs:
-
Total triglycerides
- NIHSS:
-
National Institute of Health stroke scale
- PVD:
-
Peripheral vascular disease
- rtPA:
-
Recombinant tissue plasminogen activator
- ROC:
-
Receiver Operating Curve
- sICH:
-
Symptomatic intracerebral hemorrhage
- SD:
-
Standard deviation
- TC:
-
Total cholesterol
References
Husky MM, Mazure CM, Paliwal P, McKee SA. Gender differences in the comorbidity of smoking behavior and major depression. Drug Alcohol Depend. 2008;93(1–2):176–9. https://doi.org/10.1016/j.drugalcdep.2007.07.015.
Awujoola A, Sodeke P, Olufeyisayo O, Mokikan M, Adeyemi E, Babalola G, et al. Clinical risk factors associated with ambulatory outcome in acute ischemic stroke patient smokers treated with thrombolytic therapy. Am J Med Sci. 2021;362(4):363–74.
Horn JW, Feng T, Mørkedal B, Strand LB, Horn J, Mukamal K, et al. Obesity and risk for first ischemic stroke depends on metabolic syndrome: the HUNT study. Stroke. 2021;52(11):3555–61. https://doi.org/10.1161/strokeaha.120.033016.
Wang Q. Smoking and body weight: evidence from China health and nutrition survey. BMC Public Health. 2015;15(1):1238. https://doi.org/10.1186/s12889-015-2549-9.
Kim Y, Jeong SM, Yoo B, Oh B, Kang HC. Associations of smoking with overall obesity, and central obesity: a cross-sectional study from the Korea National Health and Nutrition Examination Survey (2010–2013). Epidemiol Health. 2016;38:e2016020. https://doi.org/10.4178/epih.e2016020.
Musazadeh V, Zarezadeh M, Ghalichi F, Ahrabi SS, Jamilian P, Jamilian P, et al. Anti-obesity properties of probiotics; a considerable medical nutrition intervention: findings from an umbrella meta-analysis. Eur J Pharmacol. 2022;928:175069. https://doi.org/10.1016/j.ejphar.2022.175069.
Quiñones-Ossa GA, Lobo C, Garcia-Ballestas E, Florez WA, Moscote-Salazar LR, Agrawal A. Obesity and stroke: does the Paradox apply for stroke? Neurointervention. 2021;16(1):9–19; https://doi.org/10.5469/neuroint.2020.00108.
Blum B, Penwell A, Wormack L, Walker B, Lari S, Nathaniel TI. Gender and thrombolysis therapy in acute ischemic stroke patients with incidence of obesity. Neurol Sci. 2019;40(9):1829–39. https://doi.org/10.1007/s10072-019-03902-7.
Freedman DM, Sigurdson AJ, Rajaraman P, Doody MM, Linet MS, Ron E. The mortality risk of smoking and obesity combined. Am J Prev Med. 2006;31(5):355–62. https://doi.org/10.1016/j.amepre.2006.07.022.
Brown C, Terrell K, Goodwin R, Nathaniel T. Stroke severity in ischemic stroke patients with a history of diastolic blood pressure treated in a Telestroke Network. J Cardiovasc Dev Dis. 2022;9:10. https://doi.org/10.3390/jcdd9100345.
Brechtel L, Poupore N, Stoikov T, Roley LT, Emerson JF, Nathaniel T. Comorbidities associated with different levels of total cholesterol in male and female acute ischemic stroke patients. Medicine. 2020;99:52.
Ovbiagele B, Nguyen-Huynh MN. Stroke epidemiology: advancing our understanding of disease mechanism and therapy. Neurotherapeutics. 2011;8(3):319–29. https://doi.org/10.1007/s13311-011-0053-1.
Lawson TR, Brown IE, Westerkam DL, Blackhurst DW, Sternberg S, Leacock R, et al. Tissue plasminogen activator (rt-PA) in acute ischemic stroke: outcomes associated with ambulation. Restor Neurol Neurosci. 2015;33(3):301–8. https://doi.org/10.3233/rnn-140480.
Reeves MJ, Bushnell CD, Howard G, Gargano JW, Duncan PW, Lynch G, et al. Sex differences in stroke: epidemiology, clinical presentation, medical care, and outcomes. Lancet Neurol. 2008;7(10):915–26. https://doi.org/10.1016/s1474-4422(08)70193-5.
Nathaniel TI, Cochran T, Chaves J, Fulmer E, Sosa C, Yi S, et al. Co-morbid conditions in use of recombinant tissue plasminogen activator (rt-PA) for the treatment of acute ischaemic stroke. Brain Inj. 2016;30(10):1261–5. https://doi.org/10.1080/02699052.2016.1186840.
Synhaeve NE, Arntz RM, van Alebeek ME, van Pamelen J, Maaijwee NAM, Rutten-Jacobs LCA, et al. Women have a poorer very long-term functional outcome after stroke among adults aged 18–50 years: the FUTURE study. J Neurol. 2016;263(6):1099–105. https://doi.org/10.1007/s00415-016-8042-2.
Poupore N, Strat D, Mackey T, Brown K, Snell A, Nathaniel TI. Thrombolytic therapy in ischemic stroke patients with a preceding transient ischemic attack in telestroke and non-telestroke settings. Neurol Clin Neurosci. 2020;8(5):298–308.
Yoon CW, Bushnell CD. Stroke in women: a review focused on epidemiology, risk factors, and outcomes. J Stroke. 2023;25(1):2–15. https://doi.org/10.5853/jos.2022.03468.
Zarulli V, Barthold Jones JA, Oksuzyan A, Lindahl-Jacobsen R, Christensen K, Vaupel JW. Women live longer than men even during severe famines and epidemics. Proceedings of the National Academy of Sciences. 2018;115 4:E832-E40; doi: https://doi.org/10.1073/pnas.1701535115.
Simmons CA, Poupore N, Nathaniel TI. Age Stratification and Stroke Severity in the Telestroke Network. J Clin Med. 2023;12(4). https://doi.org/10.3390/jcm12041519.
Emdin C, Wong C, Hsiao A. Atrial fibrillation as risk factor for cardiovascular disease and death in women compared with men: systematic review and meta-analysis of cohort studies. BMJ. 2016;532:h7013.
Fredwall M, Sternberg S, Blackhurst D, Lee A, Leacock R, Nathaniel TI. Gender differences in Exclusion Criteria for recombinant tissue-type plasminogen activator. J Stroke Cerebrovasc Dis. 2016;25(11):2569–74. https://doi.org/10.1016/j.jstrokecerebrovasdis.2016.06.012.
Peters SA, Huxley RR, Woodward M. Diabetes as a risk factor for stroke in women compared with men: a systematic review and meta-analysis of 64 cohorts, including 775,385 individuals and 12,539 strokes. Lancet. 2014;383 9933:1973–80. https://doi.org/10.1016/s0140-6736(14)60040-4.
Colello MJ, Ivey LE, Gainey J, Faulkner RV, Johnson A, Brechtel L, et al. Pharmacological thrombolysis for acute ischemic stroke treatment: gender differences in clinical risk factors. Adv Med Sci. 2018;63(1):100–6. https://doi.org/10.1016/j.advms.2017.08.003.
Gainey J, Blum B, Bowie B, Cooley K, Madeline L, Ervin EL, et al. Stroke and dyslipidemia: clinical risk factors in the telestroke versus non-telestroke. Lipids Health Dis. 2018;17. https://doi.org/10.1186/s12944-018-0870-x.
Ng M, Freeman MK, Fleming TD, Robinson M, Dwyer-Lindgren L, Thomson B, et al. Smoking prevalence and cigarette consumption in 187 countries, 1980–2012. JAMA. 2014;311(2):183–92. https://doi.org/10.1001/jama.2013.284692.
Fleming T, Blum B, Averkamp B, Sullivan J, Nathaniel T. Effect of antihypertensive medications on thrombolysis therapy and outcomes in acute ischemic stroke patients. J Clin Hypertens. 2019;21(2):271–9. https://doi.org/10.1111/jch.13472.
Peters SA, Huxley RR, Woodward M. Smoking as a risk factor for stroke in women compared with men: a systematic review and meta-analysis of 81 cohorts, including 3,980,359 individuals and 42,401 strokes. Stroke. 2013;44(10):2821–8. https://doi.org/10.1161/strokeaha.113.002342.
Nathaniel TI, Gainey J, Blum B, Montgomery C, Ervin L, Madeline L. Clinical risk factors in thrombolysis therapy: Telestroke Versus Nontelestroke. J Stroke Cerebrovasc Dis. 2018;27(9):2524–33. https://doi.org/10.1016/j.jstrokecerebrovasdis.2018.05.012.
Garawi F, Devries K, Thorogood N, Uauy R. Global differences between women and men in the prevalence of obesity: is there an association with gender inequality? Eur J Clin Nutr. 2014;68(10):1101–6. https://doi.org/10.1038/ejcn.2014.86.
Polk S, Stafford C, Adkins A, Efird J, Colello M, Nathaniel IT. Contraindications with recombinant tissue plasminogen activator (rt-PA) in acute ischemic stroke population. Neurol Psychiatry Brain Res. 2018;27:6–11.
Peters SA, Huxley RR, Woodward M. Do smoking habits differ between women and men in contemporary western populations? Evidence from half a million people in the UK Biobank study. BMJ Open. 2014;4(12):e005663. https://doi.org/10.1136/bmjopen-2014-005663.
Rathfoot C, Edrissi C, Sanders CB, Knisely K, Poupore N, Nathaniel T. Gender differences in comorbidities and risk factors in ischemic stroke patients with a history of atrial fibrillation. BMC Neurol. 2021;21(1:209). https://doi.org/10.1186/s12883-021-02214-8.
Peters SAE, Carcel C, Millett ERC, Woodward M. Sex differences in the association between major risk factors and the risk of stroke in the UK Biobank cohort study. Neurology. 2020;95(20):e2715–26. https://doi.org/10.1212/wnl.0000000000010982.
LM êkê K, Samouda H, Jacobs J, di Pompeo C, Lemdani M, Hubert H, et al. Body mass index and childhood obesity classification systems: a comparison of the French, International Obesity Task Force (IOTF) and World Health Organization (WHO) references. Rev Epidemiol Sante Publique. 2015;63(3):173–82. https://doi.org/10.1016/j.respe.2014.11.003.
Duda-Pyszny D, Trzeciak P, Desperak P, Zembala M, Gąsior M. Comparison of clinical characteristics, in-hospital course, and 12-month prognosis in women and men with chronic coronary syndromes. Kardiologia Polska (Polish Heart Journal). 2021;79(4):393–400.
Kunadian V, Qiu W, Lagerqvist B, Johnston N, Sinclair H, Tan Y, et al. Gender differences in outcomes and predictors of all-cause mortality after percutaneous coronary intervention (data from United Kingdom and Sweden). Am J Cardiol. 2017;119(2):210–6.
Mukamal KJ, Ascherio A, Mittleman MA, Conigrave KM, Camargo CA Jr., Kawachi I, et al. Alcohol and risk for ischemic stroke in men: the role of drinking patterns and usual beverage. Ann Intern Med. 2005;142(1):11–9. https://doi.org/10.7326/0003-4819-142-1-200501040-00007.
Jones CA, McQuillan GM, Kusek JW, Eberhardt MS, Herman WH, Coresh J, et al. Serum creatinine levels in the US population: third National Health and Nutrition Examination Survey. Am J Kidney Dis. 1998;32(6):992–9. https://doi.org/10.1016/s0272-6386(98)70074-5.
Curb JD, Abbott RD, MacLean CJ, Rodriguez BL, Burchfiel CM, Sharp DS, et al. Age-related changes in stroke risk in men with hypertension and normal blood pressure. Stroke. 1996;27(5):819–24. https://doi.org/10.1161/01.str.27.5.819.
Scott H, Barton MJ, Johnston ANB. Isolated systolic hypertension in young males: a scoping review. Clin Hypertens. 2021;27(1:12). https://doi.org/10.1186/s40885-021-00169-z.
Jamee A, Abed Y, Jalambo MO. Gender difference and characteristics attributed to coronary artery disease in Gaza-Palestine. Glob J Health Sci. 2013;5(5):51–6. https://doi.org/10.5539/gjhs.v5n5p51.
Kundakovic M, Rocks D. Sex hormone fluctuation and increased female risk for depression and anxiety disorders: from clinical evidence to molecular mechanisms. Front Neuroendocrinol. 2022;66:101010. https://doi.org/10.1016/j.yfrne.2022.101010.
Xiang D, Liu Y, Zhou S, Zhou E, Wang Y. Protective effects of Estrogen on Cardiovascular Disease mediated by oxidative stress. Oxid Med Cell Longev. 2021;2021:5523516. https://doi.org/10.1155/2021/5523516.
Meng Q, Li Y, Ji T, Chao Y, Li J, Fu Y, et al. Estrogen prevent atherosclerosis by attenuating endothelial cell pyroptosis via activation of estrogen receptor α-mediated autophagy. J Adv Res. 2021;28:149–64. https://doi.org/10.1016/j.jare.2020.08.010.
White AM. Gender differences in the Epidemiology of Alcohol Use and Related Harms in the United States. Alcohol Res. 2020;40(2):01. https://doi.org/10.35946/arcr.v40.2.01.
Kezer CA, Simonetto DA, Shah VH. Sex Differences in Alcohol Consumption and Alcohol-Associated Liver Disease. Mayo Clin Proc. 2021;96(4):1006–16; https://doi.org/10.1016/j.mayocp.2020.08.020.
Sterling SA, Palzes VA, Lu Y, Kline-Simon AH, Parthasarathy S, Ross T, et al. Associations between medical conditions and alcohol consumption levels in an adult Primary Care Population. JAMA Netw Open. 2020;3 5:e204687–e. https://doi.org/10.1001/jamanetworkopen.2020.4687.
Control, CfD. Prevention. Surveillance report. Atlanta, Ga: US Dept of Health and Human Services, Centers for Disease Control and Prevention. 1999.
Erol A, Karpyak VM. Sex and gender-related differences in alcohol use and its consequences: contemporary knowledge and future research considerations. Drug Alcohol Depend. 2015;156:1–13. https://doi.org/10.1016/j.drugalcdep.2015.08.023.
Fried LF, Katz R, Sarnak MJ, Shlipak MG, Chaves PHM, Jenny NS, et al. Kidney function as a predictor of Noncardiovascular Mortality. J Am Soc Nephrol. 2005;16(12):3728–35. https://doi.org/10.1681/asn.2005040384.
Ibrahim B, Rayyis L, Almekhlafi M. Elevated serum Creatinine predicts higher mortality in stroke patients (P3.254). Neurology. 2017;88:16 Supplement:P3.254.
Walsh CR, O’Donnell CJ, Camargo CA, Giugliano RP, Lloyd-Jones DM. Elevated serum creatinine is associated with 1-year mortality after acute myocardial infarction. Am Heart J. 2002;144(6):1003–11. https://doi.org/10.1067/mhj.2002.125504.
Carter CE, Katz R, Kramer H, de Boer IH, Kestenbaum BR, Peralta CA, et al. Influence of urine creatinine concentrations on the relation of albumin-creatinine ratio with cardiovascular disease events: the multi-ethnic study of atherosclerosis (MESA). Am J Kidney Dis. 2013;62(4):722–9. https://doi.org/10.1053/j.ajkd.2013.05.010.
Liu S, Li M, Yang Y, Chen Y, Wang W, Zheng X. A novel risk model based on white blood cell-related biomarkers for acute kidney injury prediction in patients with ischemic stroke admitted to the intensive care unit. Front Med (Lausanne). 2022;9:1043396. https://doi.org/10.3389/fmed.2022.1043396.
Unger T, Borghi C, Charchar F, Khan NA, Poulter NR, Prabhakaran D, et al. 2020 International Society of Hypertension global hypertension practice guidelines. J Hypertens. 2020;38(6):982–1004. https://doi.org/10.1097/hjh.0000000000002453.
Musazadeh V, Kavyani Z, Naghshbandi B, Dehghan P, Vajdi M. The beneficial effects of omega-3 polyunsaturated fatty acids on controlling blood pressure: an umbrella meta-analysis. Front Nutr. 2022;9:985451. https://doi.org/10.3389/fnut.2022.985451.
Flint AC, Conell C, Ren X, Banki NM, Chan SL, Rao VA, et al. Effect of systolic and diastolic blood pressure on Cardiovascular outcomes. N Engl J Med. 2019;381(3):243–51. https://doi.org/10.1056/NEJMoa1803180.
Ramezankhani A, Parizadeh D, Azizi F, Hadaegh F. Sex differences in the association between diabetes and hypertension and the risk of stroke: cohort of the Tehran lipid and glucose study. Biology sex Differences. 2022;13(1:10). https://doi.org/10.1186/s13293-022-00421-7.
Saiz LC, Gorricho J, Garjon J, Celaya MC, Erviti J, Leache L. Blood pressure targets for the treatment of people with hypertension and cardiovascular disease. Cochrane Database Syst Reviews. 2022; 11.
Bowry R, Navalkele DD, Gonzales NR. Blood pressure management in stroke: five new things. Neurology: Clin Pract. 2014;4(5):419–26.
Sare GM, Ali M, Shuaib A, Bath PM. Relationship between hyperacute blood pressure and outcome after ischemic stroke: data from the VISTA collaboration. Stroke. 2009;40(6):2098–103.
Sprigg N, Gray LJ, Bath PM, Boysen G, De Deyn PP, Friis P, et al. Relationship between outcome and baseline blood pressure and other haemodynamic measures in acute ischaemic stroke: data from the TAIST trial. J Hypertens. 2006;24(7):1413–7.
Tziomalos K, Giampatzis V, Bouziana SD, Spanou M, Papadopoulou M, Kostaki S, et al. Elevated diastolic but not systolic blood pressure increases mortality risk in hypertensive but not normotensive patients with acute ischemic stroke. Am J Hypertens. 2015;28(6):765–71.
Boehme AK, Esenwa C, Elkind MS. Stroke risk factors, Genetics, and Prevention. Circ Res. 2017;120(3):472–95. https://doi.org/10.1161/circresaha.116.308398.
Musazadeh V, Karimi A, Malekahmadi M, Ahrabi SS, Dehghan P. Omega-3 polyunsaturated fatty acids in the treatment of non-alcoholic fatty liver disease: an umbrella systematic review and meta-analysis. Clin Exp Pharmacol Physiol. 2023;50(5):327–34. https://doi.org/10.1111/1440-1681.13750.
Shabana, Shahid SU, Sarwar S. The abnormal lipid profile in obesity and coronary heart disease (CHD) in Pakistani subjects. Lipids Health Dis. 2020;19(1):73. https://doi.org/10.1186/s12944-020-01248-0.
Duan R, Xue W, Wang K, Yin N, Hao H, Chu H, et al. Estimation of the LDL subclasses in ischemic stroke as a risk factor in a Chinese population. BMC Neurol. 2020;20(1):414. https://doi.org/10.1186/s12883-020-01989-6.
Nathaniel TI, Gainey J, Blum B, Montgomery C, Ervin L, Madeline L. Clinical risk factors in thrombolysis therapy: telestroke versus nontelestroke. J Stroke Cerebrovasc Dis. 2018;27(9):2524–33.
Albert PR. Why is depression more prevalent in women? J Psychiatry Neurosci. 2015;40(4):219–21. https://doi.org/10.1503/jpn.150205.
Dong L, Sánchez BN, Skolarus LE, Stulberg E, Morgenstern LB, Lisabeth LD. Sex difference in prevalence of depression after stroke. Neurology. 2020;94:19. https://doi.org/10.1212/wnl.0000000000009394.
Zuo B, Zhang X, Wen F-f, Zhao Y. The influence of stressful life events on depression among Chinese university students: multiple mediating roles of fatalism and core self-evaluations. J Affect Disord. 2020;260:84–90.
Lioutas V-A, Ivan CS, Himali JJ, Aparicio HJ, Leveille T, Romero JR, et al. Incidence of transient ischemic attack and Association with Long-Term risk of stroke. JAMA. 2021;325(4):373–81. https://doi.org/10.1001/jama.2020.25071.
Vyas MV, Silver FL, Austin PC, Yu AY, Pequeno P, Fang J, et al. Stroke incidence by sex across the lifespan. Stroke. 2021;52(2):447–51.
Wang W, Sun P, Han F, Qu C. Sex differences in risk factors for transient ischemic attack in a Chinese Population. Front Neurol. 2021;12:615399. https://doi.org/10.3389/fneur.2021.615399.
Wu F, Wang Q, Qiao Y, Yu Q, Wang F. A new marker of short-term mortality and poor outcome in patients with acute ischemic stroke: Mean platelet volume-to-lymphocyte ratio. Med (Baltim). 2022;101 (40):e30911. https://doi.org/10.1097/md.0000000000030911.
Poupore N, Strat D, Mackey T, Snell A, Nathaniel T. Ischemic stroke with a preceding Trans ischemic attack (TIA) less than 24 hours and thrombolytic therapy. BMC Neurol. 2020;20(1):197. https://doi.org/10.1186/s12883-020-01782-5.
Poupore N, Strat D, Mackey T, Nathaniel TI. The Association between an antecedent of transient ischemic attack prior to Onset of Stroke and Functional Ambulatory Outcome. Clin Appl Thromb Hemost. 2020;26:1076029620906867. https://doi.org/10.1177/1076029620906867.
Brechtel L, Poupore N, Stoikov T, Roley LT, Emerson JF, Nathaniel T. Comorbidities associated with different levels of total cholesterol in male and female acute ischemic stroke patients. Med (Baltim). 2020;99(5)2:e23870. https://doi.org/10.1097/md.0000000000023870.
Musazadeh V, Dehghan P, Khoshbaten M. Efficacy of omega-3-rich Camelina sativa on the metabolic and clinical markers in nonalcoholic fatty liver disease: a randomized, controlled trial. Eur J Gastroenterol Hepatol. 2022;34(5):537–45. https://doi.org/10.1097/meg.0000000000002297.
Tohidi M, Mohebi R, Cheraghi L, Hajsheikholeslami F, Aref S, Nouri S, et al. Lipid profile components and incident cerebrovascular events versus coronary heart disease; the result of 9 years follow-up in Tehran lipid and glucose study. Clin Biochem. 2013;46(9):716–21.
Kurth T, Rist PM, Ridker PM, Kotler G, Bubes V, Buring JE. Association of migraine with aura and other risk factors with incident cardiovascular disease in women. JAMA. 2020;323(22):2281–9.
Ceconi C, Guardigli G, Rizzo P, Francolini G, Ferrari R. The heart rate story. Eur Heart J Supplements. 2011;13 supplC:C4–13.
Nakai M, Iwanaga Y, Sumita Y, Wada S, Hiramatsu H, Iihara K, et al. Associations among cardiovascular and cerebrovascular diseases: analysis of the nationwide claims-based JROAD-DPC dataset. PLoS ONE. 2022;17(3):e0264390. https://doi.org/10.1371/journal.pone.0264390.
Regitz-Zagrosek V. Sex and gender differences in Heart failure. Int J Heart Fail. 2020;2(3):157–81. https://doi.org/10.36628/ijhf.2020.0004.
Tun NN, Arunagirinathan G, Munshi SK, Pappachan JM. Diabetes mellitus and stroke: a clinical update. World J Diabetes. 2017;8(6):235.
Saxena A, Anderson CS, Wang X, Sato S, Arima H, Chan E, et al. Prognostic significance of hyperglycemia in Acute Intracerebral Hemorrhage: the INTERACT2 study. Stroke. 2016;47(3):682–8. https://doi.org/10.1161/strokeaha.115.011627.
Peters SA, Carcel C, Millett ER, Woodward M. Sex differences in the association between major risk factors and the risk of stroke in the UK Biobank cohort study. Neurology. 2020;95(20):e2715–26.
Madsen TE, Long DL, Carson AP, Howard G, Kleindorfer DO, Furie KL, et al. Sex and race differences in the risk of ischemic stroke associated with fasting blood glucose in REGARDS. Neurology. 2021;97 7:e684–94.
Jian Y, Wang H, Zhao L, Li T, Zhang L, Wang X, et al. Metformin treatment and acute ischemic stroke outcomes in patients with type 2 diabetes: a retrospective cohort study. Neurol Sci. 2023;44(3):989–97. https://doi.org/10.1007/s10072-022-06491-0.
Qi W, Ma J, Guan T, Zhao D, Abu-Hanna A, Schut M, et al. Risk factors for incident stroke and its subtypes in China: a prospective study. J Am Heart Association. 2020;9(21):e016352.
Shiozawa M, Kaneko H, Itoh H, Morita K, Okada A, Matsuoka S, et al. Association of Body Mass Index with ischemic and Hemorrhagic Stroke. Nutrients. 2021;13:7. https://doi.org/10.3390/nu13072343.
Sinclair AJ, Matharu M. Migraine, cerebrovascular disease and the metabolic syndrome. Ann Indian Acad Neurol. 2012;15(Suppl 1):S72–7. https://doi.org/10.4103/0972-2327.100015.
Amiri P, Kazeminasab S, Nejadghaderi SA, Mohammadinasab R, Pourfathi H, Araj-Khodaei M, et al. Migraine: a review on its history, Global Epidemiology, risk factors, and comorbidities. Front Neurol. 2021;12:800605. https://doi.org/10.3389/fneur.2021.800605.
Allais G, Chiarle G, Sinigaglia S, Airola G, Schiapparelli P, Benedetto C. Gender-related differences in migraine. Neurol Sci. 2020. https://doi.org/10.1007/s10072-020-04643-8. 41 Suppl 2:429 – 36; doi:.
Yousufuddin M, Young N. Aging and ischemic stroke. Aging. 2019;11(9):2542–4. https://doi.org/10.18632/aging.101931.
Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, et al. Heart disease and stroke statistics—2018 update: a report from the American Heart Association. Circulation. 2018;137(12):e67–492.
Leritz EC, McGlinchey RE, Kellison I, Rudolph JL, Milberg WP. Cardiovascular disease risk factors and cognition in the elderly. Curr Cardiovasc risk Rep. 2011;5:407–12.
Valladolid-López Mdel C, Barrientos-Gutiérrez T, Reynales-Shigematsu LM, Thrasher JF, Peláez-Ballestas I, Lazcano-Ponce E, et al. Evaluating the validity of self-reported smoking in Mexican adolescents. BMJ Open. 2015;5(10):e007485. https://doi.org/10.1136/bmjopen-2014-007485.
Norris CM, Johnson NL, Hardwicke-Brown E, McEwan M, Pelletier R, Pilote L. The contribution of gender to apparent sex differences in health status among patients with coronary artery disease. J Women’s Health. 2017;26(1):50–7.
Acknowledgements
We thank the stroke unit of Greenville Health System for helping with data collection.
Funding
This research was funded by the NIH R25 Grant. The NIH played no role in the study design, data collection, analysis, and interpretation of the results. The NIH did not influence the writing of the manuscript.
Author information
Authors and Affiliations
Contributions
DTO, PCB, PXB, AIN, SIN and TIN, designed the concept, experimental design, and data analysis. PCB and PXB participated in writing the manuscript, data collection, and editing the manuscript. All co-authors provided critical reviews on different drafts of the manuscript. All authors read and approved the final manuscript for publication.
Corresponding author
Ethics declarations
Ethics approval
This is a retrospective data collection. This study was approved by the Institutional Review Board of PRISMA Health institutional committee for ethics (approval number: 00052571). All data were fully anonymized before they were accessed. Data used in our retrospective analysis were from the PRISMA Health stroke data registry. This study did not require informed consent for participation by the national legislation and institutional requirements.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ojo, D.T., Brewer, P.C., Imeh-Nathaniel, A. et al. Sex differences in clinical risk factors in obese ischemic stroke patients with a history of smoking. BMC Cardiovasc Disord 24, 288 (2024). https://doi.org/10.1186/s12872-024-03952-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-024-03952-6