
Abstract
Background
The effect of nonalcoholic fatty liver disease (NAFLD) on major adverse cardiovascular events (MACEs) can be influenced by the degree of coronary artery stenosis. However, the association between the severity of NAFLD and MACEs in patients who underwent coronary computed tomography angiography (CCTA) is unclear.
Methods
A total of 341 NAFLD patients who underwent CCTA were enrolled. The severity of NAFLD was divided into mild NAFLD and moderate-severe NAFLD by abdominal CT results. The degree of coronary artery stenosis was evaluated by using Coronary Artery Disease Reporting and Data System (CAD-RADS) category. Cox regression analysis and Kaplan–Meier analysis were used to assess poor prognosis.
Results
During the follow-up period, 45 of 341 NAFLD patients (13.20%) who underwent CCTA occurred MACEs. The severity of NAFLD (hazard ratio [HR] = 2.95[1.54–5.66]; p = 0.001) and CAD-RADS categories 3–5 (HR = 16.31[6.34–41.92]; p < 0.001) were independent risk factors for MACEs. The Kaplan–Meier analysis showed that moderate to severe NAFLD patients had a worsen prognosis than mild NAFLD patients (log-rank p < 0.001). Moreover, the combined receiver operating characteristic curve of the severity of NAFLD and CAD-RADS category showed a good predicting performance for the risk of MACEs, with an area under the curve of 0.849 (95% CI = 0.786–0.911).
Conclusion
The severity of NAFLD was independent risk factor for MACEs in patients with obstructive CAD, having CAD-RADS 3–5 categories on CCTA.
Similar content being viewed by others


Introduction
Coronary computed tomography angiography (CCTA) has become a first-line recommendation for screening patients with suspected coronary artery disease (CAD) and is widely used to detect coronary stenosis and analysis plaque characteristics. Due to CCTA can monitor early changes of CAD, it has become a new and valuable prognostic tool for evaluating major adverse cardiovascular events (MACEs) [1, 2]. Previous studies showed the prognosis value of CCTA in nonalcoholic fatty liver disease (NAFLD) patients [3, 4] and NAFLD patients with CAD have a high risk of MACEs. Because of the prognosis of CAD patients depending on the degree of coronary artery stenosis, the effect of NAFLD on MACEs may be influenced by the degree of coronary artery stenosis [3].
The severity of NAFLD is independently associated with carotid atherosclerosis [5, 6] and moderate to severe NAFLD patients had a higher incidence of future ischemic stroke events [7]. The severity of NAFLD also closely correlates with cardiac complications, such as aortic valve calcification, arrhythmias, epicardial fat thickness, and left ventricular hypertrophy et al. [8,9,10]. And moderate to severe NAFLD patients with hypertension have a higher risk of all-cause death compared with mild NAFLD patients [11, 12]. However, the association is unclear between the severity of NAFLD and MACEs in patients with different degrees of coronary artery stenosis.
Therefore, our current study was to investigate the association between the severity of NAFLD and MACEs in patients assessed by CCTA and evaluated predicting performance of the severity of NAFLD and degree of coronary artery stenosis for the risk of MACEs.
Methods
Patients
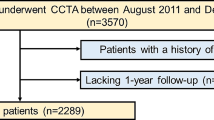
We retrospectively analyzed the continuous patients who received CCTA examination and simultaneously underwent unenhanced abdominal CT within one week in our institution between July 2012 and March 2022. The exclusion criteria were as follows: [1] a history of alcohol abuse, with outweigh 30 g/d in men and 20 g/d in women [13]; [2] history of liver cirrhosis or positive hepatitis B surface antigen or hepatitis C virus antibodies or hepatoma; [3] history of cancer; [4] previous history of myocardial infarction or coronary artery revascularization; [5] poor image quality of CCTA; and [6] individuals who lost follow-up. The flowchart of inclusion and exclusion criteria for this study is shown in Fig. 1. Finally, a total of 341 NAFLD patients were included in this research. The non-NAFLD patients incorporated 145 patients who also underwent CCTA examination and unenhanced abdominal CT as a control group.

The flowchart of inclusion and exclusion criteria. CCTA, coronary CT angiography; NAFLD, non-alcoholic fatty liver disease; CAD-RADS, coronary artery disease reporting and data system; MACEs, major adverse cardiovascular events
The requirement for informed consent was waived by Ethics Committee of Shandong Provincial Hospital Affiliated to Shandong First Medical University.
CCTA image acquisition
Routine coronary computed tomography angiography (CCTA) dates were obtained by dual-source CT scanner (Aquilion ONE, TOSHIBA; Somatom Flash or Force, Siemens Healthineers). Before scanning, all patients sprayed nitroglycerin sublingually to dilate the coronary artery and received breath-holding training to reduce respiratory motion artifacts. CCTA was performed by using a bolus tracking technique, with regions of interest placed in the root of the aorta. Detailed CCTA parameters are listed in Supplementary E1.
Image reconstruction and assessment of CCTA
The degree of coronary artery stenosis was evaluated by using the Coronary Artery Disease Reporting and Data System (CAD-RADS) category [14]. A dedicated plaque analysis software (Coronary Plaque Analysis, version 5.0.0, Siemens Healthineers, Germany) was used to measure the quantitative plaque parameters. The quantitative coronary perivascular fat attenuation index (FAI) was evaluated by using a dedicated FAI analysis software (Easy FAI, version 1.2, ShuKun, China).The detailed image evaluation were shown Supplementary E2.
Two radiologists with 20 years and 10 years of cardiac imaging experience, who were blinded to the NAFLD status and clinical outcome, independently analyzed imaging. The measured values were used for further analysis. Stenosis of the left main trunk ≥ 50% or non-left main trunk ≥ 70% is severe coronary artery stenosis, for which revascularization is often required. Coronary artery stenosis with 40–69% are moderately narrow and usually require further functional evaluation [15].
The severity of NAFLD definition and measurement
The severity of NAFLD was defined by liver attenuation minus spleen attenuation (L-S) on unenhanced CT. We defined L-S≤-10HU to indicate moderate to severe NAFLD [16]. The reviewers who measured liver and spleen attenuation were blinded to the patient’s clinical information. Liver and spleen Hounsfield units were obtained by drawing 3 circular regions of interest (ROI) with an area of at least 200 mm2 on different axial levels [3], and the ROI values were calculated as the average of the three measurements. We selected carefully sample homogeneous areas representative of the parenchyma, avoiding blood vessels, bile ducts, calcification, cyst, focal lesions, and surface margins.
Clinical outcomes
Clinical follow-up times were started after the time of the CCTA examination. Follow-up clinical dates were acquired by reviewing medical records or telephone interviews. The primary endpoint was the occurrence of MACEs, which were defined as all-cause death, nonfatal myocardial infarction, heart failure, and revascularization. Revascularization included percutaneous coronary intervention and coronary artery bypass grafting.
Statistical analysis
The intraclass correlation coefficient (ICC) was used to determine the interobserver reproducibility of the liver, spleen attenuation measurement, and lesion length. The agreement of CAD-RADS categories was tested with the Cohen k value. The SPSS version 26.0 and R version 4.0.1 software were used for statistical analysis. Continuous dates were depicted as mean ± standard deviation (SD) or median and quartiles, while categorical variables were showed as frequency with percentages.
Cox regression analysis was applied to reveal association between the severity of NAFLD and MACEs. The Kaplan-Meier analysis was used to assess the prognosis of NAFLD patients. Receiver operating characteristic (ROC) curves and area under the curve (AUC) were performed to assess the predictive performance of the severity of NAFLD and CAD-RADS category for MACEs in patients assessed by CCTA. All statistical tests were two-sided, with p < 0.05 considered statistically significant.
Results
Clinical baseline characteristics of patients
In this study, the median age of the registered patients was 59 years and 138 (40.47%) of patients were men. The demographic characteristics and laboratory data of the non-NAFLD patients, mild NAFLD patients, and moderate to severe NAFLD patients were shown in Table 1. Compared with mild NAFLD patients, the moderate to severe NAFLD patients had higher aspartate aminotransferase (AST), alanine aminotransferase (ALT), total cholesterol (TC), and low-density lipoprotein cholesterol (LDL-C) (all p < 0.05). Both groups had no statistical difference in the presence of diabetes mellitus, and level of gamma glutamyl transferase (GGT), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), glucose (GLU), and uric acid (URIC) (all p > 0.05). The NAFLD patients were more likely to have diabetes mellitus and had higher AST, ALT, GGT, TG, LDL-C, GLU, URIC, and lower HDL-C than that of non-NAFLD patients (all p < 0.05).
Quantitative parameters (plaque features and FAI) based on CCTA were compared among the non-NAFLD, mild NAFLD, and moderate to severe NAFLD patients
Though no statistically significant difference in CAD-RADS category was observed between the mild NAFLD patients and moderate to severe NAFLD patients, the latter had a higher proportion of CAD-RADS categories 3–5 than the former. FAI of three coronary arteries had statistical difference between mild NAFLD patients and moderate to severe NAFLD patients (all p < 0.05). The detailed results were shown in Table 1. As presented in Table 2, moderate to severe NAFLD patients had lower calcified plaque volume and calcified plaque volume ratio compared with mild NAFLD patients (all p < 0.05). NAFLD patients had longer lesions range and higher fibrotic plaque volume and fibrotic plaque volume ratio than non-NAFLD patients. FAI of three coronary arteries also had statistical difference between NAFLD patients and non-NAFLD patients (all p < 0.05) (Table 1).
The interobserver reliabilities of the CAD-RADS category at CCTA was great (k = 0.96). The interobserver reliabilities of the liver and spleen CT attenuation measurement, and lesion length were excellent (ICC = 0.98 [95% confidence interval CI = 0.97–0.99], 0.93 [95% CI = 0.91–0.94] and 0.98 [95% CI = 0.96–0.99], respectively).
The severity of NAFLD and CAD-RADS categories 3–5 were significantly independent risk factors for MACEs
The median time of follow-up was 28 months (interquartile range, 10.0–46.0 months). During the follow-up period, 45 of 341 patients (13.20%) had occurred MACEs in patients assessed by CCTA. On univariate analysis, men (hazard ratio [HR] = 1.99; 95% CI = 1.10–3.59; p = 0.022), history of smoking (HR = 3.23; 95% CI = 1.74–6.01; p < 0.001), CREA (HR = 1.02; 95% CI = 1.00–1.03; p = 0.014), severity of NAFLD (HR = 3.32; 95% CI = 1.75–6.30; p < 0.001), and CAD-RADS categories 3–5 (HR = 18.79; 95% CI = 7.39–47.75; p < 0.001) were significantly associated with MACEs. On multivariate analysis, the severity of NAFLD (HR = 2.95; 95% CI = 1.54–5.66; p = 0.001) and CAD-RADS categories 3–5 (HR = 16.31; 95% CI = 6.34–41.92; p < 0.001) were independent risk factors for MACEs. Detailed results were provided in Table 3.
The Kaplan–Meier curves analysis was used to compare the survival rate of the two groups and further evaluate their poor prognosis (Fig. 2). The 1-, 3-, and 5-year survival rates in the moderate to severe NAFLD patients were significantly lower than mild NAFLD patients (84.8%, 81.4%, and 68.4% vs. 94.2%, 92.5%, and 92.5%, respectively). The moderate to severe NAFLD patients had a worsen prognosis than mild NAFLD patients (log-rank p < 0.001).

Kaplan–Meier curve of different severity of NAFLD in patients assessed by CCTA. Survival rate of moderate to severe NAFLD patients compared with mild NAFLD patients
Performance of the severity of NAFLD and CAD-RADS category for predicting the risk of MACEs
The ROC curves of the severity of NAFLD and CAD-RADS category for predicting the risk of MACEs were shown in Fig. 3. The AUCs of the severity of NAFLD and CAD-RADS categories were 0.642 (95% CI = 0.557–0.727) and 0.808 (95% CI = 0.745–0.870), respectively. The combined ROC curve showed a good predicting performance, with an AUC of 0.849 (95% CI = 0.786–0.911). The most appropriate cutoff values of the combined ROC curve and CAD-RADS category curve only in predicting the risk of MACEs were set at 0.121 using the Youden index. The sensitivity and specificity were 88.9% and 72.6%, respectively.

The predictive performance of severity of NAFLD and CAD-RADS category for the risk of MACEs.
The severity of NAFLD was an independent predictor for MACEs in patients with CAD-RADS categories 3–5
During the follow-up times, MACEs were observed in 11 of 61 mild NAFLD patients (18.03%) and 29 of 60 moderate to severe NAFLD patients (48.33%) in patients with CAD-RADS categories 3–5. On univariate analysis, age (HR = 0.96; 95% CI = 0.93–0.99; p = 0.021), hypertension (HR = 0.51; 95% CI = 0.27–0.96; p = 0.036), and the severity of NAFLD (HR = 3.19; 95% CI = 1.59–6.42; p = 0.001) were associated with MACEs in patients with CAD-RADS categories 3–5. On multivariate analysis, the severity of NAFLD (HR = 2.94; 95% CI = 1.45–5.94; p = 0.003) was an independent predictor for MACEs. On the contrary, all factors had no statistical difference for MACEs in patients with CAD-RADS categories 0–2, including the severity of NAFLD (HR = 1.48; 95%CI = 0.23–9.45; p = 0.681) (Table 4).
The Kaplan–Meier curves analysis was used to show the survival rate. There was not statistical difference between the mild NAFLD patients and moderate to severe NAFLD patients with CAD-RADS categories 0–2 (log-rank P = 0.68) (Fig. 4A). The moderate to severe NAFLD patients had a poor prognosis compared with mild NAFLD patients with CAD-RADS categories 3–5 (log-rank P < 0.001) (Fig. 4B). The 1-, 3-, and 5-year survival rates of moderate to severe NAFLD patients were significantly lower than mild NAFLD patients with CAD-RADS categories 3–5 (61.7%, 55.7%, and 30.6% vs. 85.0%, 78.1%, and 78.1%, respectively).

Kaplan–Meier curves of MACEs stratified according to CAD-RADS categories at CCTA in patients with mild NAFLD and moderate to severe NAFLD. (A) Survival rate of moderate to severe NAFLD patients compared with mild NAFLD patients in the CAD-RADS categories 0–2. (B) Survival rate of moderate to severe NAFLD patients compared with mild NAFLD patients in the CAD-RADS categories 3–5
Discussion
In the present study, the severity of NAFLD was independent risk factor for MACEs in patients assessed by CCTA and moderate to severe NAFLD patients had a lower survival rate than mild NAFLD patients. The combined ROC curve of the severity of NAFLD and CAD-RADS category showed a good predicting performance for the risk of MACEs in patients assessed by CCTA.
Previous study reported that NAFLD was associated with calcified plaque, which is an independent predictor of CAD and cardiovascular outcome [17, 18]. Our results found moderate to severe NAFLD patients had lower calcified plaque volume and calcified plaque volume ratio than mild NAFLD patients. The reason might be that the aggravation of NAFLD severity may lead to liver dysfunction, insulin resistance, oxidative stress, arterial intimal dysfunction, and lipid metabolism abnormalities. When coronary artery is involved, forming atherosclerosis and coronary plaque, the number of plaques containing lipid components would also increase. Of course, the detailed association and mechanisms need to be further explored and confirmed through large sample and basic research. Previous study showed that the severity of NAFLD is associated with metabolic syndrome, including hypertension, liver aminotransferase, and dyslipidemia et al. [19]. Our results found that the ALT, AST, TC, and LDL-C levels were correlated with the severity of NAFLD according to the Spearman analysis. Though with limited roles in predicting the severity of NAFLD, increasing levels of these serum biomarkers may represent the mechanistic link with the severity of NAFLD [20], which further basic research is needed to confirm. FAI, as a part of the epicardial adipose tissue, could reflect the inflammation of the coronary artery on CCTA. Previous studies has been demonstrated that FAI is related to NAFLD, which our results was similar with it [21]. Epicardial adipose tissue also was associated with coronary artery disease assessed by CCTA. Previous studies demonstrated importance of epicardial adipose tissue volume to identify increased high-risk plaque and pericoronary adipose tissue inflammation [22]. However, the data of epicardial adipose tissue volume are not available in our hospital. It need to be studied further in the future.
It has been demonstrated that poor prognosis of liver-related disease increases progressively with the severity of NAFLD [23, 24]. A recent Swedish nationwide cohort study including 10,568 adults who were confirmed as NAFLD by liver histopathology suggested that the high all-cause mortality increased progressively with the severity of NAFLD [25]. However, much less is known about the association between the severity of NAFLD and poor cardiovascular outcomes. The major finding of the current study was that the severity of NAFLD was independent risk factor for MACEs in patients assessed by CCTA. Previous studies showed that the remission of severity of NAFLD may ultimately improve the prognosis of cerebrovascular and cardio-metabolic disease [6, 26]. It suggested that the severity of NAFLD plays an important role in poor cerebrovascular and cardiovascular outcomes, including the MACEs.
Our study clearly showed that the severity of NAFLD can provide important prognostic information for patients who underwent CCTA. Moderate to severe NAFLD patients had significantly lower survival rates than mild NAFLD patients during the follow-up period. We considered that the result mainly was related to the liver fat content of patients. Previous epidemiological studies reported that high liver fat content is likely to have a high risk of ischemic heart disease [27, 28] and impaired myocardial metabolism [5]. The potential mechanisms may be that severe NAFLD may contribute to MACEs by stimulating platelet activation or by aggravating systemic inflammation, liver insulin resistance, macrophage activation, increased oxidative stress, endothelial dysfunction, and altered lipid metabolism [29, 30]. Therefore, it is important to evaluate the severity of NAFLD, which may provide the opportunity to prevent progress of related complications and to reduce incidence of MACEs.
Moreover, we also evaluated predicting performance of the severity of NAFLD and CAD-RADS category for the risk of MACEs. The combined ROC curve of the severity of NAFLD and CAD-RADS category showed a good predicting performance with an AUC of 0.849, which was higher than the severity of NAFLD only and CAD-RADS category only, with AUC of 0.642 and 0.808, respectively. These results suggested that simultaneously evaluating the severity of NAFLD and CAD-RADS category would improve the detection of patients at higher risk of adverse cardiovascular events. Because these patients need more active medical strategies to alleviate symptoms and further improve prognosis [31].
It is vital to early identify and manage patients at high risk for different severity of NAFLD. The severity of NALFD was a significant independent predictor for MACEs in patients with CAD-RADS categories 3–5 in our study. Notably, our results showed that moderate to severe patients with CAD-RADS categories 3–5 have a relatively worsen prognosis and the survival rates reduce by about 70% within five years, which further elucidated the importance of assessing timely severity of NAFLD in patients with CAD-RADS categories 3–5 for reducing the risk of MACEs.
This study has several limitations. Firstly, this is a single-center retrospective study, and the small sample size, which might take inevitable selection bias. Secondly, the CT scanning images are obtained from different scanners, and lifestyle modification and medical therapies can modify severity of NAFLD. These issues need to be further settled in a future mulita-center prospective study with a large sample.
Conclusion
In conclusion, this study showed that the severity of NAFLD was independent risk factor for MACEs in with obstructive CAD, having CAD-RADS 3–5 categories on CCTA. And moderate to severe NAFLD patients had a worsen prognosis than mild NAFLD patients. Early assessing the severity of NAFLD is important and it may help clinicians formulate individualized treatment.
Data availability
The data sets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ALT:
-
Alanine aminotransferase
- AST:
-
Aspartate aminotransferase
- AUC:
-
Area under the curve
- CAD:
-
Coronary artery disease
- CAD-RADS:
-
Coronary Artery Disease Reporting and Data System
- CCTA:
-
Coronary computed tomography angiography
- CI:
-
Confidence interval
- CREA:
-
Creatinine
- FAI:
-
Fat attenuation index
- GGT:
-
Gamma glutamyl transferase
- GLU:
-
Glucose
- HDL-C:
-
High-density lipoprotein cholesterol
- HR:
-
Hazard ratio
- ICC:
-
Intraclass correlation coefficient
- LDL-C:
-
Low-density lipoprotein cholesterol
- MACEs:
-
Major adverse cardiovascular events
- NAFLD:
-
Nonalcoholic fatty liver disease
- ROC:
-
Receiver operating characteristic
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
- URIC:
-
Uric acid
References
Hadamitzky M, Täubert S, Deseive S, Byrne RA, Martinoff S, Schömig A, et al. Prognostic value of coronary computed tomography angiography during 5 years of follow-up in patients with suspected coronary artery disease. Eur Heart J. 2013;34(42):3277–85.
Chow BJW, Wells GA, Chen L, Yam Y, Galiwango P, Abraham A, et al. Prognostic value of 64-slice cardiac computed tomography severity of coronary artery disease, coronary atherosclerosis, and left ventricular ejection fraction. J Am Coll Cardiol. 2010;55(10):1017–28.
Yu M-M, Tang X-L, Jin H, Yang S, Yun H, Wang Q-B, et al. Coronary CT angiography in asymptomatic adults with Hepatic Steatosis. Radiology. 2021;301(3):593–601.
Ichikawa K, Miyoshi T, Osawa K, Miki T, Nakamura K, Ito H. Prognostic Value of Coronary computed Tomographic Angiography in patients with nonalcoholic fatty liver disease. JACC Cardiovasc Imaging. 2020;13(7):1628–30.
Bhatia LS, Curzen NP, Calder PC, Byrne CD. Non-alcoholic fatty liver disease: a new and important cardiovascular risk factor? Eur Heart J. 2012;33(10):1190–200.
Bhatia L, Scorletti E, Curzen N, Clough GF, Calder PC, Byrne CD. Improvement in non-alcoholic fatty liver disease severity is associated with a reduction in carotid intima-media thickness progression. Atherosclerosis. 2016;246:13–20.
Song Q-R, Liu S-L, Ling Q-H, Gao Q-N, Yang R-X, Chen S-H, et al. Severity of nonalcoholic fatty liver disease is Associated with Cardiovascular outcomes in patients with prehypertension or hypertension: a community-based Cohort Study. Front Endocrinol (Lausanne). 2022;13:942647.
Targher G, Corey KE, Byrne CD. NAFLD, and cardiovascular and cardiac diseases: factors influencing risk, prediction and treatment. Diabetes Metab. 2021;47(2):101215.
Jung JY, Park SK, Ryoo J-H, Oh C-M, Kang JG, Lee J-H, et al. Effect of non-alcoholic fatty liver disease on left ventricular diastolic function and geometry in the Korean general population. Hepatol Res. 2017;47(6):522–32.
Liu B, Li Y, Li Y, Liu Y, Yan Y, Luo A, et al. Association of epicardial adipose tissue with non-alcoholic fatty liver disease: a meta-analysis. Hepatol Int. 2019;13(6):757–65.
Xu J, Dai L, Zhang Y, Wang A, Li H, Wang Y, et al. Severity of nonalcoholic fatty liver disease and risk of future ischemic stroke events. Stroke. 2021;52(1):103–10.
Tang ASP, Chan KE, Quek J, Xiao J, Tay P, Teng M, et al. Non-alcoholic fatty liver disease increases risk of carotid atherosclerosis and ischemic stroke: an updated meta-analysis with 135,602 individuals. Clin Mol Hepatol. 2022;28(3):483–96.
Chalasani N, Younossi Z, Lavine JE, Diehl AM, Brunt EM, Cusi K, et al. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology. 2012;142(7):1592–609.
Cury RC, Leipsic J, Abbara S, Achenbach S, Berman D, Bittencourt M, et al. Computed Tomography (SCCT), the American College of Cardiology (ACC), the American College of Radiology (ACR), and the North America Society of Cardiovascular Imaging (NASCI). JACC Cardiovasc Imaging. 2022;15(11):1974–2001. CAD-RADS™ 2.0–2022 Coronary Artery Disease-Reporting and Data System: An Expert Consensus Document of the Society of Cardiovascular.
Lawton JS, Tamis-Holland JE, Bangalore S, Bates ER, Beckie TM, Bischoff JM, et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery revascularization: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice guidelines. Circulation. 2022;145(3):e4–17.
Park SH, Kim PN, Kim KW, Lee SW, Yoon SE, Park SW, et al. Macrovesicular hepatic steatosis in living liver donors: use of CT for quantitative and qualitative assessment. Radiology. 2006;239(1):105–12.
Kang MK, Kang BH, Kim JH. Nonalcoholic fatty liver disease is Associated with the Presence and morphology of subclinical coronary atherosclerosis. Yonsei Med J. 2015;56(5):1288–95.
Park HE, Kwak MS, Kim D, Kim MK, Cha MJ, Choi SY. Nonalcoholic fatty liver disease is Associated with Coronary Artery Calcification Development: a longitudinal study. J Clin Endocrinol Metab. 2016;101(8):3134–43.
Sheka AC, Adeyi O, Thompson J, Hameed B, Crawford PA, Ikramuddin S. Nonalcoholic steatohepatitis: a review. JAMA. 2020;323(12):1175–83.
Lim S, Oh TJ, Koh KK. Mechanistic link between nonalcoholic fatty liver disease and cardiometabolic disorders. Int J Cardiol. 2015;201:408–14.
Ren Z, Wen D, Xue R, Li S, Wang J, Li J, et al. Nonalcoholic fatty liver disease is associated with myocardial ischemia by CT myocardial perfusion imaging, independent of clinical and coronary CT angiography characteristics. Eur Radiol. 2023;33(6):3857–66.
Yamaura H, Otsuka K, Ishikawa H, Shirasawa K, Fukuda D, Kasayuki N. Determinants of non-calcified low-attenuation coronary plaque burden in patients without known coronary artery disease: a coronary CT Angiography Study. Front Cardiovasc Med. 2022;9:824470.
Taylor RS, Taylor RJ, Bayliss S, Hagström H, Nasr P, Schattenberg JM et al. Association between Fibrosis Stage and outcomes of patients with nonalcoholic fatty liver disease: a systematic review and Meta-analysis. Gastroenterology. 2020;158(6).
Dulai PS, Singh S, Patel J, Soni M, Prokop LJ, Younossi Z, et al. Increased risk of mortality by fibrosis stage in nonalcoholic fatty liver disease: systematic review and meta-analysis. Hepatology. 2017;65(5):1557–65.
Simon TG, Roelstraete B, Khalili H, Hagstrom H, Ludvigsson JF. Mortality in biopsy-confirmed nonalcoholic fatty liver disease: results from a nationwide cohort. Gut. 2021;70(7):1375–82.
Musso G, Cassader M, Rosina F, Gambino R. Impact of current treatments on liver disease, glucose metabolism and cardiovascular risk in non-alcoholic fatty liver disease (NAFLD): a systematic review and meta-analysis of randomised trials. Diabetologia. 2012;55(4):885–904.
Targher G, Day CP, Bonora E. Risk of cardiovascular disease in patients with nonalcoholic fatty liver disease. N Engl J Med. 2010;363(14):1341–50.
Lauridsen BK, Stender S, Kristensen TS, Kofoed KF, Køber L, Nordestgaard BG, et al. Liver fat content, non-alcoholic fatty liver disease, and ischaemic heart disease: mendelian randomization and meta-analysis of 279 013 individuals. Eur Heart J. 2018;39(5):385–93.
Schuster S, Cabrera D, Arrese M, Feldstein AE. Triggering and resolution of inflammation in NASH. Nat Rev Gastroenterol Hepatol. 2018;15(6):349–64.
Polimeni L, Del Ben M, Baratta F, Perri L, Albanese F, Pastori D, et al. Oxidative stress: new insights on the association of non-alcoholic fatty liver disease and atherosclerosis. World J Hepatol. 2015;7(10):1325–36.
Ichikawa K, Miyoshi T, Osawa K, Miki T, Toda H, Ejiri K, et al. Incremental prognostic value of non-alcoholic fatty liver disease over coronary computed tomography angiography findings in patients with suspected coronary artery disease. Eur J Prev Cardiol. 2022;28(18):2059–66.
Acknowledgements
We sincerely thank Feier Ding (Department of Radiology, Shandong Provincial Hospital) for assistance with statistical analysis, Sha Li ((Department of Radiology, Shandong Provincial Hospital)) for assistance with clinic follow-up and Songbo Zhao (Department of Central Laboratory, Shandong Provincial Hospital, Shandong University) for assistance with design and supervision of the study.
Funding
This research was supported by the Natural Science Foundation of China (NSFC; 81871354 and 82271993).
Author information
Authors and Affiliations
Contributions
Xm. W, Xy. Z, Zq. L, and Rc. S conceived and designed the study. Rc. S, Xm. L, Fy. L and Bs. Z acquired the data and implemented quality control of data. Rc. S, Xm. L and Yl. W did the clinic follow-up. K. S, Rc. S, and B. K performed the statistical analysis. K. S and Y. W made figures and tables. Rc. S, Xm. L, Xy. Z and Zq. L prepared the draft of the manuscript. Rc. S, Xm. L, Zq. L, Xy. Z and Xm. W reviewed the manuscript. Xm. W and Zq. L had direct access to verify the data.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The requirement for informed consent was waived by Ethics Committee of Shandong Provincial Hospital Affiliated to Shandong First Medical University due to the retrospective nature of this study. All methods were performed in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material. (no find link)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shi, R., Li, X., Sun, K. et al. Association between severity of nonalcoholic fatty liver disease and major adverse cardiovascular events in patients assessed by coronary computed tomography angiography. BMC Cardiovasc Disord 24, 267 (2024). https://doi.org/10.1186/s12872-024-03880-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-024-03880-5