
Abstract
Background
Cardiovascular disorders (CVDs) are the leading cause of death worldwide. This study aimed to evaluate the association between low-density lipoprotein (LDL) subfractions and cardiovascular disorders.
Methods
To ensure the rigor of the systematic review, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used. For this systematic review, a comprehensive search strategy was performed in important databases including PubMed, Scopus, Embase, International Statistical Institute (ISI) Web of Science, and google scholar from 2009 to February 2021. The following terms were used for systematic search: low-density lipoprotein, LDL, subfractions, subclasses, nuclear magnetic resonance, NMR, chromatography, high-pressure liquid, HPLC, cardiovascular disease, cerebrovascular, and peripheral vascular disease. Also, for evaluating the risk of bias, the Newcastle-Ottawa scale was employed.
Results
At the end of the search process, 33 articles were included in this study. The results of most of the evaluated studies revealed that a higher LDL particle number was consistently associated with increased risk for cardiovascular disease, independent of other lipid measurements. Also, small dense LDL was associated with an increased risk of CVDs. There was no association between LDL subfraction and CVDs in a small number of studies.
Conclusions
Overall, it seems that the evaluation of LDL subclasses can be used as a very suitable biomarker for the assessment and diagnosis of cardiovascular diseases. However, further studies are required to identify the mechanisms involved.
Similar content being viewed by others
Background
Cardiovascular disease is one of the leading causes of mortality in many countries [1]. Various factors, especially increased obesity, an inactive lifestyle, stress, and diseases such as diabetes and dyslipidemia have increased the risk of cardiovascular complications [2]. According to the Adult Treatment Panel III of the Expert Panel of the National Cholesterol Education Program recommendations, increased low-density lipoprotein (LDL) and reduction in high-density lipoprotein (HDL) levels are among the main risk factors for cardiovascular disease [3]. Various results from clinical trials as well as studies evaluating LDL genetic variants have indicated that treatment with statins and other therapies aimed at reducing LDL concentrations can prevent and reduce the risk of cardiovascular events [4,5,6]. Thus, LDL-lowering therapies are recommended by both European [7] and American guidelines [8] to prevent cardiovascular disease. Also, it has been reported in arteriographic investigations that any interventions to lower serum LDL and elevate HDL concentrations may reduce the rate of arteriographically defined disease progression [9,10,11].
Recognizing the role of LDL as a serious risk factor for cardiovascular disease, one of the questions that has arisen is whether the size of LDL particles and different subtypes of LDL plays the same role in the etiology of cardiovascular failure. It has been reported that some conditions such as metabolic syndrome, diabetes, familial combined hyperlipidemia, and hyperapobetalipoproteinemia (hyper-apoB) would elevate the concentration of small atherogenic LDL and lead to cardiovascular disease, as summarized in Fig. 1 [12, 13].
On the other hand, it has been shown that the effect of drug treatment such as statin therapy or Proprotein Convertase Subtilisin/Kexin type 9 (PCSK9) inhibitors was not the same in patients with high LDL levels, raising suspicion among researchers and physicians that differences in observed effects may be due to different concentrations of LDL subclasses [14,15,16]. Different terms are used to describe the characteristics and distribution of LDL particles such as LDL subclasses, subfraction and particle concentration, though all of these terms have almost the same meaning, and more attention has been paid to LDL subclasses since subclass separation techniques. Some studies have reported that small dense LDL (sdLDL) particles are at greater atherogenic risk than larger, less dense LDL, while some results are contradictory [17, 18]. Indeed, some studies have suggested that sdLDL are more taken up by macrophages and are at higher risk for oxidation. On the other hand, these particles easily penetrate into the subendothelial space and attach to the arterial wall, thus increasing the risk of atherosclerosis [19, 20]. A systematic review study conducted in 2009 by Stanley et al. [21] assessed the association between LDL subgroups and the incidence of cardiovascular Outcomes. However, the results of this study were contradictory and the authors of this article recommended that further studies be conducted to identify the mechanisms involved.
Due to the contradictory results and limitations mentioned in different studies, this updated systematic review study aimed to investigate the relationship between different LDL subclasses and the risk of cardiovascular disease.

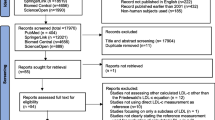
Flow chart of study selection
Method
Search strategy
To ensure the rigor of this systemic review, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used [22]. For this systematic review, a comprehensive search strategy was employed in important databases including PubMed, Scopus, Embase, International Statistical Institute (ISI) Web of Science, and google scholar from 2009 to February 2021. In order not to miss an article, manual searching was performed. For systematic search, the following search strategy was used: (“Low-density lipoprotein” OR Cholesterol, LDL OR LDL OR lipoprotein) AND (particle size.mp. OR subfractions OR subclasses OR “Nuclear Magnetic Resonance” OR Biomolecular/ OR exp Magnetic Resonance Spectroscopy/ OR “nuclear magnetic resonance” OR NMR OR “magnetic resonance spectroscopy” OR Chromatography OR “High-Pressure Liquid” OR HPLC OR ultracentrifugation.mp OR centrifugation.mp OR Electrophoresis) AND (“cardiovascular disease” OR cerebrovascular OR peripheral vascular disease OR Cardiovascular OR Cardio* OR Atherosclerosis).
Criteria for selecting articles
Table 1 summarizes the population, interventions, comparators, and outcomes (PICOS) criteria for eligibility of studies. Articles were included in this study if they met the following criteria: prospective, longitudinal, and cross-sectional design which evaluated the association between LDL subfractions and cardiovascular disease, participation of at least 10 people in the study, serum (or plasma) samples must have been obtained before determination of outcomes, evaluation of specific clinical outcome such as minimum lumen diameter.
The results of a systematic search for initial screening were entered into the EndNote software. After eliminating duplicate studies, the two authors independently evaluated the titles and abstracts of the articles. In the second stage, the researchers evaluated the full text of the remaining articles and the studies that met the necessary criteria were included in the final analysis. Also, studies with low methodological quality were detected. Data such as authors, country of study, method of assessing LDL levels, cardiovascular disease, etc. were extracted.
Risk of bias assessment
For evaluating the risk of bias, the Newcastle-Ottawa scale was used [23]. NOS was developed to evaluate the quality of nonrandomized studies, including cross-sectional, case-control, and cohort studies. This assessment allowed a total score of up to 9 points. The NOS for cohort studies was divided into three groups: selection of cohort (4 points), comparability of cohort (2 points), and assessment of outcome (3 points). The quality of the study was considered high or moderate if the sum score was ≥ 8 points or between 5 and 7 points, respectively.
Results
Characteristics of the included studies
In total, after searching the mentioned databases, 5723 studies entered the Endnote 20 software and after removing duplicate articles, 3890 articles remained for initial screening. Following the initial screening, 88 studies were chosen to evaluate the full text of these articles, and among them, finally, 33 articles were included in this study (Table 2). The flow chart of study selection has been presented in Fig. 1.
From those articles included, based on the design of studies, 20 studies had cross-sectional, 5 prospective cohort design, and 8 studies had a case-control design.
For evaluating LDL subclasses, 17 studies had employed NMR spectroscopy, 8 studies gel electrophoresis, one study HPLC, two studies liquid chromatography, one study electrical mobility, and four studies the ion mobility ultracentrifugation and lipoprint system.
Based on the Newcastle–Ottawa checklist, regarding the score of methodological quality, all included studies except six [4, 24,25,26,27,28] had high quality (more than 7 scores) (Table 3).
NMR-measured LDL subfractions
Among the studied studies, 17 studies had utilized the NMR method to evaluate LDL subfraction. Pallarés et al. [29] in a cross-sectional study conducted on 400 participants, reported that subjects with higher concentrations of small LDL particle size had a higher chance of developing cardiovascular disease. Also, Notarnicola et al. [30] showed that higher concentrations of sdLDL would increase the risk of mortality in patients with CVDs. In line with the two studies mentioned, other studies reported similar results [24, 25, 31,32,33,34]. Further, some studies have specifically examined the association between LDL subtypes and the incidence of various cardiovascular diseases. Cure et al. in a case-control study among patients with ischemic stroke reported that the level of sd‑LDL was 8.2 ± 7.8 mg/dL in the stroke group, which was significantly higher than the control group. However, the concentration of total LDL and large particles of LDL did not differ significantly between the two groups [35]. Also, Zeljkovic et al. in a cross-sectional study evaluated the concentration of various LDL subfractions among 100 patients with acute ischemic stroke and found that acute ischemic stroke (AIS) patients had significantly more LDL III and IV, but fewer LDL I and II particles [36].
LDL subfractions and coronary artery calcification (CAC)
Aneni et al. in a study conducted among 182 high cardiometabolic risk participants evaluated the association between LDL subfraction and risk of CAC. The result of this study revealed that subjects with higher concentrations of small/medium LDL subfractions had a higher risk for CAC odds compared to the participants with large LDL subfractions [37]. Prado et al. in a cross-sectional study evaluated the association between LDL subfractions and CAC among the 284 adults at intermediate risk of cardiovascular disease. They reported that the risk of CAC was 3.7 times higher in people with higher tertile of LDL particle (LDL-P) number [38]. Also, Jug et al. showed that serum concentration of small dense LDL lipoprotein was an independent predictor of CAC among the 410 patients at intermediate cardiovascular risk [26]. However, contrary to the results of the three studies mentioned, Chung et al. in a case-control study among 139 patients with rheumatoid arthritis concluded that there was no significant association between small LDL concentration and CAC [39].
LDL subfractions and stroke risk as well as atherosclerosis
Antonio et al. in a case-control study among 112 women with type 1 diabetes reported that patients with higher LDL particle (LDL-P) had a higher risk for atherosclerosis. Also, participants with higher concentrations of small LDL showed a higher risk for atherosclerosis and stroke [40]. Further, Duan et al. in a study on 566 patients with AIS reported that patients with AIS had a significantly higher concentration of LDL-3, LDL-4, and LDL-5 subclasses as well as lower concentration of LDL1 compared to the non-AIS participants [41]. A similar finding was observed in Chang et al. study [42]. In addition, Žitňanová et al. in a cross-sectional study which evaluated the association between LDL subfraction and AIS outcome, found that the serum concentration of anti-atherogenic large LDL1 subfractions was significantly lower in patients with AIS, and in contrast, they have a higher concentration of LDL3 and LDL5, which atherogenic properties [43].
Discussion
The present study has been a systematic review evaluating the association between LDL subclasses and cardiovascular disease. The results of the study revealed that participants with higher concentrations of small dense LDL were at a higher risk for CVDs. Additionally, we found that subjects with CVDs or those at risk for CVDs had higher concentrations of atherogenic LDL subclasses, such as LDL3 and LDL5.
In numerous countries, cardiovascular disease has emerged as a primary cause for mortality. Several articles have put different etiologies and theories for CVDs, among which a significant one is the rise in LDL levels, comprising seven subclasses (LDL-1 to LDL-7) [44]. The studies conducted so far on how LDL subclasses are linked to the development of different cardiovascular diseases have produced inconsistent findings [45, 46]. As the importance of evaluating LDL subclasses to predict cardiovascular disease has expanded, various methods have been developed to evaluate them [47]. For evaluating LDL subclasses, 17 studies had used NMR spectroscopy, 8 studies gel electrophoresis, one study HPLC, two studies liquid chromatography, one study electrical mobility, and four studies the ion mobility ultracentrifugation and lipoprint system. Most of the studies included in this systematic review had utilized the NMR spectroscopy method. NMR evaluates the number of LDL particles by applying a particular formula to measure the area and identifying the signal from the combined quantity of terminal methyl groups of the lipid present within the particle. Nonetheless, certain studies have employed the ultracentrifugation technique to assess LDL subgroups, where the separation of LDL subgroups is based on their density [48].
Although dyslipidemia is recognized as a traditional risk factor for cardiovascular disease, many patients with a history of acute vascular events have normal LDL levels. Concurrently,
Some people without any clinical or laboratory signs of CVDs exhibited higher concentrations of LDL-cholesterol [49, 50]. These findings promoted researchers to investigate and identify atherogenic and non-atherogenic subclasses of lipoproteins profiles. Some of the studies revealed that an atherogenic profile, characterized by elevated concentrations of VLDL, IDL1–3, small HDL, and especially by high levels of small dense LDL (LDL3–7) subfractions, can increase the risk of atherogenesis and CVDs. Meanwhile, the anti-atherogenic profile of lipoprotein subclasses, which includes a higher level of subtypes such as LDL1-2, large HDL, intermediate HDL and by only trace concentrations of LDL3–7 subfractions, has been identified by improving the body’s defenses against cardiovascular disease [51,52,53].
Despite numerous clinical and in vitro investigations, the precise mechanism behind the atherogenic effects of certain LDL subclasses remains uncertain. One proposed mechanism is that small, high-density LDL particles have a weaker binding affinity to hepatic LDL receptors, thus prolonging their clearance process [54]. Other researchers have suggested that elevated concentrations of small, dense LDL particles would increase their binding to intimal proteoglycans [55]. Additionally, LDL subclasses with smaller particles and higher density are more susceptible to oxidation, which leads to the formation of macrophage-derived foam cells, the hallmark of atherosclerotic plaques [56]. Furthermore, some studies have linked specific LDL subclasses to endothelial dysfunction [57].
The significance of examining lipoprotein subclasses has become so great that some associations that deal with cardiovascular diseases have included this field in their recommendations. While the American Heart Association still issues guidelines for treating CVD patients based on LDL levels, certain European associations, such as the European Society of Cardiology, suggest recommendations based on the level of LDL subclasses, such as sdLDL [58]. Evaluation of LDL subclasses can be used as a useful biomarker to identify people at risk for cardiovascular disease and to provide early preventive recommendations including diet and exercise [59].
The present review has been an updated systematic review, which evaluated observational studies evaluating the association between LDL subclasses and CVDs risk factors, incidence, and outcome. It has assessed results from 33 studies with a total of 12,320 subjects, providing substantial statistical power. Also, most of the studies had employed the same method to measure LDL subclasses, which is a standard method, though the evaluation method was different in some studies.
According to our knowledge, the present study has been the first systematic study examining the relationship between LDL subclasses and cardiovascular diseases. The current study had many strengths, including the systematic and comprehensive search across various databases, accurate and complete screening process, evaluation of methodological quality of studies with standard tools, and comprehensive review of all subclasses of LDL. Several limitations warrant discussion. One of the most important limitations of this study was the impossibility of meta-analysis due to the high heterogeneity of the studied outcomes. Also, the participants included in the studies in terms of health status or type of disease was a wide range, which can affect the accuracy of the results. Also, the consequences evaluated in different studies were adjusted for different confounding variables, which in turn can affect the accuracy of the results.
Conclusions
In conclusion, the assessment of LDL subclasses can be a useful biomarker for the evaluation and diagnosis of cardiovascular diseases. The results of this systematic review suggest that higher concentrations of small dense LDL particles are associated with increased risk for cardiovascular disease. However, further studies are needed to identify the mechanisms involved and to determine the clinical utility of measuring LDL subfractions in the management of cardiovascular disease.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CAC:
-
Coronary artery calcification
- CVDs:
-
Cardiovascular disorders
- LDL:
-
Low-Density Lipoprotein
- HDL:
-
High-Density Lipoprotein
- PICOS:
-
Population,interventions,comparators and outcomes
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- ISI:
-
International Statistical Institute
- AIS:
-
Acute Ischemic Stroke
- HPLC:
-
High-performance liquid chromatography
- NMR:
-
Nuclear magnetic resonance spectroscopy
- NOS:
-
Newcastle-Ottawa scale
- sdLDL:
-
Small dense LDL
- PCSK9:
-
Proprotein Convertase Subtilisin/Kexin type 9
References
Wilkins E, Wilson L, Wickramasinghe K, Bhatnagar P, Leal J, Luengo-Fernandez R. Europeancardiovasculardiseasestatistics2017.2017.
Thayer JF, Yamamoto SS, Brosschot JF. The relationship of autonomic imbalance, heart rate variability and Cardiovascular Disease risk factors. Int J Cardiol. 2010;141(2):122–31.
Cleeman J, Grundy S, Becker D, Clark L. Expert panel on detection, evaluation and treatment of high blood cholesterol in adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP III). JAMA. 2001;285(19):2486–97.
Shiffman D, Louie JZ, Caulfield MP, Nilsson PM, Devlin JJ, Melander O. LDL subfractions are associated with incident Cardiovascular Disease in the Malmö Prevention Project Study. Atherosclerosis. 2017;263:287–92.
Voight BF, Peloso GM, Orho-Melander M, Frikke-Schmidt R, Barbalic M, Jensen MK. Plasma HDL cholesterol and risk of Myocardial Infarction: a mendelian randomisation study. The Lancet. 2012;380(9841):572–80.
Hedayati M, Daneshpour MS, Zarkesh M, Yeganeh MZ, Sheikholeslami S, Faam B. etal.Biochemical assessment: findings from 20 years of the Tehran lipid and glucose study.Int J Endocrinol Metabolism.2018;16(4 Suppl).
Binno S. 2016EuropeanGuidelinesoncardiovasculardiseasepreventioninclinicalpractice–WebAddenda.2016.
Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice guidelines. J Am Coll Cardiol. 2014;63(25 Part B):2889–934.
Investigators M. Effect of simvastatin on coronary atheroma: the Multicentre Anti-atheroma Study (MAAS). The Lancet. 1994;344(8923):633–8.
Rosenson RS, Otvos JD, Freedman DS. Relations of lipoprotein subclass levels and low-density lipoprotein size to progression of coronary artery Disease in the Pravastatin limitation of Atherosclerosis in the coronary arteries (PLAC-I) trial. Am J Cardiol. 2002;90(2):89–94.
Hedayati M, Daneshpour M. Evaluation of HDL-C determination methods. Iran J Endocrinol Metabolism. 2005;7(4):365–73.
Sniderman AD. How, when, and why to use apolipoprotein B in clinical practice. Am J Cardiol. 2002;90(8):48–54.
Kwiterovich PO Jr. Clinical relevance of the biochemical, metabolic, and genetic factors that influence low-density lipoprotein heterogeneity. Am J Cardiol. 2002;90(8):30–47.
Dadu RT, Ballantyne CM. Lipid lowering with PCSK9 inhibitors. Nat Reviews Cardiol. 2014;11(10):563.
Navarese EP, Kołodziejczak M, Schulze V, Gurbel PA, Tantry U, Lin Y. Effects of proprotein convertase subtilisin/kexin type 9 antibodies in adults with hypercholesterolemia: a systematic review and meta-analysis. Ann Intern Med. 2015;163(1):40–51.
Kazi DS, Moran AE, Coxson PG, Penko J, Ollendorf DA, Pearson SD. Cost-effectiveness of PCSK9 inhibitor therapy in patients with heterozygous familial hypercholesterolemia or atherosclerotic Cardiovascular Disease. JAMA. 2016;316(7):743–53.
Wang TJ, Gona P, Larson MG, Tofler GH, Levy D, Newton-Cheh C. Multiple biomarkers for the prediction of first major cardiovascular events and death. N Engl J Med. 2006;355(25):2631–9.
Ware JH. The limitations of risk factors as prognostic tools. N engl J med. 2006;355(25):2615–7.
Krauss RM. Dense low density lipoproteins and coronary artery Disease. Am J Cardiol. 1995;75(6):53B–7B.
Krauss RM. Dietary and genetic effects on low-density lipoprotein heterogeneity. Annu Rev Nutr. 2001;21(1):283–95.
Ip S, Lichtenstein AH, Chung M, Lau J, Balk EM. Systematic review: association of low-density lipoprotein subfractions with cardiovascular outcomes. Ann Intern Med. 2009;150(7):474–84.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1–e34.
Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa: Ottawa Hospital Research Institute; 2011.
Hirayama S, Miida T. Small dense LDL: an emerging risk factor for Cardiovascular Disease. Clin Chim Acta. 2012;414:215–24.
Lakshmy R, Dorairaj P, Tarik M, Gupta R, Reddy KS. LDL particle heterogeneity, and its association with other established cardiovascular risk factors in a young Indian industrial population. Heart Asia. 2012;4(1):141–5.
Jug B, Papazian J, Lee R, Budoff MJ. Association of lipoprotein subfractions and coronary artery calcium in patient at intermediate cardiovascular risk. Am J Cardiol. 2013;111(2):213–8.
Shen MY, Chen FY, Hsu JF, Fu RH, Chang CM, Chang CT. Plasma L5 levels are elevated in ischemic Stroke patients and enhance platelet aggregation. Blood. 2016;127(10):1336–45.
Chu CS, Chan HC, Tsai MH, Stancel N, Lee HC, Cheng KH. Range of L5 LDL levels in healthy adults and L5’s predictive power in patients with hyperlipidemia or coronary artery Disease. Sci Rep. 2018;8(1):11866.
Pallarés-Carratalá V, Quesada JA, Orozco-Beltrán D, Amigó-Grau N, Lopez-Pineda A, Fernández Giménez A. Analysis of LDL and HDL size and number by nuclear magnetic resonance in a healthy working population: the LipoLab Study. Int J Clin Pract. 2021;75(1):e13610.
Notarnicola M, Tutino VDEN, et al. Integrated Small dense low-density Lipoprotein Profile in Cardiovascular Disease and Cancer: a longitudinal study. Anticancer Res. 2019;39(11):6035–9.
Llauradó G, Amigó N, Cano A, Ballesta S, Albert L, Mazarico I. etal.Specific nuclear magnetic resonance lipoprotein subclass profiles and central arterial stiffness in type 1 Diabetes Mellitus: a Case Control Study.J Clin Med.2019;8(11).
Steffen BT, Guan W, Remaley AT, Paramsothy P, Heckbert SR, McClelland RL. etal.Utility of lipoprotein particle measures for assessing coronary Heart Disease risk post-AHA/ACC guidelines: the multi-ethnic study of Atherosclerosis. Arteriosclerosis, Thrombosis, and vascular biology.2015;35(2):448.
Rizzo M, Pernice V, Frasheri A, Di Lorenzo G, Rini GB, Spinas GA. Small, dense low-density lipoproteins (LDL) are predictors of cardio- and cerebro-vascular events in subjects with the metabolic syndrome. Clin Endocrinol (Oxf). 2009;70(6):870–5.
Mora S, Otvos JD, Rifai N, Rosenson RS, Buring JE, Ridker PM. Lipoprotein particle profiles by nuclear magnetic resonance compared with standard lipids and apolipoproteins in predicting incident Cardiovascular Disease in women. Circulation. 2009;119(7):931–9.
Cure MC, Tufekci A, Cure E, Kirbas S, Ogullar S, Kirbas A. Low-density lipoprotein subfraction, carotid artery intima-media thickness, nitric oxide, and Tumor necrosis factor alpha are associated with newly diagnosed ischemic Stroke. Ann Indian Acad Neurol. 2013;16(4):498–503.
Zeljkovic A, Vekic J, Spasojevic-Kalimanovska V, Jelic-Ivanovic Z, Bogavac-Stanojevic N, Gulan B. LDL and HDL subclasses in acute ischemic Stroke: prediction of risk and short-term mortality. Atherosclerosis. 2010;210(2):548–54.
Aneni EC, Osondu CU, De La Cruz J, Martin SS, Blaha MJ, Younus A. Lipoprotein Sub-fractions by Ion-Mobility Analysis and Its Association with subclinical coronary Atherosclerosis in high-risk individuals. J Atheroscler Thromb. 2019;26(1):50–63.
Prado KB, Shugg S, Backstrand JR. Low-density lipoprotein particle number predicts coronary artery calcification in asymptomatic adults at intermediate risk of Cardiovascular Disease. J Clin Lipidol. 2011;5(5):408–13.
Chung CP, Oeser A, Raggi P, Sokka T, Pincus T, Solus JF. Lipoprotein subclasses determined by nuclear magnetic resonance spectroscopy and coronary Atherosclerosis in patients with rheumatoid arthritis. J Rheumatol. 2010;37(8):1633–8.
Amor AJ, Vinagre I, Valverde M, Urquizu X, Meler E, López E. etal.Nuclear magnetic resonance lipoproteins are associated with carotid Atherosclerosis in type 1 Diabetes and pre-eclampsia.Diab/Metab Res Rev.2020:e3362.
Duan R, Xue W, Wang K, Yin N, Hao H, Chu H. Estimation of the LDL subclasses in ischemic Stroke as a risk factor in a Chinese population. BMC Neurol. 2020;20(1):414.
Chang CY, Chen CH, Chen YM, Hsieh TY, Li JP, Shen MY. etal.Association between negatively charged low-density lipoprotein L5 and subclinical Atherosclerosis in rheumatoid arthritis patients.J Clin Med.2019;8(2).
Žitňanová I, Šiarnik P, Füllöp M, Oravec S, Penesová A, Ďuračková Z. Gender differences in LDL-and HDL-cholesterol subfractions in patients after the acute ischemic Stroke and their association with oxidative stress markers. J Clin Biochem Nutr. 2018;63(2):144–8.
Zhou M, Wang H, Zeng X, Yin P, Zhu J, Chen W. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: a systematic analysis for the global burden of Disease Study 2017. The Lancet. 2019;394(10204):1145–58.
Kwon SW, Yoon S-J, Kang TS, Kwon HM, Kim J-H, Rhee J. Significance of small dense low-density lipoprotein as a risk factor for coronary artery Disease and acute coronary syndrome. Yonsei Med J. 2006;47(3):405.
Superko HR, Gadesam RR. Is it LDL particle size or number that correlates with risk for Cardiovascular Disease? Curr Atheroscler Rep. 2008;10(5):377–85.
Chung M, Lichtenstein AH, Ip S, Lau J, Balk EM. Comparability of methods for LDL subfraction determination: a systematic review. Atherosclerosis. 2009;205(2):342–8.
Witte D, Taskinen MR, Perttunen-Nio H, van Tol A, Livingstone S, Colhoun H. Study of agreement between LDL size as measured by nuclear magnetic resonance and gradient gel electrophoresis. J Lipid Res. 2004;45(6):1069–76.
Oravec S, Gruber K, Dostal E, Mikl J. Hyper-betalipoproteinemia LDL 1, 2: a newly identified nonatherogenic hypercholesterolemia in a group of hypercholesterolemic subjects. Neuroendocrinol Lett. 2011;32(3):322–7.
Oravec S, Dukát A, Gavorník P, Lovásová Z, Gruber K. Atherogenic normolipidemia-a new phenomenon in the lipoprotein profile of clinically healthy subjects. Neuroendocrinol Lett. 2011;32(3):317–21.
Berneis KK, Krauss RM. Metabolic origins and clinical significance of LDL heterogeneity. J Lipid Res. 2002;43(9):1363–79.
Asztalos BF, Cupples LA, Demissie S, Horvath KV, Cox CE, Batista MC. etal.High-density lipoprotein subpopulation profile and coronary Heart Disease prevalence in male participants of the Framingham offspring study. Arteriosclerosis, Thrombosis, and vascular biology.2004;24(11):2181–7.
Oravec S, Dukat A, Gavornik P, Caprnda M, Kucera M, Ocadlik I. Contribution of the atherogenic lipoprotein profile to the development of arterial Hypertension. Bratisl Lek Listy. 2011;112(1):4–7.
Nigon F, Lesnik P, Rouis M, Chapman MJ. Discrete subspecies of human low density lipoproteins are heterogeneous in their interaction with the cellular LDL receptor. J Lipid Res. 1991;32(11):1741–53.
Maaninka K, Nguyen SD, Mäyränpää MI, Plihtari R, Rajamäki K, Lindsberg PJ. Human mast cell Neutral proteases generate modified LDL particles with increased proteoglycan binding. Atherosclerosis. 2018;275:390–9.
Gerber PA, Nikolic D, Rizzo M. Small, dense LDL: an update. Curr Opin Cardiol. 2017;32(4):454–9.
Atiq F, van de Wouw J, Sorop O, Heinonen I, de Maat MP, Merkus D. etal.Endothelial dysfunction, Atherosclerosis, and increase of Von Willebrand factor and factor VIII: a Randomized Controlled Trial in Swine.Thromb Haemost.2021.
Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk: the Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur Heart J. 2020;41(1):111–88.
Mihaylova B, Emberson J, Blackwell L, Keech A, Simes J, Barnes E. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular Disease: meta-analysis of individual data from 27 randomised trials. Lancet (London England). 2012;380(9841):581–90.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
ACh and MH conceived of the presented idea and developed the theory and performed the computations. MT and MH were encouraged to investigate and supervised the findings of this work. All authors discussed the results and contributed to the final manuscript. ACh wrote the manuscript with support from MT and MH.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chary, A., Tohidi, M. & Hedayati, M. Association of LDL-cholesterol subfractions with cardiovascular disorders: a systematic review. BMC Cardiovasc Disord 23, 533 (2023). https://doi.org/10.1186/s12872-023-03578-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-023-03578-0