
Abstract
Background
To investigate the incidence and influencing factors of acute gastrointestinal injury (AGI) after cardiac surgery.
Methods
A total of 346 cases receiving treatment in the Intensive Care Unit (ICU) of the Department of Cardiovascular Surgery in our hospital from January 2021 to December 2021 were enrolled and their basic information was collected, including age, gender, height, weight, past medical history, Nutrition Risk Screening 2002, Body Mass Index (BMI), total operation duration, stay in ICU, preoperative blood routine examination results, complete biochemical examination, diamine oxidase (DAO) on Day 1, D-lactic acid index, a postoperative gastrointestinal condition, other postoperative complications and death during hospitalization. Moreover, logistic regression analysis was performed to identify the independent risk factors influencing the incidence of AGI after cardiac surgery.
Results
The incidence and mortality of AGI after cardiac surgery were 10.40% (36/346) and 25% (9/36), respectively. A dichotomous logistic regression multivariate analysis revealed that DAO on Day 1 (odd ratio = 1.062, p = 0.006) and stay in ICU (odd ratio = 1.192, p < 0.001) were independent risk factors of AGI after cardiac surgery, and total protein is a protective factor (odd ratio = 0.914, p = 0.012).
Conclusions
Factors influencing AGI after cardiac surgery have been determined in this study. Our data suggest that patients with AGI after cardiac surgery have a decreased preoperative total protein, and elevated DAO on Day 1. Total protein and DAO on Day 1 were found to be correlated with AGI.
Similar content being viewed by others


Introduction
Gastrointestinal (GI) complications after cardiac surgery, although not the most common, need to be detected early because they are associated with high mortality rates. It has been demonstrated that the incidence and mortality of gastrointestinal complications after cardiac surgery are in the range of 1.21-4.17% [1,2,3,4] and 13.9-52%, respectively [5, 6]. Acute GI injury (AGI) is the malfunctioning of the GI tract in critically ill patients due to their acute illness [7]. The relationship between AGI or other gastrointestinal dysfunctions and the occurrence of gastrointestinal complications following cardiac surgery remains inadequately understood. Patients undergoing cardiac surgery are vulnerable to gastrointestinal dysfunction, primarily due to the diminished blood supply to the gastrointestinal tract resulting from surgical trauma.These disruptions can profoundly impact patient prognosis, underscoring the need for further research on this domain [8]. Therefore, the recovery of gastrointestinal function after cardiac surgery is essential to improve patients’ prognosis, and medical staff should take AGI seriously. In this study, a retrospective analysis of 346 cardiac surgery cases was performed to investigate the incidence of AGI and explore its influencing factors. Early intervention of the factors influencing AGI may improve the prognosis of patients who have undergone cardiac surgery.
Materials and methods
Demographic characteristics of the enrolled patients
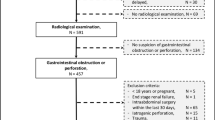
A total of 346 patients hospitalized in the Cardiac and Vascular Surgery Monitoring Unit of the First Affiliated Hospital of Soochow University from January 2021 to December 2021 were retrospectively selected and analyzed. These patients included 206 males and 140 females, with an average age of 56.07 ± 13.35 years old, The minimum age was 18 and the maximum age was 79. Inclusion criteria: At least 18 years old; no history of blood transfusion, albumin, or special nutritional support before admission; and complete clinical data. Exclusion criteria: age < 18 years old; history of blood transfusion, albumin, or special nutritional support before admission; and a history of gastrointestinal tumor or resection. The study was approved by the hospital’s ethics committee and all patients voluntarily participated and signed the informed consent form.
Monitoring and evaluation of gastrointestinal function
This study investigated cases of AGI, which manifested as nausea, vomiting, hypoactive bowel sounds, paralytic ileus, diarrhea, gastroparesis with gastric retention, gastrointestinal bleeding, abdominal distention, intestinal bleeding or perforation, and other symptoms. The AGI diagnostic criteria [7]: AGI level 1, with the risk of gastrointestinal dysfunction and failure; AGI level 2, gastrointestinal dysfunction; AGI level 3: gastrointestinal failure; AGI level 4, gastrointestinal failure with distant organ dysfunction. The diagnosis of AGI was based on the clinical characteristics and examination results.
Observation indicators
The records of the patient’s preoperative medical history included their age, gender, height, weight, BMI, Nutrition Risk Screening 2002, preoperative blood routine examination results, complete biochemical examination results, operation type, total operation duration, diamine oxidase (DAO) on Day 1, D-lactic acid index, stay in ICU and death during hospitalization.
Statistical method
Data were analyzed using SPSS 22.0 statistical analysis software. Measurement data were expressed as mean ± standard deviation (\(\stackrel{-}{x}\) ± s). Data not conforming to normal distribution were analyzed using a t-test, and data not conforming to normal distribution were analyzed by a non-parametric rank sum test. Count data were presented as cases (the percentage), and inter-group comparisons were performed using the χ2 test. Logistic binary regression analysis was performed to explore the factors influencing the incidence of AGI after cardiac surgery. p < 0.05 was considered statistically significant.
Results
General information
Among the 346 patients who underwent cardiac surgery, 206 were male and 140 were female. The average age was 56.07 ± 13.35 years old. Demographic data of the patients are presented in Table 1. Furthermore, 36 patients developed AGI during the hospitalization, with an incidence of 10.40% (36/346) and a mortality rate of 25% (9/36). This was higher than the 1.9% (6/310) mortality of non-AGI patients (p < 0.001, see Tables 1 and 2). There were 13 cases of septic shock and 171 cases of pulmonary infection after the operation, and 18 cases received CRRT treatment after the operation.
Univariate analysis of 346 cardiac surgery cases
AGI was detected in 36 out of 346 cases of cardiac surgery (incidence = 10.40%). AGI and non-AGI were consideted to be dependent variables in the influencing factor analysis. The univariate analysis showed that there were statistically significant differences between the two groups in terms of chronic kidney disease history, nutritional indicators (total protein, prealbumin, creatinine, red blood cells, lymphocytes, hemoglobin), intestinal barrier function indicators (DAO, D-lactate), operation type, operation duration, and stay in the ICU (p < 0.05, see Table 3).
Multivariate analysis of the incidence of AGI after cardiac surgery
A binominal logistic regression was performed on the factors with p < 0.05 in the univariate analysis as independent variables. For binary independent variables, the influencing factor was coded as 0 if it did not exist and 1 if it did. For the quantitative independent variables, we inputted the original values of the nutritional index, intestinal function index, total operation time, and stay in ICU. Additionally, dummy variables were set when the operation type was unordered multi-classification (Table 4). The dichotomous logistic stepwise regression analysis showed that total protein, DAO, and stay in ICU were significant independent factors for AGI (p < 0.05, Table 5)
Discussion
AGI after cardiac surgery is a rare complication with high mortality [3,4,5]
Gastrointestinal injuries are affected by various factors before and during cardiac surgery [9], with the major cause being splanchnic hypoperfusion [10]. In addition, systemic inflammation also contributes to the occurrence of GI complications [11]. Several nonischemic mechanisms may contribute to GI complications, including bacterial translocation, adverse drug reactions, and iatrogenic organ injury [8]. Preoperative hypertension, renal failure, chronic lung disease, and heart failure history have been identified as independent risk factors for acute mesenteric ischemia or postoperative gastrointestinal bleeding after cardiac surgery [9]. However, disease history was not found to be an independent risk factor in this study. Out of the 346 cases included in the study, the incidence of AGI after cardiac surgery was 10.4% (36/346), with a mortality of 25% (9/36). Dichotomous logistic regression showed that patients with higher preoperative total protein had lower risks of complications (OR = 0.914, 95%CI 0.852–0.980, p = 0.012). Total protein in the serum is a crucial indicator for monitoring nutritional status [12], and patients with extremely low levels of total protein have a low survival rate and increased risk of postoperative infection [13]. Preoperative nutritional status is a factor that significantly affects the prognosis of AGI. Malnutrition can cause systemic multiple-organ damage and renal insufficiency, which places an additional burden on the heart, leading to malignant circulation, prolonged stay in ICU, adversely affecting the prognosis, and even leading to death. Patients with a longer stay in ICU was associated with a higher risk of AGI after cardiac surgery (OR = 1.192, 95%CI 1.104–1.287, p < 0.001). One trial showed that providing various nutritional support measures can improve caloric deficiency and reduce mortality and complications in patients undergoing elective cardiac surgery [14].
DAO was an independent risk factor of the incidence of AGI after cardiac surgery (OR = 1.062, 95%CI 1.017–1.110, p = 0.006)
DAO is a highly active intracellular enzyme found in the cytoplasm of villus cells in the upper intestinal mucosa. When the intestinal mucosa is damaged, DAO is transported via the lymphatic and blood vessels in the intestinal intercellular space [15, 16]. Ye et al. [17] found that the level of DAO in the plasma was positively correlated with the degree of gastrointestinal dysfunction in critically ill children. Several studies [16, 18] have demonstrated that the D-lactate concentration in the blood is positively correlated with the severity of intestinal mucosal barrier damage, and early DAO specificity increases in patients with intestinal mucosal injury. Thus, elevated DAO in the serum is a sensitive indicator of intestinal mucosal barrier integrity. The DAO test is convenient for clinicians, is minimally traumatic for patients, and has a low cost. Therefore, the level of DAO can serve as a good indicator of the incidence of AGI after cardiac surgery. In addition to the function of digestion and absorption, the gastrointestinal tract also has the most important intestinal barrier function. Normal intestinal mucosa acts as a barrier that prevents entry of toxins and other substances, thus alleviating intestinal absorption. However, if gastrointestinal barrier function is damaged, it increased, and DAO increases. Additionally, changes in the intestinal microenvironment can cause intestinal flora disorder, resulting in the translocation of many intestinal bacteria and toxins, further exacerbating systemic inflammatory reactions [19]. Gastrointestinal failure can significantly increase mortality in severe cases [19, 20]. The mechanism underlying gastrointestinal barrier dysfunction in AGI after cardiac surgery may include the following: (1) Mechanical barrier dysfunction: is caused by the traction and compression of the heart during extracorporeal and non-extracorporeal circulation, leading to decreased gastrointestinal blood perfusion and ischemia-reperfusion injury. AGI is one of the clinical manifestations of ischemia-reperfusion injury [21]. (2) Chemical barrier dysfunction: is due to long-term fasting and total parenteral nutrition resulting in a decrease in gastric acid, bile, lysozyme, mucopolysaccharide, and other chemical components. (3) Biological barrier dysfunction: is caused by the long-term and massive use of broad-spectrum antibiotics, which leads to a reduction in the colonization of normal flora, an increase in pathogenic bacteria, and an increase in the permeability of the intestinal mucosa,compared with healthy individuals. Furthermore, the presence of a large amount of flora can disturb the internal environment and inhibit the immune system function [22]. (4) Immune barrier dysfunction: this is caused by shock, infection, trauma, and other factors, which damage the intestinal immune function and create potential niches for pathogenic bacteria. Furthermore, the integrity of regulatory cells can be damaged when the intestinal flora is disrupted [23].
Conclusion
The incidence of AGI after cardiac surgery is low but associated with a high rate of mortality. Close surveillance, prompt diagnosis, and adequate interdisciplinary treatment of AGI are important approaches for reducing mortality rates. Our data suggest that decreased preoperative total protein and elevated DAO on Day 1 are associated with the incidence of AGI after cardiac surgery. Understanding this relationship and referencing these data during the perioperative period may help optimize perioperative prevention and treatment strategies.
Data Availability
All data generated or analyzed during this study are included in this published article.
References
Vohra HA, Farid S, Bahrami T, Jullien A. Predictors of survival after gastrointestinal complications in bypass grafting. Asian Cardiovasc Thorac Ann. 2011;19(1):27–32.
Sever K, Ozbek C, Goktas B, Bas S, Ugurlucan M, Mansuroglu D. Gastrointestinal complications after open heart surgery: incidence and determinants of risk factors. Angiology. 2014;65(5):425–9.
Viana FF, Chen Y, Almeida AA, Afflu D, Wang Y, Thoma FW, et al. Gastrointestinal complications after cardiac surgery: 10-year experience of a single australian center. ANZ J Surg. 2013;83(9):651–6.
Chaudhry R, Zaki J, Wegner R, Afflu D, Wang Y, Thoma FW, et al. Gastrointestinal complications after cardiac surgery: a nationwide population-based analysis of morbidity and mortality predictors. J Cardiothorac Vasc Anesth. 2017;31(4):1268–74.
Rodriguez R, Robich MP, Plate JF, Deirmengian G, Courtney PM, Saxena A. Gastrointestinal complications following cardiac surgery: a comprehensive review. J Card Surg. 2010;25(2):188–97.
Elgharably H, Gamaleldin M, Ayyat KS, Zaki A, Hodges K, Kindzelski B, et al. Serious gastrointestinal complications after cardiac surgery and Associated Mortality. Ann Thorac Surg. 2021;112(4):1266–74.
Reintam Blaser A, Malbrain ML, Starkopf J, Fruhwald S, Jakob SM, De Waele J, et al. Gastrointestinal function in intensive care patients: terminology, definitions and management. Recommendations of the ESICM Working Group on abdominal problems. Intensive Care Med. 2012;38(3):384–94.
Sara J. Gastrointestinal complications and cardiac surgery. J Extra Corpor Technol. 2014;46(2):142–9.
Leon N, Ander Dorken G, Napaporn K, Kokoroskos N, Tolis G, Melnitchouk S, et al. Risk factors for ischemic gastrointestinal complications in patients undergoing open cardiac surgical procedures: a single-center retrospective experience. J Cardiac Surg. 2022;37(4):808–17.
Ohri SK, Velissaris T. Gastrointestinal dysfunction following cardiac surgery. Perfusion. 2006;21:215–23.
Chor CYT, Mahmood S, Khan IH, Shirke M, Harky A. Gastrointestinal complications following cardiac surgery. Asian Cardiovasc Thorac Ann. 2020;28(9):621–32.
Madhuvanthi M, Lathadevi GV. Serum proteins Alteration in Association with Body Mass Index in human volunteers. J Clin Diagn Res. 2016;10(6):CC05–7.
Chamogeorgakis T, Mason DP, Murthy SC, Thuita L, Raymond DP, Pettersson GB, et al. Impact of nutritional state on lung transplant outcomes. J Heart Lung Transplant. 2013;32(7):693–700.
De Waele E, Nguyen D, De Bondt K, La Meir M, Diltoer M, Honoré PM, et al. The CoCoS trial: caloric control in cardiac surgery patients promotes survival, an interventional trial with retrospective control. Clin Nutr. 2018;37(3):864–9.
Meng Y, Zhang Y, Liu M, Huang YK, Zhang J, Yao Q, et al. Evaluating intestinal permeability by measuring plasma endotoxin and diamine oxidase in children with acute lymphoblastic leukemia treated with high-dose methotrexate. Anticancer Agents Med Chem. 2016;16(3):387–92.
Schwelberger HG, Feurle J, Houen G. Mapping of the binding sites of human diamine oxidase (DAO) monoclonal antibodies. Inflanun Res. 2018;67(3):245–53.
Ye Y, Wang N, Tao W. Meta-analysis of the correlation of the changes of diamine oxidase with gastrointestinal dysfunction of critically ill patients. J Clin Med. 2019;6(4):30–2.
Kumar D, Pandey G, Bansal D, Rawat A, Kumar U, Dubey D, et al. NMR-based urinary profiling of lactulose/mannitol ratio used to assess the altered intestinal permeability in acute on chronic liver failure (ACLF) patients. Magn Reson Chem. 2017;55(4):289–96.
Shimizu K, Ogura H, Hamasaki T, Goto M, Tasaki O, Asahara T, et al. Altered gut flora are associated with septic complications and death in critically ill patients with systemic inflammatory response syndrome. Dig Dis Sci. 2011;56(4):1171–7.
Reintam Blaser A, Poeze M, Malbrain ML, Björck M, Oudemans-van Straaten HM, Starkopf J, et al. Gastrointestinal symptoms during the first week of intensive care are associated with poor outcome: a prospective multicenter study. Intensive Care Med. 2013;39(5):899–909.
Wu M, Yiang G, Liao W, Tsai AP, Cheng YL, Cheng PW, et al. Current mechanistic concepts in Ischemia and Reperfusion Injury. Cell Physiol Biochem. 2018;46(4):1650–67.
Spiljar M, Merkler D, Trajkovski M. The Immune System Bridges the gut microbiota with systemic energy homeostasis: focus on TLRs, Mucosal Barrier, and SCFAs. Front Immunol. 2017;8:1353.
Kerkhoff N, Bontkes HJ, Westers TM, de Gruijl TD, Kordasti S, van de Loosdrecht AA. Dendritic cells in myelodysplastic syndromes: from pathogenesis to immunotherapy. Immunotherapy. 2013;5(6):621–37.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
Ruolin Lu and Biwen Yang involved program 、thinking and Collected data.Ruolin Lu performed the data analysis with advice .Ruolin Lu wrote the manuscript. Biwen Yang revised the manuscript. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study protocol was reviewed and approved by Medical Ethics Committee of the First Affiliated Hospital of Soochow University, approval number: (2023) Ethical Review Approval No.069. Written informed consent was obtained from all the participants prior to the enrollment of this study. All methods were performed in accordance with the relevant guidelines and regulations (Declaration of Helsinki).
Consent for publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lu, R., Yang, B. Incidence and influencing factors of acute gastrointestinal injury after cardiac surgery. BMC Cardiovasc Disord 23, 437 (2023). https://doi.org/10.1186/s12872-023-03475-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-023-03475-6