
Abstract
Background
Mental stress-induced myocardial ischemia (MSIMI) frequently occurs in patients with coronary artery disease (CAD), and is even more common in patients with co-occurring CAD and depression/anxiety. MSIMI appears to be a poor prognostic factor for CAD, but existing data on depression/anxiety patients are limited.
Methods
This cohort study will consecutively screen 2,647 CAD patients between 2023 and 2025. Included subjects will need to have received coronary revascularization and also have depression and/or anxiety at baseline. This study will enroll 360 subjects who meet the criteria. Two mental stress tests will be carried out in each patient at 1 month and 1 year timelines after coronary revascularization, using Stroop color word tests. MSIMI will be assessed by 99 m−Tc-sestamibi myocardial perfusion imaging. The endothelial function will be assessed by EndoPAT. Furthermore, we will dynamically monitor patients’ health and mental conditions every 3 months. The mean follow-up time will be 1 year. The primary endpoint is the major adverse cardiac events, a composite of all-cause death, cardiac death, myocardial infarction, stroke, or unplanned revascularization. Secondary endpoints will include overall health and mental conditions. The reproducibility of mental stress combined with myocardial perfusion for detecting MSIMI and comparisons between coronary stenosis and ischemic segments will also be included.
Conclusions
This cohort study will provide information on MSIMI outcomes in CAD patients who also have comorbid depression/anxiety after revascularization. In addition, understanding the long-term dynamics of MSIMI and the match between coronary stenosis and ischemia will provide insight into MSIMI mechanisms.
Trail Registration
ChiCTR2200055792, 2022.1.20, www.medresman.org.cn;
Similar content being viewed by others


Background
Mental stress-induced myocardial ischemia (MSIMI) is increasingly recognized as a risk factor and a poor prognostic factor for coronary artery disease (CAD). The relationship between mental stress and myocardial ischemia was originally observed through controlled and objective experiments in 1976 [1]. Over the past 40 years, there has been increasing evidence that mental stress can evoke myocardial ischemia. MSIMI is defined as the imbalance between myocardial oxygen demand and supply during mental stress [2, 3]. MSIMI is common in CAD patients [4,5,6], and is also a prognostic factor for major adverse cardiovascular events (MACEs). Results from cohort studies have demonstrated that MSIMI is associated with double the risk for subsequent death or adverse cardiovascular events [7,8,9,10,11,12,13,14]. However, the data in high-risk patients (i.e., those with CAD and comorbid depression/anxiety) is limited.
However, no clinical studies on MSIMI have been conducted in patients with comorbid CAD and depression and/or anxiety. Psychological factors (such as depression and anxiety) have interactions with MSIMI in CAD patients. Both depression and anxiety are common psychological factors amongst CAD patients and have emerged as important risk factors for CAD [15]. They also increase the risk of MACEs in CAD patients [15, 16], even beyond the traditional risk factors [17]. Prior work has also found associations between psychological factors and MSIMI in both CAD and myocardial infarction patients [18, 19]. Moreover, the prevalence of MSIMI in patients with depression/anxiety and CAD was 22.08 times higher than in patients without depression/anxiety [20]. Thus, these results may enhance our understanding of the mechanisms underlying the association between MSIMI prognosis and future cardiovascular events in patients with depression and anxiety.
Additionally, long-term dynamic observations of MSIMI are lacking, and due to the overall variability of emotional factors, we speculate that MSIMI may also change over time. A small-sample clinical study using echocardiography to assess MSIMI with decreased ejection fraction found short-term (4 to 8 weeks) repeatability of psychological stress testing, but these findings still need to be replicated in a larger patient population [21].
Therefore, the aim of our study is to observe the dynamical impact of MSIMI on cardiovascular outcomes in a consecutive cohort of CAD patients with depression and/or anxiety who are receiving coronary revascularization and to dynamically observe long-term MSIMI changes. Our main hypothesis is that, amongst CAD patients with comorbid depression/anxiety, those with MSIMI will have higher incidences of MACEs than those without MSIMI.
Methods
The aim of this study is to dynamically observe the long-term effects of MSIMI on cardiovascular events in high-risk CAD patients combined with depression/anxiety. The mechanism of MSIMI will be further explored, including comparisons between coronary stenosis and myocardial perfusion, endothelial function as well as reproducibility of mental stress.
Study design and settings
This study is designed as a prospective, single-center, single-blinded cohort study and has been registered at www.medresman.org.cn (trial identifier: ChiCTR2200055792), following the STROBE guidelines [22]. All study processes will be performed at the Beijing Anzhen Hospital. The period of recruitment was from 2023 to 2025. We will have a median follow-up time of 1 year. Data collection will be completed within 1 week of each patients’ completion of the mental stress test. This research has been approved by the Beijing Anzhen Hospital Medical Ethics Committee (NO. 2019001), and all participants provided informed consent.
Participants
The study participants included adult patients with angiographically-confirmed CAD, including stable or unstable angina pectoris and myocardial infarction. All patients need to have received coronary revascularization procedures, including percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG). Before these procedures, we used the Patient Health Questionnaire-9 (PHQ-9) and Generalized Anxiety Disorder-7 (GAD-7) scores to screen for depression and/or anxiety. We used recommended cutoff scores (i.e., PHQ-9 > or = 5 and/or GAD-7 > or = 5) to diagnose the major depressive disorder and generalized anxiety disorder in CAD patients [23]. We also used the Seattle Anginal Questionnaire (SAQ) to assess patients’ health status.
The exclusion criteria were as follows: (1) patients who had acute coronary syndrome within 1 week; (2) patients with severe heart failure (NYHA ≥ III); (3) patients with uncontrolled hypertension (≥ 180/110mmHg); (4) patients with severe mental illness, except for severe depression; (5) patients with contraindications to nuclear medicine, such as active asthma; (6) dialysis patients; (7) patients with life expectancies less than 1 year, such as those with malignant tumor; (8) patients who were blind or were unable to read a single word of the 4 colors on the Stroop test. The complete inclusion and exclusion criteria are shown in Table 1.
Measures
Mental stress
Each participant will take two mental stress tests at 1 month and 1 year times points after coronary revascularization. The mental stress protocol includes the Stroop color word test (SCWT), which conflicts with the color and meaning. The SCWT is well-accepted and has good reproducibility amongst CAD patients [24]. The SCWT process has been detailed in previously published articles [25]. Both blood pressure (BP) and heart rate (HR) will be measured before SCWT and every 1 min after the test begins. After the test is completed, each patient will have 5 min to rest. Myocardial oxygen demand will be estimated by the rate-pressure product (RPP), which is defined as the peak HR multiplied by the maximum BP during the test. The test requires two trained operators to perform and record.
SPECT imaging procedures
MSIMI will be evaluated using 99 m−Tc-sestamibi gated Single Photon Emission Computed Tomography (SPECT) scans. The scanning and post-processing processes have been explained in detail in previous articles [25]. Tridimensional reconstruction of the left ventricle will be performed to assess ventricular function, in addition to analyzing ejection fraction (EF), end-diastolic volume (EDV), end-systolic volume (ESV), contractility, and myocardial thickness [24]. Four abnormal SPECT phenomena will be considered positive for MISIMI [26, 27], including reversable myocardial perfusion defects (RMPD), transient ischemic dilation (TID), reverse redistribution (RR), and EF reduction of ≥ 5% [28] (see Fig. 1). SPECT images will be analyzed by two experts who did not know the clinical conditions, and the controversial parts need to consult with a third expert to determine.

Four abnormal SPECT phenomena
(A) RMPD: The stress SPECT images show a reversible perfusion defect from the lateral wall apex to part of the middle of the posterior lateral wall. (B) TID: Rest EDV is 83ml and stress EDV is 102ml. The TID value is 1.27, which is likely to represent diffuse subendocardial ischemia or microvascular disease in the absence of epicardial coronary disease. (C) RR: The stress images show no perfusion defects, while the rest images show perfusion defects (including in the apical anterior segment of the left ventricle wall, the lateral apical segment, the posterior lateral wall mid-segment, and the basal segment). (D) EF decline ≥ 5%: Rest EF was 76%, and stress EF is declined to 62%; EF declined 14%
Comparison between coronary angiography and SPECT imaging
The mechanism underlying MSIMI is not clear, but microvascular dysfunction maybe one underlying factor [5]. However, a series of MSIMI studies found that the SPECT images of MSIMI and conventional stress-induced myocardial ischemia (CSIMI) did not match [29,30,31], but there were no studies that matched 17-segment MSIMI models and coronary angiographic vascular stenosis. Because all patients in this study received psychological stress SPECTs and coronary angiography, we can use their data to compare images to find the imaging-based characteristics of MSIMI.
Health and mental health conditions
CAD-related health conditions will be evaluated using the SAQ Questionnaire, which is one of the most widely used and frequently studied health status end points that exists within cardiovascular medicine [32]. Higher scores indicate better health status [33]. Mental status, which mainly included depression and anxiety in our study, will be assessed with the PHQ-9 and GAD-7 questionnaires at baseline and at each follow-up time point. The accuracy of the PHQ-9 and GAD-7 for screening depression and anxiety in CAD patients has been demonstrated across several previous studies [34,35,36]. Following previously-published suggestions [25], we defined the presence of depression or anxiety by a score of 5 points or higher. We will assess CAD-related health and mental status at baseline and at every follow-up time point after coronary revascularization.
Endothelial function test
Non-invasive detection of peripheral endothelial function tests will be used to assess the relationship between endothelial dysfunction and MSIMI. Endothelial function tests will be implemented before mental stress tests at baseline and follow-up time points. An EndoPAT 2000 Machine (Itamar Medical Ltd, Caesarea, Israel) [37] will be used to assess the reactive hyperemia index (RHI). Nitrates or any medications for erectile dysfunction will be discontinued 1 day before each patient’s endothelial function test. The test is performed by a trained physician.
Data collection
Data will be collected by a pre-designed Case Report Form. Data elements will include patients’ demographics, medical histories, SAQ questionnaires, depression and anxiety assessments, medical care records, medications, laboratory results, coronary angiography results, mental stress tests, SPECT imaging results, endothelial function tests, follow-up questionnaires, and clinical event documentations (Table 2).
Follow-Up
Patients will be followed up every 3 months after coronary revascularization with telephone calls or clinical visits for a mean follow-up of 1 year. SAQ, PHQ-9, and GAD-7 questionnaires will be used to assess health and mental status every 3 months. At 1 month and 1 year, patients will need to have a clinical visit to receive mental stress tests, SPECT imaging, and assessments of psychological and health status. At 1 year, patients will receive coronary angiography. At the 3, 6 and 9-month follow-up time points, patients will be contacted by phone call to assess psychological and health status, as well as study-related events. All patients will receive optimal medical therapy according to clinical practice guidelines.
Endpoints
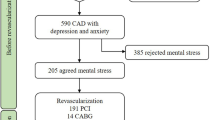
The primary will be the one-year difference rate of MACEs between patients with and without MSIMI. MACEs are defined as a composite of all-cause death, cardiac death, non-fatal MI, non-fatal stroke or any unplanned revascularization. Secondary endpoints will include health and mental status as well as changes in endothelial function in MSIMI. The reproducibility of mental stress combined with myocardial perfusion for detecting MSIMI will also be evaluated in this study. The study flowchart is displayed in Fig. 2.

Flowchart of the MSIMI Cohort Study in CAD Patients with comorbid Depression/anxiety after Coronary Revascularization
Statistics
The hypothesis of our prospective cohort study is that MSIMI will increase the rate of 1-year MACEs after coronary revascularization in patients with comorbid CAD and depression and/or anxiety. Sample size calculation is based on the primary endpoint. According to a previous systematic review and meta-analysis [7], we estimated that the presence of MSIMI would result in a MACEs rate at 1 year after coronary revascularization that is 2.24 times higher than patients without MSIMI (33.82% vs. 15.37%). According to our previous meta-analysis, compared with non-depressed people, the rate of MACEs in depressed patients is between 8.0 and 44.2%, the average rate is 28.7% [38]. Assuming a loss to follow-up rate of 5%, we calculated that 360 CAD patients after revascularization combined with derpression/anxiety would need to be enrolled in order to detect this expected difference with 85% power at the 5% significance level. According to our center’s statistics, the prevalence of depression and/or anxiety was 13.6% [39], these 360 CAD patients with depression/anxiety after revascularization need to be screened from 2,647 CAD patients. These findings were calculated with PASS 11.0.7 statistical software (NCSS, USA).
Continuous variables will be expressed as mean ± SD or median with corresponding IQR, and differences in continuous data will be compared by using Students t-tests or Mann-Whitney U tests as appropriate. Categorical variables will be expressed as frequency counts and will be compared by using chi-square tests or Fishers exact tests. The association between MSIMI and clinical measurements will be assessed with univariable and multivariable logistic regression. Kendall’s tau-b correlation coefficient test will be used to detect the consistency of MSIMI at baseline and follow-up time points. The impact of MSIMI alone at 1 month and 12 month after revascularization on MACEs at 12-month follow-up was compared by Kaplan–Meier curve survival analysis. To identify predictors, the influence of combined MSIMI, mental status and endothelial function on MACEs will be analysed by Cox proportional hazards regression models. A value of P < 0.05 was considered statistically significant. Statistical analyses will be performed using IBM SPSS Statistics 22.0.
Discussion
Our cohort study will be the first clinical trial to attempt to explore the prognosis of MSIMI in high-risk CAD patients with comorbid depression and/or anxiety following coronary revascularization. The major strengths and features of our study include: (1) a large sample size of consecutive CAD patients with depression and/or anxiety; (2) the ability to verify the reproducibility of MSIMI and its long-term impacts on MACEs; and (3) the ability to examine comprehensive myocardial perfusion and coronary angiography during times of psychological stress.
The American Heart Association recommends that all CAD patients be screened for depression because of its incidence and association with poor prognosis [39]. Additionally, standardized screening pathways for early identification of depression have been shown to improve outcomes [40]. Anxiety is also common in CAD and is confirmed to be associated with MACE events, but the relationship is not as strong as the relationship with depression [15, 16, 41]. Additionally, compared to CAD patients without depression or anxiety, the prevalence of MSIMI has been shown to be 22.08 times higher in CAD patients with depression and/or anxiety [20]. However, the characteristics of MSIMI in CAD with depression/anxiety and the prognostic outcomes are still not well-understood. Thus, we will screen CAD patients for depression and anxiety based on AHA recommendations to determine the characteristics and prognosis of these high-risk patients via long-term follow-up of mental status, MSIMI, and MACE events.
While previous MSIMI cohort studies on prognosis only performed only one mental stress test at baseline [7, 13], our study will dynamically observe changes in MSIMI with two mental stress tests, both at baseline and follow-up. At the same time, according to the results of two psychological stress tests, the patients were divided into four groups: MSIMI negative group, MSIMI positive group, MSIMI trans-negative group and MSIMI trans-positive group, and the differences in the occurrence of MACE events among the four groups were observed.
Few previous studies have investigated MSIMI reproducibility. Most studies have included only one mental stress test [4, 6, 7, 11, 13, 14]. In a recent study [42], 12 of 16 (75%) CAD patients showed repeated MSIMI by radionuclide ventriculography at an approximately 2-week interval. Additionally, the 3 CAD patients who did not exhibit mental stress-induced ischemia also did not exhibit ischemia with repeated mental stress testing. The PIMI study [43] compared the two standardized mental stress tests (a timed SCWT and a public speaking task) in a nuclear cardiology laboratory before and after 2–8 weeks. 68% and 60% of the patients had consistent scores on the Stroop test and speech test, respectively, which was considered modestly reproducible. However, neither study lasted longer than 2 months. The results of our study will examine long-term reproducibility over the course of 12 months and will link the findings with MACE events.
Most previous studies have shown no correlation between coronary angiographic stenosis and the occurrence of MSIMI [31, 44], and it has been speculated that MSIMI is driven by alternative mechanisms, such as endothelial and microvascular dysfunction [5]. However, these studies did not simultaneously perform coronary angiography and SPECT imaging after mental stress, meaning it was impossible to understand the relationship between coronary stenosis and MSIMI segments. Therefore, our study design will include patients with coronary angiography and revascularization, and will thus be able to compare whether the blood vessels corresponding to ischemic MSIMI segments are related to stenosis or revascularization.
One limitation of our study is that we did not assess CSIMI, so we could not simultaneously obtain coronary flow reserve (CFR) data or perform adenosine stress testing. In the pre-experimental phase, we tried to measure CFR during mental stress tests in 5 patients. However, all patients had CFR values less than 2.0, so we considered mental stress to be less intense than adenosine. Thus, we were unable to assess microvascular dysfunction based on CFR in this population. We will consider correcting this oversight in future research.
Conclusion
Our MSIMI study is a prospective, single-center, single-blinded cohort study that will assess MSIMI in CAD patients with comorbid depression and/or anxiety after revascularization. Our hypothesis is that MSIMI will enhance the rate of 1-year MACE events. The study will also provide evidence for the long-term dynamics of mental stress with 99 m−Tc-sestamibi SPECT imaging, as well as the interpretation of imaging mechanisms by contrasting coronary angiography with stenotic coronary arteries and SPECT ischemic segments.
Data availability
Not applicable.
Abbreviations
- MSIMI:
-
Mental stress-induced myocardial ischemia
- CAD:
-
Coronary artery disease
- MACEs:
-
Major adverse cardiovascular events
- PCI:
-
Percutaneous coronary intervention
- CABG:
-
Coronary artery bypass grafting
- PHQ-9:
-
Patient Health Questionnaire-9
- GAD-7:
-
Generalized Anxiety Disorder-7
- SAQ:
-
Seattle Anginal Questionnaire
- SCWT:
-
Stroop color word test
- BP:
-
Blood Pressure
- HR:
-
Heart rate
- RPP:
-
rate-pressure product
- SPECT:
-
Single Photon Emission Computed Tomography
- EF:
-
Ejection fraction
- EDV:
-
End-diastolic volume
- ESV:
-
End-systolic volume
- RMPD:
-
Reversable myocardial perfusion defects
- TID:
-
Transient ischemic dilation
- RR:
-
Reverse redistribution
- CSIMI:
-
Conventional stress-induced myocardial ischemia
- RHI:
-
Reactive hyperemia index
- CFR:
-
Coronary flow reserve
References
Schiffer F, Hartley LH, Schulman CL, Abelmann WH. The quiz electrocardiogram: a new diagnostic and research technique for evaluating the relation between emotional stress and ischemic heart disease. Am J Cardiol. 1976;37(1):41–7.
Strike PC, Steptoe A. Systematic review of mental stress-induced myocardial ischaemia. Eur Heart J. 2003;24(8):690–703.
Zhang L, Bao Y, Wang X, Zhou Y, Tao S, Xu W, et al. A meta-analysis on the prevalence, associated factors and diagnostic methods of mental stress induced myocardial ischemia. J translational Med. 2020;18(1):218.
Jiang W, Samad Z, Boyle S, Becker RC, Williams R, Kuhn C, et al. Prevalence and clinical characteristics of mental stress-induced myocardial ischemia in patients with coronary heart disease. J Am Coll Cardiol. 2013;61(7):714–22.
Arri SS, Ryan M, Redwood SR, Marber MS. Mental stress-induced myocardial ischaemia. Heart. 2016;102(6):472–80.
Krantz DS, Sheps DS, Carney RM, Natelson BH. Effects of mental stress in patients with coronary artery disease: evidence and clinical implications. JAMA. 2000;283(14):1800–2.
Wei J, Rooks C, Ramadan R, Shah AJ, Bremner JD, Quyyumi AA, et al. Meta-analysis of mental stress-induced myocardial ischemia and subsequent cardiac events in patients with coronary artery disease. Am J Cardiol. 2014;114(2):187–92.
Jain D, Burg M, Soufer R, Zaret BL. Prognostic implications of mental stress-induced silent left ventricular dysfunction in patients with stable angina pectoris. Am J Cardiol. 1995;76(1):31–5.
Jiang W, Babyak M, Krantz DS, Waugh RA, Coleman RE, Hanson MM, et al. Mental stress–induced myocardial ischemia and cardiac events. JAMA. 1996;275(21):1651–6.
Krantz DS, Santiago HT, Kop WJ, Bairey Merz CN, Rozanski A, Gottdiener JS. Prognostic value of mental stress testing in coronary artery disease. Am J Cardiol. 1999;84(11):1292–7.
Sheps DS, McMahon RP, Becker L, Carney RM, Freedland KE, Cohen JD, et al. Mental stress-induced ischemia and all-cause mortality in patients with coronary artery disease: results from the Psychophysiological Investigations of myocardial ischemia study. Circulation. 2002;105(15):1780–4.
Babyak MA, Blumenthal JA, Hinderliter A, Hoffman B, Waugh RA, Coleman RE, et al. Prognosis after change in left ventricular ejection fraction during mental stress testing in patients with stable coronary artery disease. Am J Cardiol. 2010;105(1):25–8.
Vaccarino V, Almuwaqqat Z, Kim JH, Hammadah M, Shah AJ, Ko YA, et al. Association of Mental Stress-Induced Myocardial Ischemia with Cardiovascular events in patients with Coronary Heart Disease. JAMA. 2021;326(18):1818–28.
Alenezi F, Brummett BH, Boyle SH, Samad Z, Babyak MA, Alzaeim N, et al. Usefulness of myocardial annular velocity change during Mental stress to Predict Cardiovascular Outcome in patients with coronary artery disease (from the responses of Mental Stress-Induced myocardial ischemia to Escitalopram Treatment Trial). Am J Cardiol. 2017;120(9):1495–500.
Allgulander C. Anxiety as a risk factor in cardiovascular disease. Curr Opin Psychiatry. 2016;29(1):13–7.
Frasure-Smith N, Lesperance F. Depression and anxiety as predictors of 2-year cardiac events in patients with stable coronary artery disease. Arch Gen Psychiatry. 2008;65(1):62–71.
May HT, Horne BD, Knight S, Knowlton KU, Bair TL, Lappe DL, et al. The association of depression at any time to the risk of death following coronary artery disease diagnosis. Eur heart J Qual care Clin outcomes. 2017;3(4):296–302.
Boyle SH, Samad Z, Becker RC, Williams R, Kuhn C, Ortel TL, et al. Depressive symptoms and mental stress-induced myocardial ischemia in patients with coronary heart disease. Psychosom Med. 2013;75(9):822–31.
Wei J, Pimple P, Shah AJ, Rooks C, Bremner JD, Nye JA, et al. Depressive symptoms are associated with mental stress-induced myocardial ischemia after acute myocardial infarction. PLoS ONE. 2014;9(7):e102986.
Zhang LJ, He DF, Yang Y, Pu LH, Xu LY, Zhou YX, et al. [A clinical study of mental stress-induced myocardial ischemia in patients with stable coronary artery disease and depression/anxiety]. Zhonghua nei ke za zhi. 2018;57(7):494–9.
Jain D, Joska T, Lee FA, Burg M, Lampert R, Zaret BL. Day-to-day reproducibility of mental stress-induced abnormal left ventricular function response in patients with coronary artery disease and its relationship to autonomic activation. J nuclear cardiology: official publication Am Soc Nuclear Cardiol. 2001;8(3):347–55.
von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, et al. The strengthening the reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–7.
Stafford L, Berk M, Jackson HJ. Validity of the hospital anxiety and Depression Scale and Patient Health Questionnaire-9 to screen for depression in patients with coronary artery disease. Gen Hosp Psychiatry. 2007;29(5):417–24.
Barbirato GB, Felix R, de Azevedo JC, Correa PL, de Nobrega AC, Coimbra A, et al. Prevalence of induced ischemia by mental distress. Arquivos brasileiros de cardiologia. 2010;94(3):301–7. 21 – 7.
Nan N, Dong W, Gao B, Cui F, Chang Z, Jiao J, et al. Association between quality of life and mental stress-induced myocardial ischaemia in high-risk patients after coronary revascularization. Health Qual Life Outcomes. 2022;20(1):69.
Dorbala S, Ananthasubramaniam K, Armstrong IS, Chareonthaitawee P, DePuey EG, Einstein AJ, et al. Single Photon Emission Computed Tomography (SPECT) Myocardial Perfusion Imaging Guidelines: Instrumentation, Acquisition, Processing, and interpretation. J nuclear cardiology: official publication Am Soc Nuclear Cardiol. 2018;25(5):1784–846.
Becker LC, Pepine CJ, Bonsall R, Cohen JD, Goldberg AD, Coghlan C, et al. Left ventricular, peripheral vascular, and neurohumoral responses to mental stress in normal middle-aged men and women. Reference group for the Psychophysiological Investigations of myocardial ischemia (PIMI) Study. Circulation. 1996;94(11):2768–77.
Jiang W. Emotional triggering of cardiac dysfunction: the present and future. Curr Cardiol Rep. 2015;17(10):91.
Vaccarino V, Wilmot K, Al Mheid I, Ramadan R, Pimple P, Shah AJ et al. Sex Differences in Mental Stress-Induced Myocardial Ischemia in Patients With Coronary Heart Disease. J Am Heart Association. 2016;5(9).
Pimple P, Hammadah M, Wilmot K, Ramadan R, Al Mheid I, Levantsevych O, et al. Chest Pain and Mental Stress-Induced myocardial ischemia: sex differences. Am J Med. 2018;131(5):540–7e1.
Hammadah M, Al Mheid I, Wilmot K, Ramadan R, Shah AJ, Sun Y, et al. The Mental stress ischemia prognosis study: objectives, Study Design, and prevalence of Inducible Ischemia. Psychosom Med. 2017;79(3):311–7.
Kirtane AJ. The importance of listening to patients: the Seattle Angina Questionnaire. JAMA Cardiol. 2018;3(11):1037.
Spertus JA, Winder JA, Dewhurst TA, Deyo RA, Prodzinski J, McDonell M, et al. Development and evaluation of the Seattle Angina Questionnaire: a new functional status measure for coronary artery disease. J Am Coll Cardiol. 1995;25(2):333–41.
van der Zwaan GL, van Dijk SEM, Adriaanse MC, van Marwijk HWJ, van Tulder MW, Pols AD, et al. Diagnostic accuracy of the Patient Health Questionnaire-9 for assessment of depression in type II diabetes mellitus and/or coronary heart disease in primary care. J Affect Disord. 2016;190:68–74.
Hayek SS, Ko YA, Awad M, Del Mar Soto A, Ahmed H, Patel K, et al. Depression and chest pain in patients with coronary artery disease. Int J Cardiol. 2017;230:420–6.
Morys JM, Bellwon J, Adamczyk K, Gruchala M. Depression and anxiety in patients with coronary artery disease, measured by means of self-report measures and clinician-rated instrument. Kardiologia Polska. 2016;74(1):53–60.
Axtell AL, Gomari FA, Cooke JP. Assessing endothelial vasodilator function with the Endo-PAT 2000. J visualized experiments: JoVE. 2010(44).
Zhang WY, Nan N, Song XT, Tian JF, Yang XY. Impact of depression on clinical outcomes following percutaneous coronary intervention: a systematic review and meta-analysis. BMJ open. 2019;9(8):e026445.
Zhang WY, Nan N, He Y, Zuo HJ, Song XT, Zhang M et al. Prevalence of depression and anxiety symptoms and their associations with cardiovascular risk factors in coronary patients. Psychol health Med. 2022:1–13.
Lichtman JH, Bigger JT Jr, Blumenthal JA, Frasure-Smith N, Kaufmann PG, Lesperance F, et al. Depression and coronary heart disease: recommendations for screening, referral, and treatment: a science advisory from the American Heart Association Prevention Committee of the Council on Cardiovascular nursing, Council on Clinical Cardiology, Council on Epidemiology and Prevention, and Interdisciplinary Council on Quality of Care and Outcomes Research: endorsed by the american Psychiatric Association. Circulation. 2008;118(17):1768–75.
Celano CM, Millstein RA, Bedoya CA, Healy BC, Roest AM, Huffman JC. Association between anxiety and mortality in patients with coronary artery disease: a meta-analysis. Am Heart J. 2015;170(6):1105–15.
Kim CK, Bartholomew BA, Mastin ST, Taasan VC, Carson KM, Sheps DS. Detection and reproducibility of mental stress-induced myocardial ischemia with Tc-99m sestamibi SPECT in normal and coronary artery disease populations. J nuclear cardiology: official publication Am Soc Nuclear Cardiol. 2003;10(1):56–62.
Carney RM, McMahon RP, Freedland KE, Becker L, Krantz DS, Proschan MA, et al. Reproducibility of mental stress-induced myocardial ischemia in the Psychophysiological Investigations of myocardial ischemia (PIMI). Psychosom Med. 1998;60(1):64–70.
Almuwaqqat Z, Sullivan S, Hammadah M, Lima BB, Shah AJ, Abdelhadi N, et al. Sex-specific Association between Coronary Artery Disease Severity and Myocardial Ischemia Induced by Mental stress. Psychosom Med. 2019;81(1):57–66.
Acknowledgements
The authors would like to thank Bin Li and Kun Lin from Health Biotech CO., Ltd for their EndoPAT2000 machine free of charge to test endothelial dysfunction.
Funding
This study was supported by theproject of China International Medical Foundation (Grant 2022-N-01-01), Beijing Lab for Cardiovascular Precision Medicine (Grant PXM2020_014226_000017_00377132_FCG) and Beijing Engineering Research Center of Cardiovascular Wisdom Diagnosis and Treatment.
Author information
Authors and Affiliations
Contributions
SXT and ZHJ: Concept, study design and manuscript revision. ZHJ: Definition of intellectual content and departmental cooperation. NN: Data collection, analysis and interpretation, manuscript drafting and revision. FL and WG: Psychological stress test design and data analysis. DW and MHZ: Study design of Nuclear Medicine section, image acquisition and image data analysis. GBY: Data acquisition and data analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no competing interests
Ethics approval and consent to participate
All study processes will be performed at the Beijing Anzhen Hospital. The period of recruitment was from 2023 to 2025. We will have a median follow-up time of 1 year. This research has been approved by the Beijing Anzhen Hospital Medical Ethics Committee (NO. 2019001) in accordance with the Declaration of Helsinki and all methods were performed in accordance with the relevant guidelines and regulations, and all participants provided informed consent.
Consent for publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Nan, N., Feng, L., Dong, W. et al. The prognostic study of mental stress-induced myocardial ischemia in coronary revascularization patients with depression/anxiety: rationale and design. BMC Cardiovasc Disord 23, 235 (2023). https://doi.org/10.1186/s12872-023-03246-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-023-03246-3