
Abstract
Objective
To investigate the possible association between AT1R gene polymorphisms and major adverse cardiovascular and cerebrovascular events (MACCEs) in hypertension patients combined with or without coronary artery disease (CAD) in Xinjiang.
Methods
374 CAD patients and 341 non-CAD individuals were enrolled as study participants and all of them have a hypertension diagnosis. AT1R gene polymorphisms were genotyped by SNPscan™ typing assays. During the follow-up in the clinic or by telephone interview, MACCEs were recorded. Kaplan–Meier curves and Cox survival analyses were used to explore the association between AT1R gene polymorphisms and the occurrence of MACCEs.
Results
AT1R gene rs389566 was associated with MACCEs. The TT genotype of the AT1R gene rs389566 had a significantly higher probability of MACCEs than the AA + AT genotype (75.2% vs. 24.8%, P = 0.033). Older age (OR = 1.028, 95% CI: 1.009–1.0047, P = 0.003) and TT genotype of rs389566 (OR = 1.770, 95% CI: 1.148–2.729, P = 0.01) were risk factors of MACCEs. AT1R gene rs389566 TT genotype may be a predisposing factor for the occurrence of MACCEs in hypertensive patients.
Conclusion
We should also pay more attention to the prevent of MACCEs in hypertension patients combined with CAD. Especially those elderly hypertensive patients carrying AT1R rs389566 TT genotype requires avoidance of unhealthy lifestyle, better management of blood pressure control and reduce the occurrence of MACCEs.
Similar content being viewed by others


Introduction
Coronary artery disease (CAD) and hypertensive are common diseases that endanger human health. As blood pressure regulatory system in the body, the renin-angiotensin system (RAS) is an important risk factors for CAD [1]. The angiotensin II (Ang II) type 1 receptor (AT1R) is involved in the classical physiological actions of Ang II, and plays a pivotal role in the pathogenesis of atherosclerosis in human [2].
Hypertension is a major risk factor for CAD and 25% of patients with CAD have hypertension [3, 4]. CAD is the first cause of morbidity and mortality in hypertension [5]. As referred above, AT1R is very important for the CAD, but its roles in pathogenesis of hypertension patients combined with CAD remains to be understood, although the associations between the AT1R polymorphisms, CAD and hypertension had been proved in French and English Caucasians population respectively [6, 7].
This study sequenced two single nucleotide polymorphisms (SNPs) of AT1R gene in all patients, and the differences in the distribution frequencies of these SNPs were compared between CAD patients and non-CAD patients combined with hypertension, and the association between AT1R gene polymorphisms and major adverse cardiovascular and cerebrovascular events (MACCEs) were analyzed.
Materials and methods
Study Population
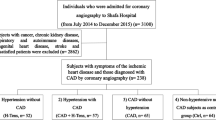
In this case-control study, we recruited adult hypertension patients combined with CAD or non-CAD who were long-term residents of the Xinjiang region, China, and they were admitted to the Heart Center of the First Affiliated Hospital of the Xinjiang Medical University with symptoms of chest tightness or precordial discomfort during 2010–2018. Each subject signed an informed consent before participating in this study. Inclusion criteria: Guidelines for the diagnosis of hypertension [8]. Hypertension was defined as systolic blood pressure (SBP) above 140 mmHg or diastolic blood pressure (DBP) above 90 mmHg, having previously been diagnosed by a physician or taking antihypertensive drugs [9]. Exclusion criteria: patients with incomplete data and complicated with one or more than one disease, such as secondary hypertension, valvular heart disease, rheumatic heart disease, heart failure but no hypertension, congenital heart disease, systemic immune system diseases, and multiple organ failure.
General data collection
The medical record system of our hospital was consulted according to the name and hospitalization certificate number, and the required data were collected according to the inclusion criteria, and data entry was performed using an Excel sheet. General data were collected including gender, age, body mass index (BMI), hypertension, type 2 diabetes mellitus (T2DM), Although people over the age of 50 used to smoke and drink, they have stopped smoking and drinking. Considering that smoking and drinking have caused damage to the vascular endothelium, this part of the population is still considered to have a history of smoking and drinking [10], family history of CAD, etc. Laboratory tests for blood glucose, lipids including cholesterol, triglycerides, high density lipoprotein cholesterol (HDL-c) and low-density lipoprotein cholesterol (LDL-c) were also collected.
Diagnostic of MACCEs, CAD and Hypertension
MACCEs were considered as the endpoints, including cardiac and noncardiac death, nonfatal acute myocardial infarction, unplanned revascularization (new percutaneous coronary intervention or bypass cardiac surgery), malignant arrhythmia, development of congestive heart failure, and stroke. Cardiovascular events were defined according to the guidelines of the European Society of Cardiology (ESC) and the standardized definition of vascular and stroke endpoint events in the Clinical Data Interchange Standards Consortium (CDISC) clinical trial center [11, 12]. Typical symptom of CAD is exertional angina, with pressure pain in the precordial region during activity or emotional stress. It can radiate to the left shoulder or/and left upper arm for 5–10 min and can be relieved by rest or medications such as nitroglycerin. Diagnosis CAD is based on symptoms, signs and ancillary tests such as electrocardiography and coronary angiography (CAG). CAG is the gold standard for diagnosing CAD. Diagnosis of CAD should be at least one coronary arterial stenosis of 50% or its major branches in the CAG [13]. According to the Treatment of hypertension: The ESH/ESC guidelines recommendations [8], hypertension is diagnosed under the following conditions: systolic blood pressure (SBP) ≥ 140mmHg and / or diastolic blood pressure (DBP) ≥ 90mmHg on three different days in the absence of antihypertensive drugs; patients with a history of hypertension and currently taking antihypertensive drugs although their blood pressures were lower than 140 / 90mmHg.
Genotyping assay
The same genotyping and unified standard biochemical tests were applied to all subjects. Two SNPs (rs389566 and rs1680760) of the AT1R gene whose minor allele frequencies (MAF) are more than 5% were selected from the HapMap human SNP database (www.hapmap.org). We also found that the above two SNPs were the tagging SNP of the Chinese Xinxiang hypertension population (MAF ≥ 5% and with R2 ≥ 0.8 as a cut-off in linkage disequilibrium pattern analysis) in the HapMap [14]. A total of 5 mL of fasting peripheral venous blood was drawn from the subjects into ethylenediaminetetraacetic acid (EDTA)-containing blood collection tubes, and plasma and blood cells were separated through centrifugation and stored in a − 80 °C refrigerator until further use. Plasma was were measured by biochemical indicator and blood cells were subjected to genomic DNA extraction using a whole blood genome extraction kit (Tiangen Biotech, China). AT1R gene polymorphism was detected by TaqMan® SNP genotyping qRT PCR. Genotyping accuracy was determined by genotypic concordance between replicate samples, and the accuracy of each SNP was 100%. The reaction system of qPCR amplification was composed of following reagents: 3 µL of TaqMan Universal Master Mix, 0.12 µL probes and 1.88 µL ddH2O in a 6 µL final reaction volume containing 50 ng DNA. Amplification cycling conditions were as follows: 95 °C for 5 min; 35 cycles of 95 °C for 15 s and 60 °C for 1 min.
Statistical methods
SPSS 26.0 statistical software was used for statistical analysis. T-test was used for comparison between groups; χ chi-square test was used for comparison of count data. Cox regression was used for multi-factor analysis. The associations between patients’ survival rate and the AT1R gene polymorphism were evaluated using Kaplan–Meier analysis. A difference was considered statistically significant as P < 0.05 (two-sided).
Results
General clinical characteristics
In this study, we compared the general characteristics of patients between non-CAD and CAD patients combined with hypertension. We found that CAD patients tended to be older (55.7 ± 9.7 vs. 59.6 ± 10.7 years, P < 0.001), higher glucose levels of BMI (26.93 ± 3.85 vs. 26.07 ± 3.10 kg/m2, P = 0.030), SBP (132 ± 17 vs. 129 ± 18 mmHg, P = 0.023), DBP (80 ± 11 vs. 78 ± 12 mmHg, P = 0.043) compared with non-CAD patients. Patients with CAD also have higher levels of TC (4.17 ± 1.01 vs. 4.45 ± 1.18 mmol/L, P = 0.001), LDL-c (2.60 ± 0.83 vs. 2.76 ± 0.96 mmol/L, P = 0.010) and lower HDL-c (1.04 ± 0.29 vs. 0.99 ± 0.28 mmol/L, P = 0.020, Table 1).
General characteristics and biochemical parameters between control (non-MACCEs) and MACCEs groups had been compared, as shown in Table 2. There was no significant difference regarding gender, smoking, alcohol intake, T2DM between these groups (P > 0.05). The prevalence of MACCEs in CAD patients was significantly higher than non-CAD patients (79.5% vs. 20.5%), P < 0.001. Patients with MACCEs showed higher blood glucose compared with those non-MACCEs patients (8.15 ± 3.42 vs. 6.93 ± 3.22 mmol/L), P < 0.001.
Patients with MACCEs showed higher age (Table 2) compared with those non-MACCEs patients (57.1 ± 10.3 vs. 59.1 ± 9.7 years), P < 0.001. We then compared characteristics among different age groups in Table 3. In 51–60 years old and over 60 years old groups, MACCEs occurrence increased significantly (31.6% and 54.7%, respectively, P = 0.001). The BMI, blood pressure, glucose, TG, HDL-c showed significantly difference among different age groups (P < 0.05). There was no difference regarding rs16860760, rs389566 TT genotype among different age groups (P = 0.932, P = 0.446 respectively).
Occurrence of MACCEs in patients with different genotypes of rs16860760 in AT1R gene
There was no significant difference regarding the frequency of MACCEs in different AT1R rs16860760 SNPs (P > 0.05), but the AT1R gene rs389566 polymorphism showed significant association with the probability of MACCEs in patients with hypertension (Table 4). And the patients carrying TT genotype at rs389566 locus had a higher risk of MACCEs than those carrying the AA + AT gene type (24.8% vs. 75.2%, P = 0.033).
Risk factors of MACCEs
In the present study, the mean follow-up duration was 65.6 (38.3, 91.8) months. The Kaplan–Meier analysis revealed that the MACCEs-free cumulative survival rate in the TT genotype group was obviously lower than that in the AA + AT genotype group (P = 0.009, Fig. 1).

Kaplan-Meier curves of MACCEs survival analysis according to the rs389566 genotype
Through univariate Cox survival analysis, we found that elderly, glucose, coronary artery disease, and rs389566 TT gene types may be risk factors for MACCEs in patients with hypertension. As shown in Table 5 and Fig. 2, age, AT1R gene rs389566 TT genotype, CAD and glucose variables were included to construct a multifactorial Cox proportional risk model. The results showed old age may be a predisposing factor on the occurrence of MACCEs (OR = 1.028, 95% CI: 1.009–1.047, P = 0.003), and rs389566 TT genotype may be a predisposing factor on the occurrence of MACCEs (OR = 1.770, 95%CI 1.148–2.729, P = 0.010).Patients with CAD were prone to MACCEs (OR = 4.118, 95%CI 2.542–6.672, P < 0.001). However, the glucose showed no significant different effect on occurrence of MACCEs in the final model (P > 0.05).

Cox regression analysis of the forest plot of MACCEs risk factors in hypertensive patients
Discussion
Many factors influence the occurrence of MACCEs, such as family history of CAD, smoking, obesity, hypertension, diabetes, abnormal lipid metabolism, insulin resistance, and homocysteine mia [15]. In the present study, AT1R gene rs389566 TT genotype was found to be associated with the occurrence of MACCEs in hypertension patients.
Cardiovascular disease is the leading cause of death worldwide [16], and hypertension is the most common chronic disease and the most important risk factor for cardiovascular disease [17]. Although CAD mortality rates have gradually declined in Western countries over the past few decades, the condition still causes about one-third of deaths in people over 35 years of age [18]. MACCEs remain the major cause of mortality and morbidity in patients both in hypertension or CAD patients [19, 20].
However, it has been reported in the literature that the incidence of MACCEs is significantly higher in CAD combined with hypertension patients compared with non-CAD or non-hypertension patients [21, 22], but the reasons remain to be unknown. The traditional risk factors of MACCEs include fasting glucose, heart rate variability, blood pressure [23,24,25,26] and dyslipidemia [27]. As previous reported, AT1R gene polymorphism was found to be associated with the development of CAD in Chinese population [28, 29]. Here we found AT1R rs389566 TT genotype may be an independent risk factor for the development of MACCEs in patients with hypertension especially those combined with CAD. The main effects of Renin-Angiotensin-Aldosterone System (RAAS) on cardiovascular system are atherosclerosis and hypertension, leading to congestive heart failure and MACCEs [30]. And Ang II also promotes the development of atherosclerosis through AT1 receptors, stimulating the secretion of inflammatory mediators, and converting stable plaques into vulnerable plaques [31]. Overexpression of the AT1R gene leads to myocardial hypertrophy and ventricular remodeling [32]. The previously study demonstrates that the AT1R polymorphism is associated with abnormal coronary vasoconstriction which causes rupture of plaque and thrombus formation [33].
Xinjiang is a multi-ethnic region, and there are 13 ethnic groups living here. Most residents like high-salt, high-calorie high-fat diet and low vegetable intake. Influential factors of unhealthy living habits lead to high incidence of obesity, hyperglycemia, hyperlipidemia and hypertension. These risk factors increase the risk of cardiovascular and cerebrovascular diseases in hypertensive patients [34]. According to the best knowledge of ours, we have not found the prevalence of MACCEs in Xinjiang population, but other studies had shown that valvular heart diseases were more common in the Han and Kazakh compared with the Uyghur [35]. The prevalence of chronic heart failure was higher in the Kazakh than the Han or Uyghur [36], and the prevalence of peripheral arterial disease was higher in the Uyghur than the Kazakh [37]. Our study found that AT1R gene mutation was associated with the occurrence of MACCEs in hypertension patients in the Xinjiang. The patients with hypertension carrying TT genotype of the AT1R gene rs389566 were prone to MACCEs. Previous studies have been conducted on AT1R gene polymorphisms in the Chinese population, but mainly on hypertension, atherosclerosis, cardiovascular disease risk factors, and intravascular restenosis. The association of AT1R gene polymorphisms with the occurrence of MACCEs events has not been reported before. Most previous studies have focused on the association of the AT1R rs5186 (A1166C) locus polymorphism and acute myocardial infarction in Caucasian, Asian, African, Brazilian, and Durban populations, and the C allele was proved to be a risk factor for occurrence of myocardial infarction [38]. In Asia, previous studies [38, 39] reported that AT1R A1166C polymorphism may influence the occurrence of myocardial infarction susceptibility in Chinese. However, the sample size of these studies is relatively small, and fewer studies have focused on the relationship between AT1R rs16860760 and MACCEs. In the present study, we found the significant association between AT1R rs389566 polymorphism and MACCEs in Chinese hypertensive population which could help provide a clinical basis for future targeted interventions.
Different ethnic groups in Xinjiang may have different genetic backgrounds, diets and living environments, and it is necessary to carry out further genetic and laboratory investigations to distinguish the differences among different ethnic groups.
Besides AT1R gene polymorphism, the age is also a factor affecting the occurrence of MACCEs. Our study found that the occurrence of MACCEs is higher in older age population, Patients with hypertension over 60 years are more likely to occur MACCEs and the prevalence is about 54.7% and it was consistent with previous study [40]. For aged population, MACCEs prevention should be emphasized in future.
Our study confirmed that AT1R rs389566 TT genotype increased the occurrence of MACCEs in hypertension patients.
Conclusion
In summary, this study provides the current status of risk factors for the occurrence of MACCEs in hypertensive patients combined with CAD in Xinjiang, China. Angiotensin receptor blocker (ARB) is an important drug for the treatment of hypertension and heart failure. We found that the incidence of MACCEs in hypertensive patients with TT genotype of AT1R rs389566 gene polymorphism increased after gene mutation. so, the regulation of AT1R is very important for hypertension patients. ARB drugs can act on AT1R. In theory, the standardized application of ARB drugs can reduce the occurrence of MACCEs in hypertension patients. The incidence of MACCEs in hypertension patients combined with CAD is higher. We should actively prevent and treat CAD to prevent MACCEs. The present findings provide potential intervention targets for the prognosis of patients who are at high risk of MACCEs, and this will help clinician do genomics-based personalized therapy in future.
Limitation
This study also has some limitations. First, the sample size was not large enough. Second, participants in the current study were recruited only at the First Affiliated Hospital of Xinjiang Medical University, which may not necessarily reflect the true prevalence of hypertension combined with CAD and the occurrence of MACCEs at the provincial or national level. Thirdly, in our study, MACCEs is the end point. Of the 715 subjects we included, 117 cases (23%) had MACCEs and the incidence of MACCEs was low. In order to reflect the universality of MACCEs with AT1R rs389566 genotype in hypertensive population, it needs longer follow-up and larger sample size support. Finally, we focused our interest on the AT1R gene polymorphism: as discussed, many other factors are involved in MACCEs and may cause increase in occurrence. Broader analyses are therefore encouraged to better understand the complexity of the MACCEs occurrence process.
Data Availability
The datasets used and analyzed during the current study available from the corresponding author on reasonable request.
Change history
30 June 2023
A Correction to this paper has been published: https://doi.org/10.1186/s12872-023-03368-8
References
Paz Ocaranza M, Riquelme JA, García L, Jalil JE, Chiong M, Santos RAS, Lavandero S. Counter-regulatory renin-angiotensin system in cardiovascular disease. Nat Rev Cardiol. 2020;17:116–29.
Silva GM, França-Falcão MS, Calzerra NTM, Luz MS, Gadelha DDA, Balarini CM, Queiroz TM. Role of renin-angiotensin System Components in Atherosclerosis: Focus on Ang-II, ACE2, and Ang-1-7. Front Physiol. 2020;11:1067.
R C SM. Blood pressure, antihypertensive drug treatment and the risks of stroke and of coronary heart disease. Br Med Bull (British medical bulletin). 1994;50:278–98.
Slivnick J, Lampert BC. Hypertension and heart failure. Heart Fail Clin. 2019;15:531–41.
Frąk W, Wojtasińska A, Lisińska W, Młynarska E, Franczyk B, Rysz J. Pathophysiology of Cardiovascular Diseases: New Insights into Molecular Mechanisms of Atherosclerosis, Arterial Hypertension, and Coronary Artery Disease.Biomedicines2022,10.
Tiret L, Bonnardeaux A, Poirier O, Ricard S, Marques-Vidal P, Evans A, Arveiler D, Luc G, Kee F, Ducimetiere P, et al. Synergistic effects of angiotensin-converting enzyme and angiotensin-II type 1 receptor gene polymorphisms on risk of myocardial infarction. Lancet. 1994;344:910–3.
Bonnardeaux A, Davies E, Jeunemaitre X, Fery I, Charru A, Clauser E, Tiret L, Cambien F, Corvol P, Soubrier F. Angiotensin II type 1 receptor gene polymorphisms in human essential hypertension. Hypertension. 1994;24:63–9.
Cuspidi C, Tadic M, Grassi G, Mancia G. Treatment of hypertension: the ESH/ESC guidelines recommendations. Pharmacol Res. 2018;128:315–21.
Mancia G. The new american guidelines on hypertension: a favorable opinion. J Clin Hypertens (Greenwich). 2014;16:255–6.
Fredman L, Sexton M, Cui Y, Althuis M, Wehren L, Hornbeck P, Kanarek N. Cigarette smoking, alcohol consumption, and screening mammography among women ages 50 and older. Prev Med. 1999;28:407–17.
Arslan F, Bongartz L, Ten Berg JM, Jukema JW, Appelman Y, Liem AH, de Winter RJ, van ‘t Hof AWJ, Damman P. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: comments from the dutch ACS working group. Neth Heart J. 2018;26:417–21.
Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González-Juanatey JR, Harjola VP, Jankowska EA, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)developed with the special contribution of the heart failure Association (HFA) of the ESC. Eur Heart J. 2016;37:2129–200.
Bao L, Zhuomin L, Yunqian L. Comparison of coronary angiography and three kinds of noninvasive methods in the diagnosis of coronary artery disease. Chin J cardiovscular. 1999;27:105–6.
Wu C-K, Tsai C-T, Chang Y-C, Luo J-L, Wang Y-C, Hwang J-J, Lin J-L, Tseng C-D, Chiang F-T. Genetic polymorphisms of the angiotensin II type 1 receptor gene and diastolic heart failure.Journal of Hypertension2009,27.
Jin-jun R, Yuan J, Qiao-lan L. Meta-analysis on the risks factors of coronary heart diease. Med J west china. 2014;26:1629–32.
Lino CA, Barreto-Chaves ML. Beta-arrestins in the context of cardiovascular diseases: focusing on angiotensin II type 1 receptor (AT1R). Cell Signal. 2022;92:110253.
Hypertension WGoCGftMo, League CH, Cardiology CSo, Committee CMDAH, Care, HBoCIEaPAfMaH. Association HBoCGM: 2018 Chinese guidelines for the management of hypertension.Chinese Journal of Cardiovascular Medicine2019,24.
Sanchis-Gomar F, Perez-Quilis C, Leischik R, Lucia A. Epidemiology of coronary heart disease and acute coronary syndrome.Ann Trans Med2016,4.
Miao B, Hernandez AV, Alberts MJ, Mangiafico N, Roman YM, Coleman CI. Incidence and predictors of major adverse cardiovascular events in patients with established atherosclerotic disease or multiple risk factors. J Am Heart Association(J Am Heart Assoc). 2020;9:e014402.
Wong Y-K, Cheung CY, Tang CS, Au K-W, Hai JS, Lee C-H, Lau K-K, Cheung BM, Sham P-C, Xu A. Age-biomarkers-clinical risk factors for prediction of cardiovascular events in patients with coronary artery disease. Arteriosclerosis, Thrombosis,Vascular Biology(Arterioscler Thromb V asc Biol) 2018, 38:2519–2527.
zhang j. The characteristics of blood pressure and its relationship with the incidence of Cardiovascular Event in patients with essential hypertension combining Coronary Heart Disease. Chin J Integr Med cardiovscular disease. 2009;7:141–3.
Jespersen L, Hvelplund A, Abildstrøm SZ, Pedersen F, Galatius S, Madsen JK, Jørgensen E, Kelbæk H, Prescott E. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. Eur Heart J. 2011;33:734–44.
Cao X, Kang Y, Tian Y, Wang X, Chen Z, Zhang L, Zheng C, Chen L, Zhou H, Wang Z. Attributable risk of cardiovascular mortality associated with different glycometabolic status among different regions in China. Chin J Cardiovasc Med. 2022;27:60–5.
Xuehui J, Lixia G, Beiyan Z, Yujin T. The influence of heart rate variability on the prognosis of elderly patients with heart failure.Chinese Journal of Cardiovascular Medicine2022,27.
Keith M, Diaz, Tanner RM, Falzon L, Levitan EB, Reynolds K, Shimbo D, Muntner P. Visit-to-visit variability of blood pressure and cardiovascular disease and all-cause mortality: a systematic review and meta-analysis. Hypertension. 2014;64:965–82.
Gosmanova EO, Mikkelsen MK, Molnar MZ, Lu JL, Yessayan LT, Kalantar-Zadeh K, Kovesdy CP. Association of systolic blood pressure variability with mortality,Coronary Heart Disease, Stroke,and Renal Disease. J Am Coll Cardiol. 2016;68:1375–86.
Boey E, Gay GMW, Poh K-K, Yeo T-C, Tan H-C, Lee C-H. Visit-to-visit variability in LDL- and HDL-cholesterol is associated with adverse events after ST-segment elevation myocardial infarction: a 5-year follow-up study. Atherosclerosis. 2016;244:86–92.
Liu C, Li Y, Guan T, Lai Y, Shen Y, Zeyaweiding A, Zhao H, Li F, Maimaiti T. ACE2 polymorphisms associated with cardiovascular risk in uygurs with type 2 diabetes mellitus. Cardiovasc Diabetol. 2018;17:127.
Li Y, Li X, Jia N, Guo S, Chu S, Niu W. Meta-analysis of the association between angiotensin II receptor, type 1 gene A1166C polymorphism and coronary artery disease in chinese populations. J Renin-Angiotensin-Aldosterone Syst. 2013;14:82–90.
Kumar R, Singh VP, Baker KM. The intracellular renin–angiotensin system: implications in cardiovascular remodeling. Curr Opin Nephrol Hypertens. 2008;17:168–73.
N D-Y PP, FW P. Overexpression of angiotensin I type I receptor in cardiomyocytes induces cardiachypertrophy and remodeling.Proc Natl Acad Sei U S A2000:931–936.
Paradis P, Dali-Youcef N, Paradis FW, Thibault Gt, Nemer M. Overexpression of angiotensin II type I receptor in cardiomyocytes induces cardiac hypertrophy and remodeling. The Proceedings of the National Academy of Sciences 2000, 97:931–936.
C A, F MHCB, N R, Lablanche HEPMXE. The angiotensin II type 1 receptor gene polymorphism is AssociatedWith coronary artery vasoconstriction. J Am Coll Cardiol. 1997;29:486–90.
Gai MT, Ma YT, Yang YN, Liu F, Xie X, Li XM, Ma X, Fu ZY, Chen BD, Chen XC. [Current status regarding the cardiovascular disease-related risk levels among the hypertensive population of different ethnicities in Xinjiang Uygur Autonomous Region, China]. Zhonghua Yi Xue Za Zhi. 2016;96:565–9.
Wang YT, Tao J, Maimaiti A, Adi D, Yang YN, Li XM, Ma X, Liu F, Chen BD, Ma YT. Prevalence of valvular heart diseases and associated risk factors in Han, Uygur and Kazak population in Xinjiang, China. PLoS ONE. 2017;12:e0174490.
Yang YN, Ma YT, Liu F, Huang D, Li XM, Huang Y, Tang Q, Chen BD, Ma X, Xie X, et al. [Incidence and distributing feature of chronic heart failure in adult population of Xinjiang]. Zhonghua xin xue guan bing za zhi. 2010;38:460–4.
Chen P, Ma YT, Yang YN, Liu F, Huang D, Li XM, Huang Y, Ma X, Xie X, Yang SJ, Yu ZX. [Prevalence of peripheral arterial disease and its correlative risk factors in Xinjiang Uygur and Kazak adult populations]. Zhonghua Yi Xue Za Zhi. 2010;90:3115–8.
Feng X, Zheng B-S, Shi J-J, Qian J, He W, Zhou H-F. A systematic review and meta-analysis of the association between angiotensin II type 1 receptor A1166C gene polymorphism and myocardial infarction susceptibility. J Renin-Angiotensin-Aldosterone Syst. 2014;15:307–15.
Zhang H, Sun M, Peng J, Sun T, Zhang Y, Yang J. Association of the angiotensin type 1 receptor gene A1166C polymorphisms with myocardial infarction: a meta-analysis. J Thromb haemostasis. 2011;9:1258–60.
Shuyao W, Yan L, Qian S. Multivariate analysis of risk and prognostic factors in patients with Coronary Heart Disease. Chin Gen Pract. 2018;21:3562–70.
Acknowledgements
Not applicable.
Funding
The survey was funded by the Xinjiang Young Scientific and Technical Talents Training Project (2020Q087, 2019Q040), the National Natural Science Foundation of China (82160054, 81960078, 81960073), and State Key Laboratory of Pathogenesis, Prevention and Treatment of High Incidence Diseases in Central Asia, Xinjiang Medical University (SKL-HIDCA-2021-XXG4).
Author information
Authors and Affiliations
Contributions
X-ML, X-MG and Y-NY were involved in the study design of the experiments. J-YL, G-LD, Y-MH, FL, TZ and B-BF performed the experiments, evaluated the data and wrote the manuscript. J-YL, G-LD and Y-MH were involved in data analysis and manuscript editing. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study conducted according to the standards of the Declaration of Helsinki and its experimental protocols was approved by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University. Written informed consent was obtained from all subjects and/or their legal guardian(s). All participants consented for drawing their blood samples and collection of their relevant clinical data.
Consent for publication
Not applicable.
Competing Interests
All of these authors declared that they had no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: funding statement has been updated.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Luo, JY., Du, GL., Hao, YM. et al. AT1R gene rs389566 polymorphism contributes to MACCEs in hypertension patients. BMC Cardiovasc Disord 23, 284 (2023). https://doi.org/10.1186/s12872-023-03223-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-023-03223-w