
Abstract
Background
Atrial fibrillation (AF) is the most common cardiac arrhythmia in patients with chronic kidney disease (CKD) and acute coronary syndrome (ACS). This study aimed to explore the frequency and impact of AF on clinical outcomes in CKD patients with ACS.
Methods
CKD inpatients with ACS between November 2014 and December 2018 were included based on the improving care for cardiovascular disease in China-ACS (CCC-ACS) project. Included patients were divided into an AF group and a non-AF group according to the discharge diagnosis. Multivariable logistic regression was used to adjust for potential confounders.
Results
A total of 16,533 CKD patients with ACS were included. A total of 1418 (8.6%) patients had clinically recognized AF during hospitalization, 654 of whom had an eGFR of 45 to < 60 ml/min/1.73 m2, and 764 had an estimated glomerular filtration rate (eGFR) < 45 ml/min/1.73 m2. Compared with the non-AF group, the AF group had a higher risk of in-hospital mortality [OR 1.250; 95% CI (1.001–1.560), P = 0.049] and major adverse cardiovascular events (MACEs) [OR 1.361; 95% CI (1.197–1.547), P < 0.001]. We also found that compared with patients with eGFR 45 to < 60 ml/min/1.73 m2, patients with eGFR < 45 ml/min/1.73 m2 had a 1.512-fold increased risk of mortality and a 1.435-fold increased risk of MACEs.
Conclusions
AF was a risk factor affecting the short-term prognosis of ACS patients in the CKD population. Furthermore, the lower the eGFR, the higher the risk of in-hospital mortality and MACEs in CKD patients with ACS.
Trial registry: Clinicaltrial.gov, NCT02306616. Registered 29 November 2014, https://clinicaltrials.gov/ct2/show/NCT02306616?term=NCT02306616&draw=2&rank=1
Similar content being viewed by others


Background
Chronic kidney disease (CKD) has become a global public health problem [1, 2]. In 2012, it was reported that the prevalence of CKD in China reached 10.8% [3]. Patients with CKD have an increased risk of cardiovascular events and mortality, due to anemia, arterial calcification and vascular endothelial dysfunction [4,5,6,7]. Moreover, patients with CKD are in a two- to three-fold higher risk of atrial fibrillation (AF) than that in the general population due to left ventricular hypertrophy, poor ventricular compliance, left ventricular dilatation and activation of the renin angiotensin system [8,9,10]. AF is also the most common cardiac arrhythmia in patients with acute coronary syndrome (ACS), with an incidence ranging between 5 and 23% [11,12,13,14]. We can see that the incidence of AF in CKD patients is high, and the clinical prognosis is poor. The prognosis of ACS patients with CKD is also poor. AF is a common arrhythmia in ACS patients. In CKD, the occurrence of AF and the prognosis of ACS patients cause the attention of clinicians. We though that patients with AF may show a poor prognosis in CKD patients with ACS. However, there is currently no consensus on the role of AF on the prognosis of CKD patients with ACS [15,16,17,18,19,20]. Most of the studies of AF in ACS have been done in general patients including CKD and non-CKD patients. There is little information about the association of AF with clinical outcomes across the spectrum of CKD patients. Therefore, patients with CKD experiencing ACS are under-treated for AF. Based on this, the purpose of this study was to explore the association between AF and in-hospital outcomes in CKD patients with ACS.
Methods
This article was a retrospective study based on the Improving Care for Cardiovascular Disease in China-Acute Coronary Syndrome (CCC-ACS) project, which is a national, hospital-based quality improvement project with an ongoing database, aiming to increase adherence to ACS guidelines in China and to improve patient outcomes. The project was launched in 2014 as a collaborative initiative of the American Heart Association (AHA) and the Chinese Society of Cardiology (CSC). A total of 92,509 patients from 246 hospitals were recruited, representing the diversity of ACS care in hospitals in China. Clinical data were collected via a web-based data collection platform (Oracle Clinical Remote Data Capture, Oracle Corporation). Data elements collected in this study included patient demographics, medical history, symptoms on arrival, in-hospital treatments, discharge medications, and secondary prevention strategies. The eligible patients each month were consecutively entered into the online data reporting system before the middle of the following month after patient discharge. The following four approaches were adopted to ensure the accuracy and completeness of the data: (1) face-to-face training workshops, (2) use of a standardized online reporting tool, (3) onsite quality control, and (4) monitoring of data completeness. Details of the design and methodology of the CCC-ACS project have been published previously [21].
From November 2014 to December 2018, CKD patients with ACS from the CCC-ACS were enrolled based on the principal discharge diagnosis and laboratory testing value at admission. ACS was defined in accordance with the guidelines published by the Chinese Society of Cardiology for the diagnosis and management of patients with ST-segment-elevation myocardial infarction (STEMI) and non-ST-segment elevation (NSTE) ACS [22, 23]. CKD was defined as eGFR < 60 ml/min/1.73 m2. CKD severity was then categorized according to the KDIGO guidelines as follows [24]: eGFR 45 to < 60 ml/min/1.73 m2 and eGFR < 45 ml/min/1.73 m2. The included patients were divided into the AF group and the non-AF group according to the discharge diagnosis. Patients in the AF group were further divided into previous and new-onset AF based on whether they had new-onset AF during this hospitalization. Institutional review board approval was granted for the aggregate data set for research and quality improvement by the Ethics Committee of Beijing Anzhen Hospital, Capital Medical University. As this was a large population-based study, approval from the Ethics Committee of Beijing Anzhen Hospital, Capital Medical University, included a waiver of informed consent.
The diagnosis of AF was based on the discharge diagnosis, and all patients’ clinical data were collected through the Web data collection platform, which had automatic data review and query function to ensure the accuracy and integrity of data. The doctors of the CCC-ACS project partner hospitals will judge whether the ACS patients had AF during their hospitalization. The CCC-ACS project partner hospitals were all certified general hospitals. Past medical history was derived from the inquiry and record of the patient’s medical history. All the laboratory testing values were the values tested the first time after admission. The first creatinine level measured during hospitalization was used to calculate the estimated glomerular filtration rate (eGFR). eGFR was calculated with the Chronic Kidney Disease Epidemiology Collaboration equation [25].
The outcomes of this study included in-hospital all-cause mortality and major adverse cardiovascular events (MACEs). MACEs were defined as a composite of reinfarction, heart failure, cardiogenic shock, cardiac arrest, stent thrombosis, and stroke (ischemic and hemorrhagic).
Continuous variables are presented as the mean and standard deviation (SD) or median and interquartile range (IQR) when distribution and variance met the appropriate conditions. Categorical variables are presented as percentages. Comparisons between groups of continuous variables were performed by t test or Mann–Whitney U test (Kruskal–Wallis). The chi-square test was used to compare the categorical variables. A multivariate logistic regression model was used to determine the association between AF and in-hospital outcomes by controlling for potential confounders. The variables entered in the multivariate model were clinically relevant variables and those significant in univariable models. For variables with missing values, the sequential regression multiple imputation method implemented by IVEware software version 0.2 (Survey Research Center, University of Michigan, Ann Arbor, MI, USA) was used to impute the missing values. All P values were 2-tailed, and P < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS 23.0 (SPSS Inc., Chicago, IL).
Results
This study included 16,533 CKD (eGFR < 60 ml/min/1.73 m2) patients with ACS. A total of 1418 (8.6%) patients had clinically recognized AF during hospitalization, and 654 (46.1%) of these patients had an eGFR of 45 to < 60 ml/min/1.73 m2, and 764 (53.9%) had an eGFR < 45 ml/min/1.73 m2. In our study, of the 1418 patients in the AF group, 592 patients (41.75%) had previous AF and 824 patients (58.25%) had new-onset AF. Patients in the AF group were more likely to be older and have previous hypertension, heart failure, CABG and stroke (all P < 0.001) (Table 1).
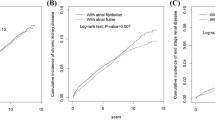
In our study, the proportion of patients who received antiplatelet, warfarin, statins, beta-blockers and ACEI/ARB drugs before admission was low regardless of whether they had AF. Compared with patients without AF, patients with AF were more likely to be treated with warfarin (3.2% vs 0.2%, P < 0.001) and beta-blockers (12.8% vs 10.9%, P = 0.030), while they were less likely to receive percutaneous coronary intervention (40.9% vs 55.9%, P < 0.001) during hospitalization (Additional file 1: Table S1). We could also know that 71 patients (5.0%) with AF received warfarin anticoagulation during hospitalization, and 949 patients (66.9%) received subcutaneous anticoagulation therapy. As shown in Fig. 1, compared with patients without AF, patients with AF had a poorer prognosis. The proportion of mortality (7.40% vs 4.90%, P < 0.001) and MACEs (29.30% vs 20.10%, P < 0.001) were significantly higher in the AF group (Fig. 1). After adjusting for confounders, AF was significantly related to in-hospital mortality [OR 1.250; 95% CI (1.001–1.560), P = 0.049] (Table 2) and MACEs [OR 1.361; 95% CI (1.197–1.547), P < 0.001] (Table 3). Further analysis showed that new-onset AF was significantly related to in-hospital mortality and MACEs [OR 1.334; 95% CI (1.013–1.755), P = 0.040; OR 1.346; 95% CI (1.143–1.586), P < 0.001, respectively]. However, prior AF was significantly related to in-hospital MACEs [OR 1.369; 95% CI (1.129–1.661), P = 0.001, not related to mortality [OR 1.149; 95% CI (0.812–1.625), P = 0.433]. We also found that compared with the patients with eGFR 45 to < 60 ml/min/1.73 m2, patients with eGFR < 45 ml/min/1.73 m2 had a 1.512-fold increased risk of mortality (Table 2) and a 1.435-fold increased risk of MACEs (Table 3).

Prevalence of in-hospital outcomes in patients with or without AF. *P < 0.001. AF atrial fibrillation, MACEs major adverse cardiovascular events
Discussion
This study was the first known study on the incidence and prognosis of ACS with concomitant AF in patients with CKD from a Chinese database. The results showed that the prevalence of ACS with concomitant AF was 8.6% in patients with CKD, which was similar to the findings of previous studies conducted in the general population (5.0–23.0%) [9,10,11]. In this study, AF included both new-onset AF during hospitalization and pre-existing AF because the diagnosis of AF was based on the discharge diagnosis in the database. We found that 41.7% of the cases of AF in this study were pre-existing. Our study showed that the patients with AF were more likely to be older; have comorbidities, such as previous hypertension and heart failure; and have lower baseline eGFR, which was consistent with previous studies [26,27,28]. In addition, the proportion of ACS patients with AF receiving PCI during hospitalization was significantly lower than that of those without AF, which was also consistent with our clinical practice. In the CKD population, the proportion of ACS patients with other cardiovascular diseases receiving PCI was lower than that of patients with ACS alone due to the greater risk of adverse events. In our study, we focused on the prognosis of patients with ACS during hospitalization, a period that has the highest risk of early clinical events [29]. Some previous studies suggested that AF can increase the risk of short-term and long-term mortality, stroke and bleeding events in ACS patients [30,31,32]. However, there were also studies that reported different results. Kinjo et al. analyzed the data of 2475 patients with AMI who underwent PCI within 24 h after onset. The results revealed that AF was an independent predictor of 1-year mortality but was not a predictor of in-hospital mortality [26]. Luca et al. analyzed the data of 16,803 ACS patients in Italy. The results showed that AF at admission was not an independent predictor of in-hospital mortality, although patients with AF had a higher risk of mortality than those without AF. However, the characteristics of AF and the stratified analysis of renal function were not mentioned in this study [33]. The incidence of AF in CKD patients is high, and the clinical prognosis is poor. The prognosis of ACS patients with CKD is also poor. AF is a common arrhythmia in ACS patients. In CKD, the occurrence of AF and the prognosis of ACS patients cause the attention of clinicians and should be studied.
In our study, AF was defined according to the discharge diagnosis, which made it more accurate in terms of the patients’ characteristics. The results showed that the risk of in-hospital mortality and MACEs was significantly higher in the AF group than in the non-AF group. Moreover, after adjusting for confounders, AF was found to be an independent risk factor for in-hospital mortality and MACEs in CKD patients with ACS. Further analysis showed that new-onset AF was significantly related to in-hospital mortality and MACEs. However, prior AF was significantly related to in-hospital MACEs, not related to mortality. Furthermore, we analyzed the relationship between renal function and in-hospital prognosis in CKD patients with ACS. The results showed that the decrease in renal function was an independent risk factor for adverse in-hospital outcomes in CKD patients with ACS. These patients, especially those with severe renal insufficiency, should be given more attention and closer monitoring in clinical practice to reduce the incidence of in-hospital mortality and MACEs.
Our study also had some limitations. First, since this study included observational data from a large database, although we adjusted for a wide range of potential confounders, we cannot rule out residual confounding factors, including whether the AF was new-onset or pre-existing and the type, occurrence time and duration of AF. Second, because of the atypical symptoms of some patients with AF, there may be some cases of undiagnosed AF. Third, due to the limitation of data collection, the definition of CKD in our study only included eGFR < 60 ml/min/1.73 m2, which is different from the KDIGO criteria. Finally, due to the observational nature of the study, causality and the underlying mechanisms could not be determined.
Conclusions
In summary, our study was the first and largest to investigate ACS with concomitant AF in CKD patients in China. In this study, we found that AF was a risk factor affecting the short-term prognosis of ACS patients in the CKD population. Furthermore, the lower the eGFR, the higher the risk of in-hospital mortality and MACEs in CKD patients with ACS. These patients, especially those with severe renal insufficiency, should be given more attention and closer monitoring in clinical practice. Further studies are needed to investigate the effect of AF on the long-term prognosis of CKD patients with ACS.
Availability of data and materials
The datasets used and analyzed during the current study are available from the principal investigator of CCC-ACS on reasonable request.
Abbreviations
- AF:
-
Atrial fibrillation
- CKD:
-
Chronic kidney disease
- ACS:
-
Acute coronary syndrome
- CCC-ACS:
-
Care for cardiovascular disease in China-acute coronary syndrome
- eGFR:
-
Estimated glomerular filtration rate
- MACEs:
-
Major adverse cardiovascular events
- AHA:
-
American Heart Association
- CSC:
-
Chinese Society of Cardiology
- STEMI:
-
ST-segment-elevation myocardial infarction
- NSTE:
-
Non-ST-segment elevation
- SD:
-
Standard deviation
- IQR:
-
Interquartile range
- HF:
-
Heart failure
- CABG:
-
Coronary artery bypass grafting
- ACEI:
-
Angiotensin-converting enzyme inhibitor
- ARB:
-
Angiotensin receptor blockade
- PCI:
-
Percutaneous coronary intervention
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- LVEF:
-
Left ventricular ejection fraction
References
Eckardt KU, Coresh J, Devuyst O, Johnson RJ, Kottgen A, Levey AS, Levin A. Evolving importance of kidney disease: from subspecialty to global health burden. Lancet. 2013;382(9887):158–69.
Gasparini A, Evans M, Coresh J, Grams ME, Norin O, Qureshi AR, Runesson B, Barany P, Arnlov J, Jernberg T, Wettermark B, Elinder CG, Carrero JJ. Prevalence and recognition of chronic kidney disease in Stockholm healthcare. Nephrol Dial Transplant. 2016;31(12):2086–94.
Zhang L, Wang F, Wang L, Wang W, Liu B, Liu J, Chen M, He Q, Liao Y, Yu X, Chen N, Zhang JE, Hu Z, Liu F, Hong D, Ma L, Liu H, Zhou X, Chen J, Pan L, Chen W, Wang W, Li X, Wang H. Prevalence of chronic kidney disease in China: a cross-sectional survey. Lancet. 2012;379(9818):815–22.
Shlipak MG, Fried LF, Crump C, Bleyer AJ, Manolio TA, Tracy RP, Furberg CD, Psaty BM. Elevations of inflammatory and procoagulant biomarkers in elderly persons with renal insufficiency. Circulation. 2003;107(1):87–92.
Hsu CY, McCulloch CE, Curhan GC. Epidemiology of anemia associated with chronic renal insufficiency among adults in the United States: results from the Third National Health and Nutrition Examination Survey. J Am Soc Nephrol. 2002;13(2):504–10.
London GM, Guérin AP, Marchais SJ, Métivier F, Pannier B, Adda H. Arterial media calcification in end-stage renal disease: impact on all-cause and cardiovascular mortality. Nephrol Dial Transplant. 2003;18(9):1731–40.
Washam JB, Herzog CA, Beitelshees AL, Cohen MG, Henry TD, Kapur NK, Mega JL, Menon V, Page RL II, Newby LK, and on behalf of the American Heart Association Clinical Pharmacology Committee of the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, Council on Functional Genomics and Translational Biology, Council on the Kidney in Cardiovascular Disease, and Council on Quality of Care and Outcomes Research. Pharmacotherapy in chronic kidney disease patients presenting with acute coronary syndrome: a scientific statement from the American Heart Association. Circulation. 2015;131(12):1123–49.
Gupta J, Mitra N, Kanetsky PA, Devaney J, Wing MR, Reilly M, Shah VO, Balakrishnan VS, Guzman NJ, Girndt M, Periera BG, Feldman HI, Kusek JW, Joffe MM, Raj DS, CRIC Study Investigators. Association between albuminuria, kidney function, and inflammatory biomarker profile in CKD in CRIC. Clin J Am Soc Nephrol. 2012;7(12):1938–46.
Alonso A, Lopez FL, Matsushita K, Loehr LR, Agarwal SK, Chen LY, Coresh J, Soliman EZ, Astor BC. Chronic kidney disease is associated with the incidence of atrial fibrillation: the atherosclerosis risk in communities (ARIC) study. Circulation. 2011;123(25):2946–53.
Parikh NI, Hwang S-J, Larson MG, Meigs JB, Levy D, Fox CS. Cardiovascular disease risk factors in chronic kidney disease: overall burden and rates of treatment and control. Arch Intern Med. 2006;166(17):1884–91.
Dewland TA, Olgin JE, Vittinghoff E, Marcus GM. Incident AF among Asians, Hispanics, blacks, and whites. Circulation. 2013;128(23):2470–7.
Foussas S. Acute coronary syndromes and AF. Hellenic J Cardiol. 2016;57(2):141–2.
Schmitt J, Duray G, Gersh BJ, Hohnloser SH. AF in acute myocardial infarction: a systematic review of the incidence, clinical features and prognostic implications. Eur Heart J. 2009;30(9):1038–45.
Jabre P, Roger VL, Murad MH, Chamberlain AM, Prokop L, Adnet F, Jouven X. Mortality associated with AF in patients with myocardial infarction: a systematic review and meta-analysis. Circulation. 2011;123(15):1587–93.
Nagai M, Itoh T, Ishida M, Fusazaki T, Komatsu T, Nakamura M, Morino Y. New-onset AF in patients with acute coronary syndrome may be associated with worse prognosis and future heart failure. J Arrhythm. 2019;35(2):182–9.
Al Khdair D, Alshengeiti L, Elbarouni B, Yan RT, Grondin FR, Spencer FA, Pallie S, Brieger D, Eagle KA, Mangat I, Singh S, Goodman SG, Yan AT, Global Registry of Acute Coronary Events (GRACE/GRACE2) and the Canadian Registry of Coronary Events (CANRACE) Investigators. Management and outcome of acute coronary syndrome patients in relation to previous history of AF. Can J Cardiol. 2012;28(4):453–9.
González-Pacheco H, Márquez MF, Arias-Mendoza A, Álvarez-Sangabriel A, Eid-Lidt G, González-Hermosillo A, Azar-Manzur F, Altamirano-Castillo A, Briseño-Cruz JL, García-Martínez A, Mendoza-García S, Martínez-Sánchez C. Clinical features and in-hospital mortality associated with different types of AF in patients with acute coronary syndrome with and without ST elevation. J Cardiol. 2015;66(2):148–54.
Rene AG, Généreux P, Ezekowitz M, Kirtane AJ, Xu K, Mehran R, Brener SJ, Stone GW. Impact of AF in patients with ST-elevation myocardial infarction treated with percutaneous coronary intervention (from the HORIZONS-AMI [Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction] trial). Am J Cardiol. 2014;113(2):236–42.
Topaz G, Flint N, Steinvil A, Finkelstein A, Banai S, Keren G, Shacham Y, Yankelson L. Long term prognosis of AF in ST-elevation myocardial infarction patients undergoing percutaneous coronary intervention. Int J Cardiol. 2017;240(15):228–33.
Ulus T, Isgandarov K, Yilmaz AS, Vasi I, Moghanchızadeh SH, Mutlu F. Predictors of new-onset AF in elderly patients with acute coronary syndrome undergoing percutaneous coronary intervention. Aging Clin Exp Res. 2018;30(12):1475–82.
Hao Y, Liu J, Liu J, Smith SC Jr, Huo Y, Fonarow GC, Ma C, Ge J, Taubert KA, Morgan L, Guo Y, Zhang Q, Wang W, Zhao D, CCC-ACS Investigators. Rationale and design of the Improving Care for Cardiovascular Disease in China(CCC) project: a national effort to prompt quality enhancement for acute coronary syndrome. Am Heart J. 2016;179(9):107–15.
Chinese Society of Cardiology. Guideline for diagnosis and treatment of patients with ST-elevation myocardial infarction 2010. Chin J Cardiol. 2010;38(8):675–90.
Chinese Society of Cardiology. Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation 2012. Chin J Cardiol. 2012;40(5):353–67.
Levey AS, de Jong PE, Coresh J, El Nahas M, Astor BC, Matsushita K, Gansevoort RT, Kasiske BL, Eckardt KU. The definition, classification, and prognosis of chronic kidney disease: a KDIGO controversies conference report. Kidney Int. 2011;80(1):17–28.
Stevens LA, Schmid CH, Greene T, Zhang YL, Beck GJ, Froissart M, Hamm LL, Lewis JB, Mauer M, Navis GJ, Steffes MW, Eggers PW, Coresh J, Levey AS. Comparative performance of the CKD epidemiology collaboration (CKD-EPI) and the modification of diet in renal disease (MDRD) study equations for estimating GFR levels above 60 mL/min/1.73 m2. Am J Kidney Dis. 2010;56(3):486–95.
Kinjo K, Sato H, Sato H, Ohnishi Y, Hishida E, Nakatani D, Mizuno H, Fukunami M, Koretsune Y, Takeda H, Hori M, Osaka Acute Coronary Insufficiency Study (OACIS) Group. Prognostic significance of AF/atrial flutter in patients with myocardial infarction treated with percutaneous coronary intervention. Am J Cardiol. 2003;92(10):1150–4.
Lopes RD, Pieper KS, Horton JR, Al-Khatib SM, Newby LK, Mehta RH, Van de Werf F, Armstrong PW, Mahaffey KW, Harrington RA, Ohman EM, White HD, Wallentin L, Granger CB. Short- and long-term outcomes following AF in patients with acute coronary syndromes with or without ST-segment elevation. Heart. 2008;94(7):867–73.
Almendro-Delia M, Valle-Caballero MJ, Garcia-Rubira JC, Muñoz-Calero B, Garcia-Alcantara A, Reina-Toral A, Benítez-Parejo J, Hidalgo-Urbano R, ARIAM Andalucia Study Group. Prognostic impact of AF in acute coronary syndromes: results from the ARIAM registry. Eur Heart J Acute Cardiovasc Care. 2014;3(2):141–8.
Budaj A, Flasinska K, Gore JM, Anderson FA Jr, Dabbous OH, Spencer FA, Goldberg RJ, Fox KA, GRACE Investigators. Magnitude of and risk factors for in-hospital and postdischarge stroke in patients with acute coronary syndromes: findings from a Global Registry of Acute Coronary Events. Circulation. 2005;111(24):3242–7.
Mohamed MO, Kirchhof P, Vidovich M, Savage M, Rashid M, Kwok CS, Thomas M, El Omar O, Al Ayoubi F, Fischman DL, Mamas MA. Effect of concomitant AF on in-hospital outcomes of non-ST-elevation-acute coronary syndrome-related hospitalizations in the United States. Am J Cardiol. 2019;124(4):465–75.
Hersi A, Alhabib KF, Alsheikh-Ali AA, Sulaiman K, Alfaleh HF, Alsaif S, Al-Mahmeed W, Asaad N, Haitham A, Al-Motarreb A, Suwaidi J, Shehab A. Prognostic significance of prevalent and incident AF among patients hospitalized with acute coronary syndrome: findings from the Gulf RACE-2 Registry. Angiology. 2012;63(6):466–71.
Giglioli C, Minelli M, Chiostri M, Landi D, Romano SM, Balzi D, Valente S, Padeletti L, Gensini GF, Cecchi E. Prognostic impact of AF occurrence in patients with non-ST-elevation acute coronary syndromes: is dysrhythmia duration a parameter to focus on? Intern Emerg Med. 2014;9(5):521–8.
De Luca L, Casella G, Rubboli A, Gonzini L, Lucci D, Boccanelli A, Chiarella F, Di Chiara A, De Servi S, Di Lenarda A, Di Pasquale G. Recent trends in management and outcome of patients with acute coronary syndromes and AF. Int J Cardiol. 2017;248(15):369–75.
Acknowledgements
We acknowledge all participating hospitals for their contributions to the CCC-ACS project (Additional file 1: Table S2). We would like to thank AJE (www.aje.cn) for English language editing.
Funding
The CCC-ACS project is a collaborative program of the American Heart Association and the Chinese Society of Cardiology. The American Heart Association was funded by Pfizer and AstraZeneca for the quality improvement initiative through an independent grant for learning and change’. In addition, the study of this article is supported by three funding projects: “Application and Development of Clinical Medicine with the Capital Characteristics” D10110005 0010017, Beijing, China, and “The Capital Health Research and Development of Special” 2011-2006-07, 2018-2-1051, Beijing, China. The funder of these grants all was Beijing government. The funding bodies had no role in the design of this study; in the collection, analysis, and interpretation of data; or in writing the manuscript.
Author information
Authors and Affiliations
Consortia
Contributions
HC, LJY, NY, DZ, CSM and JL designed the study; LJY, NY, GQW, WJB, FBX, YCH, JL and NY cleaned the data; LJY and NY analyzed the data; LJY, NY and HC wrote the manuscript. All authors reviewed and edited the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Institutional review board approval was granted for the aggregate data set for research and quality improvement by the Ethics Committee of Beijing Anzhen Hospital, Capital Medical University. As this was a large population-based study, approval from the Ethics Committee of Beijing Anzhen Hospital, Capital Medical University, included a waiver of informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Table S1. Treatments pre-hospital and during hospitalization. Table S2. Investigators of CCC-ACS project.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yang, L., Ye, N., Wang, G. et al. The association between atrial fibrillation and in-hospital outcomes in chronic kidney disease patients with acute coronary syndrome: findings from the improving care for cardiovascular disease in China-acute coronary syndrome (CCC-ACS) project. BMC Cardiovasc Disord 21, 345 (2021). https://doi.org/10.1186/s12872-021-02125-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-021-02125-z