
Abstract
Background
The aim of this study was to determine the difference in effects of beta-blockers on long-term clinical outcomes between ischemic heart disease (IHD) patients with mid-range ejection fraction (mrEF) and those with reduced ejection fraction (rEF).
Methods
Data were assessed of 3508 consecutive IHD patients who underwent percutaneous coronary intervention (PCI) between 1997 and 2011. Among them, 316 patients with mrEF (EF = 40–49%) and 201 patients with rEF (EF < 40%) were identified. They were assigned to groups according to users and non-users of beta-blockers and effects of beta-blockers were assessed between mrEF and rEF patients, separately. The primary outcome was a composite of all-cause death and non-fatal acute coronary syndrome.
Results
The median follow-up period was 5.5 years in mrEF patients and 4.3 years in rEF patients. Cumulative event-free survival was significantly lower in the group with beta-blockers than in the group without beta-blockers in rEF (p = 0.003), whereas no difference was observed in mrEF (p = 0.137) between those with and without beta-blockers. In the multivariate analysis, use of beta-blockers was associated with reduction in clinical outcomes in patients with rEF (hazard ratio (HR), 0.59; 95% confidence interval (CI), 0.36–0.97; p = 0.036), whereas no association was observed among those with mrEF (HR 0.74; 95% CI 0.49–1.10; p = 0.137).
Conclusions
Our observational study showed that use of beta-blockers was not associated with long-term clinical outcomes in IHD patients with mrEF, whereas a significant association was observed in those with rEF.
Similar content being viewed by others

Background
Ischemic heart disease (IHD) is the most common cause of heart failure (HF) with left ventricular (LV) dysfunction [1,2,3]. The severity of LV systolic dysfunction is an important prognostic factor in patients with IHD [4], possibly because impaired LV systolic function increases likelihood of developing HF and ventricular arrhythmia, both of which could be fatal conditions. In the last few decades, significant advancements in treatments for IHD have been made through the adoption of healthy behaviors (i.e., restriction of salt intake, endorsement of physical activity, smoking cessation), improvement in interventional cardiology (i.e., less invasiveness in devices for catheter intervention, development of coronary stents) and evidence-based medical therapy, including beta-blockers, angiotensin-converting enzyme inhibitors (ACEIs), statins, and aspirin [5]. Despite the advancements, cardiovascular events, such as acute coronary syndrome (ACS), development of HF, and sudden cardiac death, still remain a matter of concern for patients with IHD, which requires further refinement of treatment strategies in order to reduce subsequent cardiovascular events in those patients. Beta-blockers have been established as evidence-based medical therapy to prevent secondary cardiovascular events [6, 7]. However, the evidence has originated largely from studies examining patients with myocardial infarction, especially those complicated with HF or LV systolic dysfunction. Furthermore, there has been debate over the long-term beneficial effects of beta-blockers in IHD patients without HF or previous myocardial infarction. It is possible that the effects of beta-blockers may vary depending on LV ejection fraction (EF), considering the inconsistent results between studies in patients with and without reduced EF (rEF). Recently, the European Society of Cardiology guideline has proposed a new classification for HF which defines those with EF of between 40 and 49% as mid-range EF (mrEF), for those who have not been classified as either HF with rEF or HF with preserved EF. To date, optimal medical therapy for IHD patients with mrEF has not been established and few studies have examined to see if beta-blockers would be useful in those with mrEF. We hypothesized that effects of beta-blockers in IHD patients would be different between patients with mrEF and those with rEF. In this study, we aimed to investigate differences in the effects of beta-blockers on long-term clinical outcomes in IHD patients with mrEF and those with rEF.
Methods
Subjects
We used data from an observational cohort which consists of 3508 consecutive IHD patients who underwent their first percutaneous coronary intervention (PCI) at Juntendo University Hospital (Tokyo, Japan) between January 1997 and October 2011. Three hundred and sixty-three patients whose information on EF were missing, were excluded from analyses. Among 3145 patients, we identified individuals with EF < 50% at the time of their PCI and they were subsequently grouped into two groups according to ranges of their EF. Patients with EF of between 40 and 49% were classified as mrEF group, while those with EF < 40% were classified as rEF group. For each group, we further divided the study population into two groups according to whether they were prescribed with beta-blockers or not at discharge. Decisions on the prescription of beta-blockers were at the discretion of attending doctors based on patients’ clinical status (i.e., comorbid with hypertension, presentation of acute myocardial infarction as the type of IHD, presence of ventricular arrhythmia). Associations between beta-blocker and risks of clinical events were assessed in patients with rEF and mrEF groups, separately.
Informed consent was obtained from all patients before performing PCI. This study was conducted under the approval of our institutional review board in accordance with the Declaration of Helsinki. The ethics application approval number was 17-206.
Data collection
Baseline data, including age, sex, body mass index (BMI), blood pressure (BP), smoking status, family history of IHD, medication use, and comorbidities that include hypertension, diabetes mellitus (DM), dyslipidemia, and chronic kidney disease (CKD), were prospectively collected. In elective cases, blood samples were collected early in the morning of the day of PCI after an overnight fast. Hypertension was defined as systolic blood pressure (BP) ≥ 140 mm Hg, diastolic BP ≥ 90 mm Hg, or medication with antihypertensive drugs. DM was defined as fasting plasma glycemic levels ≥ 126 mg/dL, medication with oral hypoglycemic drugs, or insulin injections. A current smoker was defined as a person who smoked at the time of PCI or who had quit smoking within a year before their PCI. CKD was defined as an estimated glomerular filtration rate (eGFR) of < 60 mL/min/1.73 m2, which was calculated based on the Modification of Diet in Renal Disease Study equation modified with a Japanese coefficient using baseline serum creatinine [8].
Outcomes
The follow-up period ended on December 31, 2011. Survival data and information on clinical events were collected through serial contact with the patients or their families and, for patients who died or underwent follow-up at our hospital, assessed based on medical records. Details of hospital admission and cause of death were supplied by other hospitals or clinics where the patients had been admitted. Investigators performed blinded collection of all data.
In this study, the primary outcome was a composite event of all-cause death and non-fatal acute coronary syndrome (ACS). We defined ACS as ST-elevation myocardial infarction (STEMI), non-STEMI, or unstable angina pectoris. We determined STEMI based on symptoms of ischemia with ST-segment elevation in electrocardiogram and increased serum levels of cardiac enzymes (troponin, creatinine kinase (CK) MB, CK ≥ two-fold increase) [9, 10], and non-STEMI based on symptoms of ischemia without ST-segment elevation in electrocardiogram and increased serum levels of cardiac enzymes. Unstable angina pectoris was determined based on symptoms of ischemia at rest or the presence of a crescendo of symptoms or new-onset symptoms associated with transient ischemic ST-segment shifts and normal serum levels of cardiac enzymes [11].
Statistical analysis
Results are expressed as means ± standard deviation or median (interquartile range (IQR)) for continuous variables and as ratios (%) for categorical variables. Baseline data were compared using an unpaired t-test or Mann–Whitney U test for continuous variables and the chi-squared test or Fisher’s exact test for categorical variables. Kaplan–Meier survival curves were constructed to compare cumulative event rates between mrEF and rEF groups with the log-rank test as a significance test. Cox proportional hazard regression analyses were conducted to identify whether use of beta-blockers would be associated with the primary composite outcome. Factors associated with outcomes were determined using univariate Cox proportional hazard regression analyses with the following variables: age, sex, hypertension, DM, CKD, family history of IHD, current smoking status, low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), LVEF, and presentation of ACS as well as medication use that included statins, ACEIs or angiotensin receptor blockers (ARBs), aspirin and beta-blockers or no beta-blockers. Variables with a p value < 0.1 in univariate analyses were included in multivariate Cox proportional hazard regression analyses. A p value of < 0.05 was considered significant, unless otherwise indicated. All data were analyzed using JMP 10.0 MDSU statistical software (SAS Institute, Cary, NC, USA).
Results
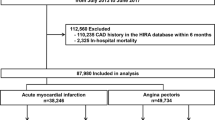
Figure 1 shows a flow chart of the study population. We initially selected 530 patients with LV systolic dysfunction (EF < 50%) among 3508 patients who underwent their first PCI. Patients whose information on prescription of beta-blockers were missing, were excluded (N = 13). In total, 517 patients were enrolled and assigned to two groups: mrEF (EF 40–49%) or rEF (EF < 40%). Both groups of people were subsequently assigned to two groups according to users or non-users of beta-blockers. The prescription rates of beta-blockers were 51.6% and 49.3% in mrEF and rEF, respectively. Table 1 shows the baseline characteristics of each group. In mrEF group, BMI and use of statins were significantly higher in patients with beta-blockers than in those without. In the rEF group, hypertension, diastolic BP and use of aspirin, ACE-Is/ARBs, Type B2/C lesion, drug eluting stent (DES) use, and statins were significantly higher in patients with beta-blockers than in those without. The minimal lumen diameter at baseline was significantly smaller in patients with beta-blockers than in those without.

Study flow chart. CAD, coronary artery disease; IHD, ischemic heart disease; mrEF, mid-range ejection fraction; PCI, percutaneous coronary intervention; rEF, reduced ejection fraction
The median follow-up period was 5.5 (IQR 2.5–9.0) years in the mrEF group and 4.3 (IQR 1.1–7.9) years in the rEF group, and outcome data were fully documented during the entire follow-up period. Figure 2 shows cumulative event rates comparing those with and without beta-blockers. No difference was observed in the incidence of the primary composite outcome between patients with and without beta-blockers in the mrEF group (log-rank test, p = 0.137). On the other hand, the cumulative incidence was lower in patients with beta-blockers than those without in the rEF group (log-rank test, p = 0.003). The numbers and percentages of each event are shown in Table 2. Similarly, Fig. 3 shows no difference in the cumulative incidence of all-cause death between those with and without beta-blockers in the mrEF group, whereas in the rEF group, the cumulative incidence of all-cause death in patients with beta-blockers was lower than that in those without them. Table 3 shows univariate and multivariate Cox proportional hazards regression analyses including variables with p < 0.1 in the univariate analysis for the mrEF group. Table 4 shows univariate and multivariate Cox proportional hazards regression analysis including variables with p < 0.1 in univariate analysis for the rEF group similarly. In the multivariate Cox proportional hazards regression analysis for the primary outcome in the mrEF group, greater age, and presence of DM were significant independent predictors of the outcome, while use of beta-blockers was not a significant independent predictor, even in the univariate Cox proportional hazards regression analysis (HR 0.74; 95% CI 0.49–1.10; p = 0.137) (Table 3). On the other hand, in the multivariate Cox proportional hazards regression analysis in the rEF group, beta-blocker use was a significant independent predictor of favorable outcomes (HR 0.59; 95% CI 0.36–0.97; p = 0.036) in addition to using ACEIs/ARBs. Also, greater age and presence of CKD and ACS were significant independent predictors of unfavorable outcomes. (Table 4).

Cumulative incidence rates of the primary composite outcome for those with and without beta-blockers in the mrEF and rEF. There was no significant difference in the cumulative incidence rates of the primary outcome between the two groups in the mrEF (log-rank test, p = 0.137). There was a significant difference in the cumulative incidence rates of the primary outcome between the two groups (log-rank test, p = 0.003) in the rEF

Cumulative incidence rates of all-cause death for those with and without beta blockers in the mrEF and rEF. There was a no significant difference in the cumulative incidence rates of all-cause death between the two groups in the mrEF (log-rank test, p = 0.575). There was a significant difference in the cumulative incidence rate of all-cause death between the two groups in rEF (log-rank test, p = 0.026)
Discussion
This observational study demonstrated that beta-blocker use was not significantly associated with a reduction in the composite of all-cause death and non-fatal ACS among those with mrEF. In contrast, use of beta-blockers was associated with reduction in the events among those with rEF. The prescription rates of beta-blockers were 51.6 and 49.3% in IHD patients with mrEF and rEF, respectively. Our study suggested that the effects of beta-blockers on long-term clinical outcomes in IHD patients may differ based on their ranges of LVEF. In particular, these findings may affect daily clinical practice in patients with IHD and remind physicians the importance of measuring LVEF in patients undergoing PCI.
Prior studies have shown that beta-blockers could improve clinical outcomes in IHD patients [6, 7, 12, 13]. As a result, many guidelines have adopted beta-blockers as one of the first-line drugs for patients with recent myocardial infarction in order to improve their clinical courses by preventing subsequent cardiovascular events, including recurrent coronary events, development of HF, ventricular arrhythmia and death [14, 15], which partly support our finding that use of beta-blockers was associated with a reduction in clinical outcomes for IHD patients who underwent PCI. However, most of the previous studies demonstrating the beneficial effects of beta-blockers have focused on patients with impaired LV systolic function or those complicated with HF. Furthermore, the protective effects of beta-blockers have not been well established in a certain subset of patients whose conditions are not complicated with LV dysfunction [16,17,18]. Considering the inconsistent results regarding the beneficial effects of beta-blockers between patients with rEF [6, 7] and those on preserved EF [16,17,18], it has been speculated that LVEF has a role of modifying the effects beta-blockers on prevention of cardiovascular events. However, this has not been fully examined. Our study investigated IHD patients with mrEF, which is a relatively new category for differentiating HF patients according to their LVEF. In this study, the prescription rate of beta-blockers in patients with mrEF was higher than in those with rEF. No associations were observed between beta-blockers and the composite of all-cause death and non-fatal ACS in those with mrEF, whereas the associations were significant in those with rEF, suggesting that the beneficial effects of beta-blockers may vary depending on ranges of LVEF. Prior evidence has suggested that patients with HF with preserved EF would not necessarily benefit from beta-blockers as opposed to those with HF with reduced EF [16,17,18]. Our study further demonstrated that IHD patients with even modest impairment of LVEF may not be proper candidates for beta-blockers in the long run. Optimal medical therapies have not been established for patients with HF with mrEF as well as IHD patients with mrEF.
Beta-blocker is one of the recommended anti-ischemic drugs for improving angina through reduction in myocardial oxygen consumption and increase in the threshold to myocardial ischemia. Although previous studies have demonstrated that beta-blocker therapy is effective in reducing cardiovascular events, including death and recurrent myocardial infarction (MI), in patients with coronary artery disease, most of the studies were conducted prior to the widespread use of reperfusion therapy, which had dramatically changed the clinical practices for the patients, and the beneficial effects of beta-blockers were limited to patients experiencing MI and those with reduced LVEF [6, 7]. On the other hand, the survival benefits of beta-blockers for IHD patients with mrEF remain unclear. Our study showed no associations between beta-blockers and long-term clinical outcomes, including all-cause death and non-fatal ACS, in IHD patients with mrEF, whereas the association was significant in those with rEF. Given the various adverse effects attributed to beta-blockers, such as depression, dizziness, and bradycardia [19, 20], which are likely to exert in elderly people, broad use of beta-blockers should be avoided, and appropriate patient selection should be made based on the presence of angina, history of MI, reduced LVEF, as well as concomitant HF. It should be noted that in IHD patients with mrEF, the presence of DM was an independent predictor of worse clinical outcomes, which is similar to the results of prior studies [21,22,23]. This should be further investigated in larger scale studies with a consideration of the effects of beta blockers in mrEF patients with and without DM in the IHD population.
Our study had some limitations. First, it was not possible to exclude unmeasured confounders in this observational study setting, although several variables were adjusted in the multivariate Cox regression analyses. For example, information about the dosage of beta-blockers was not available. Heart rate, which may be suggestive of an effect of the beta-blockers effect, was not considered because no information regarding heart rate is available. Their effects on the clinical outcomes remain unknown. Because subjects of the present study are from the IHD patient population, information regarding the management and treatment of HF, such as B-type natriuretic peptide levels, some medications for HF (i.e., aldosterone antagonists and diuretics), and cardiac implantable devices (e.g., implantable cardioverter defibrillator or cardiac resynchronization therapy which can also affect mortality [24]) is unavailable. Second, data on symptoms related to myocardial ischemia were not available for this study. However, associations between beta-blockers and improvement in angina were beyond the scope of this study. Considering the small number of participants from a single institution in this study, further studies involving post-hoc analyses of large-scale multicentric observational studies or prospective randomized controlled trials are needed to better understand the usefulness of beta-blockers in the management of IHD with mrEF.
Conclusions
Beta-blockers were not associated with a reduction in the long-term clinical outcomes of IHD patients with mrEF, whereas a significant association was observed in those with rEF. Appropriate patient selection should be made based on the presence of angina, history of MI, concomitant HF as well as LVEF.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request. All data generated or analysed during this study are included in this published article.
Abbreviations
- ACEI:
-
angiotensin-converting enzyme inhibitors
- ACS:
-
acute coronary syndrome
- ARB:
-
angiotensin receptor blockers
- BMI:
-
body mass index
- BMS:
-
bare metal stent
- BP:
-
blood pressure
- CI:
-
confidence interval
- CK:
-
creatinine kinase
- CKD:
-
chronic kidney disease
- DES:
-
drug-eluting stent
- DM:
-
diabetes mellitus
- eGFR:
-
estimated glomerular filtration rate
- HDL-C:
-
high-density lipoprotein cholesterol
- HF:
-
heart failure
- HR:
-
hazard ratio
- IHD:
-
ischemic heart disease
- LAD:
-
left anterior descending artery
- LDL-C:
-
low-density lipoprotein cholesterol
- LMT:
-
left main trunk
- LVEF:
-
left ventricular ejection fraction
- MI:
-
myocardial infarction
- MLD:
-
minimal lumen diameter
- mrEF:
-
mid-range ejection fraction
- PCI:
-
percutaneous coronary intervention
- rEF:
-
reduced ejection fraction
- STEMI:
-
ST-elevation myocardial infarction
References
Lloyd-Jones DM, Larson MG, Leip EP, Beiser A, D’Agostino RB, Kannel WB, Murabito JM, Vasan RS, Benjamin EJ, Levy D. Lifetime risk for developing congestive heart failure: the Framingham Heart Study. Circulation. 2002;106(24):3068–72.
McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Bohm M, Dickstein K, Falk V, Filippatos G, Fonseca C, Gomez-Sanchez MA et al: ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2012, 33(14):1787–1847.
Shiba N, Nochioka K, Miura M, Kohno H, Shimokawa H. Trend of westernization of etiology and clinical characteristics of heart failure patients in Japan–first report from the CHART-2 study. Circul J. 2011;75(4):823–33.
Lamblin N, Meurice T, Tricot O, Lemesle G, Deneve M, de Groote P, Bauters C. Effect of left ventricular systolic dysfunction on secondary medical prevention and clinical outcome in stable coronary artery disease patients. Arch Cardiovasc Dis. 2017;110(1):35–41.
Elgendy IY, Mahtta D, Pepine CJ. Medical therapy for heart failure caused by ischemic heart disease. Circ Res. 2019;124(11):1520–35.
Jánosi A, Ghali JK, Herlitz J, Czuriga I, Klibaner M, Wikstrand J, Hjalmarson A. Metoprolol CR/XL in postmyocardial infarction patients with chronic heart failure: experiences from MERIT-HF. Am Heart J. 2003;146(4):721–8.
Dargie HJ. Effect of carvedilol on outcome after myocardial infarction in patients with left-ventricular dysfunction: the CAPRICORN randomised trial. Lancet (London, England). 2001;357(9266):1385–90.
Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, Yamagata K, Tomino Y, Yokoyama H, Hishida A. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53(6):982–92.
Thygesen K, Alpert JS, White HD. Universal definition of myocardial infarction. Eur Heart J. 2007;28(20):2525–38.
Jaffe AS, Ravkilde J, Roberts R, Naslund U, Apple FS, Galvani M, Katus H. It’s time for a change to a troponin standard. Circulation. 2000;102(11):1216–20.
Cannon CP, Brindis RG, Chaitman BR, Cohen DJ, Cross JT Jr, Drozda JP Jr, Fesmire FM, Fintel DJ, Fonarow GC, Fox KA, et al. 2013 ACCF/AHA key data elements and definitions for measuring the clinical management and outcomes of patients with acute coronary syndromes and coronary artery disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on clinical data standards (writing committee to develop acute coronary syndromes and coronary artery disease clinical data standards). Circulation. 2013;127(9):1052–89.
von Arnim T. Medical treatment to reduce total ischemic burden: total ischemic burden bisoprolol study (TIBBS), a multicenter trial comparing bisoprolol and nifedipine. The TIBBS Investigators. J Am Coll Cardiol. 1995;25(1):231–8.
Fox KM, Mulcahy D, Findlay I, Ford I, Dargie HJ. The Total Ischaemic Burden European Trial (TIBET). Effects of atenolol, nifedipine SR and their combination on the exercise test and the total ischaemic burden in 608 patients with stable angina. The TIBET Study Group. Eur Heart J. 1996;17(1):96–103.
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, Caforio ALP, Crea F, Goudevenos JA, Halvorsen S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2017;39(2):119–77.
Smith SC Jr, Benjamin EJ, Bonow RO, Braun LT, Creager MA, Franklin BA, Gibbons RJ, Grundy SM, Hiratzka LF, Jones DW, et al. AHA/ACCF secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation. Circulation. 2011;124(22):2458–73.
Dondo TB, Hall M, West RM, Jernberg T, Lindahl B, Bueno H, Danchin N, Deanfield JE, Hemingway H, Fox KAA, et al. beta-blockers and mortality after acute myocardial infarction in patients without heart failure or ventricular dysfunction. J Am Coll Cardiol. 2017;69(22):2710–20.
Watanabe H, Ozasa N, Morimoto T, Shiomi H, Bingyuan B, Suwa S, Nakagawa Y, Izumi C, Kadota K, Ikeguchi S, et al. Long-term use of carvedilol in patients with ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention. PLoS ONE. 2018;13(8):e0199347.
Puymirat E, Riant E, Aissaoui N, Soria A, Ducrocq G, Coste P, Cottin Y, Aupetit JF, Bonnefoy E, Blanchard D, et al. β blockers and mortality after myocardial infarction in patients without heart failure: multicentre prospective cohort study. BMJ (Clin Res ed). 2016;354:i4801.
Lauterbach M. Clinical toxicology of beta-blocker overdose in adults. Basic Clin Pharmacol Toxicol. 2019;125(2):178–86.
Dahlöf C, Dimenäs E. Side effects of beta-blocker treatments as related to the central nervous system. Am J Med Sci. 1990;299(4):236–44.
Marfella R, Sardu C, Calabrò P, Siniscalchi M, Minicucci F, Signoriello G, Balestrieri ML, Mauro C, Rizzo MR, Paolisso G, et al. Non-ST-elevation myocardial infarction outcomes in patients with type 2 diabetes with non-obstructive coronary artery stenosis: effects of incretin treatment. Diabetes Obes Metab. 2018;20(3):723–9.
Marfella R, Sardu C, Balestrieri ML, Siniscalchi M, Minicucci F, Signoriello G, Calabrò P, Mauro C, Pieretti G, Coppola A, et al. Effects of incretin treatment on cardiovascular outcomes in diabetic STEMI-patients with culprit obstructive and multivessel non obstructive-coronary-stenosis. Diabetol Metabol Syndrome. 2018;10:1.
Sardu C, Paolisso P, Sacra C, Mauro C, Minicucci F, Portoghese M, Rizzo MR, Barbieri M, Sasso FC, D’Onofrio N, et al. Effects of metformin therapy on coronary endothelial dysfunction in patients with prediabetes with stable angina and nonobstructive coronary artery stenosis: the CODYCE multicenter prospective study. Diabetes Care. 2019;42(10):1946–55.
Sardu C, Paolisso P, Sacra C, Santamaria M, de Lucia C, Ruocco A, Mauro C, Paolisso G, Rizzo MR, Barbieri M, et al. Cardiac resynchronization therapy with a defibrillator (CRTd) in failing heart patients with type 2 diabetes mellitus and treated by glucagon-like peptide 1 receptor agonists (GLP-1 RA) therapy vs. conventional hypoglycemic drugs: arrhythmic burden, hospitalizations for heart failure, and CRTd responders rate. Cardiovasc Diabetol 2018, 17(1):137.
Acknowledgements
We thank the staff of the Department of Cardiovascular Medicine at Juntendo University. We are also grateful to Yumi Nozawa and Ayako Onodera for their secretarial assistance.
Funding
This study was partly supported by a Grant-in-Aid for Scientific Research (C) [Grant Number 26507010]; JSPS KAKENHI Grant Number JP17K09527, by a Grant-in-Aid for Early Career Scientists Grant Number 18K15904, by a grant to Intractable Respiratory Diseases and Pulmonary Hypertension Research Group, from the Ministry of Health, Labor and Welfare of Japan, No. 20FC1027.
Author information
Authors and Affiliations
Contributions
All authors listed have contributed sufficiently to the project to be included as authors, and all those who are qualified to be authors are listed in the author byline. J.S. and T.K. contributed to designing the study protocol, collecting clinical data, supervising data management and statistical analysis, and drafting the manuscript. H.E., H.W., S.D., H.K., S.T., M.O., T.D., S.O., K.M. contributed to collecting clinical data and reviewing the manuscript. H.D. was involved in supervision and funding acquisition. I attest to the fact that all authors listed on the title page have read the manuscript, attest to the validity and legitimacy of the data and its interpretation, and agree to its submission to BMC cardiovascular disorders. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods were carried out in accordance with relevant guidelines and regulations.
All experimental protocols were approved by a Juntendo University review board in accordance with the Declaration of Helsinki. The ethics application approval number was 17–206. Informed consent was obtained from all patients and all subjects were over 20 in this study.
Consent for publication
Not applicable.
Competing interests
T.K is affiliated with a department endowed by Philips Respironics, ResMed, Teijin Home Healthcare, and Fukuda Denshi. R.N is affiliated with a department endowed by Philips Respironics, ResMed, Teijin Home Healthcare, and Fukuda Denshi. H.D received speakers’ Bureau/Honoraria from Kowa Pharmaceutical Company Ltd., Sanofi-Aventis K.K., Daiichi Sankyo Company., Takeda Pharma ceutical Co., Ltd., Bayer Yakuhin Ltd., MSD K.K., Astellas Pharma Inc., Amgen Astellas BioPharma K.K., AstraZeneca K.K., and research funds from Sanwakagaku Kenkyusho Co., Ltd., Canon Medical Systems Corporation., Kowa Pharmaceutical Company Ltd., Daiichi Sankyo Company., Abbott Medical Japan Co., Ltd., Nihon Medi-Physics Co., Ltd., and Scholarship funds from Abbott Medical Japan Co., Ltd., Nippon Boehringer Ingelheim Co., Ltd., Otsuka Pharmaceutical Co., Ltd., Bayer Yakuhin Ltd., Astellas Pharma Inc., Dainippon Sumitomo Pharma Co., Ltd., Pfizer Co., Ltd., Daiichi Sankyo Company., Takeda Pharma ceutical Co., Ltd., Abbott Medical Japan Co., Ltd., Actelion Pharmaceuticals Ltd., Mitsubishi Tanabe Pharma Corporation., Teijin Pharma Ltd., that are unrelated to this study. All other authors declare no conflict of interest. These funding sources have no other roles in this study. The sponsor had no role in the design of the study, the collection and analysis of the data, or the preparation of the manuscript.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shitara, J., Naito, R., Kasai, T. et al. Differing effects of beta-blockers on long-term clinical outcomes following percutaneous coronary intervention between patients with mid-range and reduced left ventricular ejection fraction. BMC Cardiovasc Disord 21, 36 (2021). https://doi.org/10.1186/s12872-021-01850-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-021-01850-9