
Abstract
Background
The main sedative which is propofol in painless gastroenteroscopy, has a high risk of reducing blood pressure and respiratory depression. Remimazolam (a short-acting benzodiazepine) is expected to be widely used in painless gastroenteroscopy due to its rapid onset, rapid metabolism and light respiratory and circulation inhibition.
Methods
A randomized, single-blind, parallel, controlled study, 123 outpatients who were undergoing painless colonoscopy and ramdomly divided into group A, B and C, in Hangzhou First People’s Hospital, July-December 2021. All patients were intravenously injected with 5 µg sufentanil for analgesic preconditioning. The group A was induced by 0.2 mg/kg remimazolam besylate. The group B was induced by 0.25 mg/kg remimazolam besylate. And the group C was inducted by 2.0 mg /kg propofol. If the patients had limb movement or MOAA/S score > 3 and so on, remimazolam besylate was added at 2.5 mg/ time in group A and B, and propofol emulsion injection was added at 0.5 mg/kg/ time in group C. During the operation, according to the actual situation, remimazolam was per added 2.5 mg in the experimental group, and propofol was 0.5 mg/kg in the control group. Heart rate (HR), non-invasive blood pressure (BP), respiratory rate (RR), pulse oxygen saturation (SpO2), and improved vigilance/sedation score (MOAA/S) of patients was recorded from entering endoscopy room to get out of the anesthesia recovery room, also including perioperative adverse events, other medications or treatments, the time of patients waking up and leaving the hospital.
Results
The successful rate of induction in three groups was 100%. There was no significant difference in the sedation completion rate among the three groups (Group A:90.2%, Group B: 92.7%, Group C: 92.7%, P = 1.000). The rate of adverse events after administration: group A(27.0%) and B(36.8%) both lower than group C(71.0%),P < 0.001;There was no significant difference between group A and group B, P > 0.744;The average time from the last drug administration to meet the discharge criteria of the subjects in three groups was as follows: The average time of group A(16.2 min) and Group B(16.5 min) both shorter than group C(19.6 min), P = 0.001; There was no significant difference between group A and group B, P = 0.742. Conclusions: This study revealed that remimazolam is a safe and effective medication for colonoscopy sedation, the security of remimazolam is better than propofol, and the sedative effect with the initial dose of 0.25 mg/kg of remimazolam is optimal.
Trial registration
China Clinical Trial Center with registration number: 2100052615,02/11/2021.
Similar content being viewed by others


Background
Endoscopy is a well-accepted and widely used method in the diagnosis and treatment of gastrointestinal diseases [1, 2]. Sedation and anesthesia in endoscopic procedures has the benefit of eliminating anxiety and discomfort in patients and improving patient acceptance of and satisfaction with endoscopic procedures, it’s also useful for improving the completion rate, quality of endoscopic examination and treatment outcomes of therapeutic endoscopy from the viewpoint of endoscopists [3].
In China, the total intravenous anesthesia(TIVA) commonly used for sedating patients during a procedure involves the use of two major hypnotics, midazolam, and propofol, often in combination with an opioid analgesic, typically fentanyl, or sufentanil [4, 5]. Midazolam has potent anxiolytic effect with amnesia, sedation, skeletal muscle relaxant activity, and good hemodynamic stability with lack of significant side effects in doses < 0.5 mg/kg and the onset time is about 3–5 min. A single dose of midazolam with an elimination half-life of 20–80 min, while multiple doses produced greater accumulative effects of its long-acting metabolite that causes a slower recovery of neuropsychiatric function [6, 7]. Propofol is a commonly used agent in total intravenous anesthesia. Propofol has high lipophilicity and can quickly cross the blood-brain barrier to achieve a deep sedative effect in a short period of time. However, propofol has a number of known limitations, such as high incidence of hypotension, respiratory depression, pain on injection and a lack of availability of antagonists [4, 8].
Remimazolam (CNS7056) is a new ultrashort-acting benzodiazepine developed for use in sedation and anesthesia that acts on the central GABAa receptor, opening the channel and increasing the inward flow of chloride ions, causing hyperpolarization of the nerve cell membrane and thus inhibiting neuronal activity, producing sedation and amnesia etc [9, 10]. Phase I pharmacokinetic trials demonstrated that remimazolam had an onset time of 1–3 min and a steady-state half-life of 7–8 min after a 2-h simulated infusion similar to propofol, and there is no active metabolite and almost no accumulation [11,12,13]. When compared with propofol in both sedation and general anesthesia, remimazolam exhibited better safety profile, including a lower incidence of hypotension, less bradycardia treatment requirement, and no pain on injection [14, 15], and flumazenil can antagonize the effects of remimazolam there is almost no rebound phenomenon [12, 16].
The study used a randomized, single blind, controlled method to evaluate the safety and effectiveness of remimazolam in colonoscopy diagnosis and treatment, and remimazolam is divided into two dose groups for administration to find a suitable administration scheme.
Methods
General information
This study was approved by the Ethics Committee of Hangzhou First People’s Hospital affiliated to Zhejiang University school of medicine (Approval number: 2020 YLS No. (041) – 01,24/12/2020). All subjects were fully informed about the experimental protocol and voluntarily signed an informed consent form before the start of the study. The inclusion, exclusion and abscission criteria are shown in Table 1.
Scoring standard
Sedation level was assessed using a 6-point sedation scale, which was modified from the observer assessment of alertness and sedation scale (MOAA/S) (Table 2). The incidence and severity of injection pain were assessed using a four point scale 0 = no pain; 1 = mild pain; 2 = moderate pain and 3 = severe pain [17]. The modified Aldrete score (Table 3) was used to evaluate whether the patient could leave the Post -Anesthesia Care Unit (PACU). Recovery from sedation was assessed by using a modified Aldrete scoring system, which was evaluated every 3 min after the removal of the endoscope [18, 19].
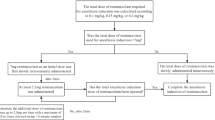
Procedures (The trial procedure is shown in Fig. 1)
Subjects who met the inclusion criteria were randomly assigned to three groups in a ratio of 1:1:1, using the random number table generated by SPSS 26.0 (SPSS Inc. Chicago, IL, United States). Patients were asked to fast 4–6 h before the examination, and intestinal preparation (lactulose and magnesium sulfate) was used to reduce bowel movements [20]. After entering the Operation room, a “Venturi” mask with an oxygen flow of 2–4 L/min was used to inhale oxygen, open the venous access, connect the monitor, and continuously monitor the electrocardiogram (ECG), invasive blood pressure (INBP), respiratory rate (RR), pulse oxygen saturation (SpO2) and heart rate (HR). The MOAA /S score assessment and bispectral index (BIS) to evaluate the depth of sedation, and the MOAA /S score was selected as the primary outcome measure. One hundred and twenty-three patients were divided into three groups: remimazolam 0.2 mg/kg (Group A), 0.25 mg /kg (Group B), and propofol 2 mg/kg (Group C).
Patients received a single dose of sufentanil 5.0 µg for analgesia. According to grouping, patients were received remimazolam or propofol intravenously within 1 min after sufentanil administration for anesthesia. Evaluation was performed every 30 s after administering sedatives, and the evaluation interval was shortened to 5 s at the beginning of study drug administration until the MOAA/S score was ≤ 3, and the longest evaluation time was no more than 3 min after the beginning of study drug administration, otherwise, supplemental remimazolam2.5 mg or propofol 30 mg were administered, and failure was recorded if two additional attempts could not make MOAA/S score was ≤ 3. During the procedure, once the patients’ eyelash reflexes (detected 2-min interval)recovered, frown, limb movement, moaning or MOAA /S score >3, supplemental remimazolam 2.5 mg or propofol 30–50 mg were administered to maintain sedation. If the patient’s body movement still significantly affects the operation after two doses were administered consecutively (the interval >2 min), it is considered sedation failure, and other sedatives were used as the rescue drug to finish the operation.
In case of hypotension, defined as systolic blood pressure less than 80 mmHg or a fall in systolic or diastolic BP of 30% or more below baseline (The setting standard for hypotension was a systolic blood pressure of less than 90mmHg, and the standard for hypotension was adjusted to a systolic blood pressure of less than 80mmHg according to the patient’s body position, measurement site and clinical observation), a bolus of norepinephrine (10ug IV) or ephedrine (6 mg IV) was administered; in case of bradycardia, defined as HR < 50, a bolus of atropine was administered (0.5 mg). In case of SpO2 drops below 92%, chin lift and/or manual or mechanical ventilation. If the MOAA/S score < 5 when completion of colonoscopy 30 min, administrate flumazenil which is the antagonist benzodiazepines [16, 18, 19] .The main observation index and secondary observation index are listed in Table 4.
Sample size and power
The sample size was estimated on PASS software version 16.0. Based on a previous study, the incidence of hypotension with remimazolam in painless gastrointestinal endoscopic was 13.04%, while the incidence with propofol was 42.86%(15). For a 1-sided type I error rate of 0.05 and a target power of 80%, 37 patients were required for the treatment group. In this study, the data from the completed sedation patients were used for analysis and statistics, and considering the failure rate of about 10%, 123 cases were finally included.
Statistical methods
SPSS26.0 software was used for data analysis. Measurement data were expressed as mean ± standard deviation (Mean ± SD), and counting data were expressed as Χ 2 Test, P<0.05 is considered statistically significant, and all tests are bilateral tests.

Flowchart of study patient enrollment
Results
General aspects and data
The subjects selected for the study were randomly divided into three groups, and each group consisted of 41 participants. The subjects were blind and did not know the trial grouping. In group A, 37 cases succeeded in sedation and 4 cases failed; In group B, 38 cases succeeded in sedation and 3 cases failed; In group C, sedation was successful in 38 cases and 3 cases failed. Finally, take 37 cases in group A, 38 cases in group B and 38 cases in group C to data analysis. There was no statistically significant difference in the baseline data of the subjects (Table 5). There was no significant difference in HR, BP, SpO2, RR, MOAA /S scores of the three groups before induction (Table 6).
Vital signs during sedation
The incidence of hypotension in Group C was 54.0%, which was significantly higher than Group A (10.8%) and Group B (18.9%) ( P<0.001), and there was no difference between Group A and Group B (P = 0.744); In addition, compared with Group C, the overall fluctuation range of blood pressure in Group A and Group B was smaller (Figs. 2, 3 and 4). The incidence of bradycardia in Group A(5.4%) and B (5.3%) was significantly lower than that in Group C (18.9%, P = 0.107); The heart rate diachronic analysis showed that the heart rate fluctuation of Group A and Group B was smaller than that of Group C (Fig. 2); There was no hypoxemia in Group A, the incidence of hypoxemia in Group B was significantly lower than that in Group C (5.3% vs. 10.5%, P = 0.163); The diachronic analysis of SpO2 and RR (Figs. 5 and 6) showed that the respiratory inhibition of Group A and Group B was smaller than that of Group C.

The change trend of HR at each time point during the perioperative period was compared among the three groups

The change trend of MAP at each time point during the perioperative period was compared among the three groups

The change trend of SBP at each time point during the perioperative period was compared among the three groups

The change trend of SpO2 at each time point during the perioperative period was compared among the three groups

The change trend of RR at each time point during the perioperative period was compared among the three groups
Adverse events
After administration, adverse events occured in Group C was 71.0% higher than Group A (27.0%) and Group B (36.8%) (P<0.001) with no life threatening events or deaths; The degree of pain at the injection site in three groups was ≤ 2, and the incidence of pain at the injection site in Group A (not occurred) and Group B (2.6%) was lower than Group C(42.1%) (P<0.001) (Table 7; Fig. 7).

The rates of major adverse reactions during perioperative period were compared among the three groups
Successful sedation
The sedation success rate was similar at 90.2%, 92.7% and 92.7% in Group A, B and C, respectively (P = 1.000). Propofol and sufentanil were used as rescue drugs for failure of sedation (Table 8).
There are 4 cases failure of sedation in group A, and these patients were sedated quickly after the first administration, with MOAA/S ≤ 3 (2 males and 2 females); Three of patients had obvious body movement during the operation of doctors, which affected the operation. The body movement reaction of the patients was still obvious after two consecutive drug supplementation, and then they were sedated with other sedatives. Another case showed obvious intestinal peristalsis during the operation of the digestive endoscopist, and the endoscopist complained that the patient had intestinal spasm and required propofol to complete sedation.
There are 3 cases failure of sedation in group B, and all patients were sedated quickly after the first administration, with MOAA/S ≤ 3 (2 male and 1 female); Two of patients had obvious body movement during the operation of digestive endoscopy doctors, which affected the operation, and their body movement was still obvious after two consecutive drug additions, and propofol was then used to maintain sedation. In another case, the doctor considered that the patient had obvious intestinal distortion and high difficulty during the operation of digestive endoscopy, so other drugs were required to maintain sedation.
There were 3 cases of sedation failure in group C, all patients were sedated quickly after the first administration, and the MOAA/S ≤ 3 (3 women). 2 patients showed obvious body movement during the operation doctors, and the obvious body movement was still seen after two consecutive doses of 30–50 mg propofol, and then sufentanil and propofol were added to maintain sedation level. The other patient showed MOAA/S > 3 points during the operation of doctor, and the MOAA/S > 3 points remained after the addition of 50 mg of propofol for two consecutive times, and the subsequent addition of propofol to maintain sedation level.
Intraoperative sedation
At T1, the MOAA/S scores of Group C were significantly lower than those of group B (P<0.001); At T1, T3 and T4, the MOAA /S scores of Group C were significantly lower than those of Group A (P = 0.001, P = 0.001, P<0.001); There was no statistically significant difference in MOAA/S scores between Group A and Group B at T0,T1,T2,T4,T5 (P = 1.000, P = 1.000, P = 0.193, P = 0.073,P = 1.000) (Table 9; Fig. 8). Timepoints T2, T3 and T4 are showing lower BIS values in Group C than those in Group A and Group B (T2:P<0.001, P<0.001; T3:P = 0.003, P = 0.033; T4:P<0.001, P = 0.002) (Fig. 9). (Due to the limitation of reality, only some subjects in each group were selected for BIS monitoring).

The change trend of MOAA/S at each time point during the perioperative period was compared among the three groups

The change trend of BIS at each time point during the perioperative period was compared among the three groups
Awakening and recovery
The mean time to reach post anaesthesia care unit discharge criteria was shorter for Group A (16.2 min) and Group B (16.5 min) as compared to Group C (19.5 min) (P = 0.011); There was no significant difference between Group A and Group B (16.2 min vs 16.5 min, P = 0.742)(Table 10).
Drug usage in test groups
The average first dose of patients in Group A was lower than Group B, while the average number of additions was higher than Group B (P = 0.022), and there was no significant difference between Group A and Group C or between Group B and Group C (P = 0.584, P = 0.867) (Fig. 10) (Fig. 11). However, there was no significant difference between the average supplemental dose and the average total amount of medication in group A and group B (P = 0.469) (Fig. 10) (Table 11).

The perioperative sedative drugs were compared among the three groups

Comparison of the first dose, additional dose and total dose of remimazolam between two groups
Discussion
This study showed that the sedation success rate in the remimazolam group was similar to that in the propofol group (P = 1.000). Compared with propofol, remimazolam showed shorter time to fully alert and reach post anesthesia care unit (PACU) discharge criteria. The MOAA/S scores of the three groups were ≤ 3 min after administration 1 min, indicating that the induction dose of remimazolam and propofol enable subjects to achieve the target sedation depth in a short time.
There was no statistical difference between the three groups in the average time from the last administration to full alert, indicating that the inhibition of remimazolam and propofol on the central nervous system was reversible, and the recovery time was not significantly different. The time from the last administration to reach post-anesthesia care unit discharge criteria of Group A and Group B was significantly shorter than Group C (P = 0.011), indicating that the metabolism time of remimazolam was shorter than propofol. This advantage is attributed to the molecular design of remimazolam. Its ultra-short-acting properties lead to its rapid breakdown into inactive metabolites by ubiquitous tissue esterase. On the other hand, this advantage was attributed to the lower depth of sedation induced by remimazolam. The sedation curve showed that the propofol group had deeper sedation and longer recovery time than the remimazolam group. This is consistent with its properties as a benzodiazepine [21]. Also, colonoscopy is a short procedure that does not require such a depth of sedation. Thus, remimazolam is sufficient to provide an acceptable sedation protocol for colonoscopy.
In the present study, remimazolam was used as a sedative agent in combination with sufentanil to achieve the level of sedation required for the colonoscopy without prolonging the time to full alert and the time to discharge criteria. Our results were also consistent with those of previous studies in showing that remimazolam was well tolerated and non-inferior to propofol [22,23,24].
The adverse events rate of Group C was significantly higher than that of Group A and Group B (P<0.001) indicated that remimazolam has less circulatory inhibition and higher safety. Colonoscopy requires intestinal preparation and fasting the day before, which makes the patient’s effective circulating blood volume relatively insufficient, and propofol lower blood pressure more significantly through the dual effects include peripheral vascular expansion and myocardial inhibition [25, 26].Therefore, we need drugs with less influence on circulation to make the sedation process more secure.
Compared with propofol, remimazolam showed a significantly lower incidence of hypotension and hypoxemia. Respiratory and circulatory depression is the most common presentation after brain stem inhibition by narcotic drugs [27]. R. N. Upton*et al. think that high doses of CNS7056 (remimazolam) and propofol cause short-term respiratory and circulatory depression of similar magnitude and duration [28]. Therefore, the small inhibitory effects of remimazolam on respiration and circulation in this study may be due to the relatively small dosage of remimazolam, or it may be due to its unique pharmacological structure, which has a relatively mild inhibitory effect on the brain stem.
The incidence of pain at the injection site in Group A and Group B was lower than Group C (0 vs. 2.6% vs42.1%), and the degree of injection pain in Group B was grade 1, which showed that remimazolam effectively reduced the incidence of injection pain. This may be attributed to the fact that remimazolam is configured with normal saline and its components provide no or less stimulation of the vessel wall. Thus, remimazolam is sufficient to provide an acceptable sedation protocol for colonoscopy.
In treatment groups, it was divided into Group A and Group B according to the first dosage. It showed that 0.20 mg /kg and 0.25 mg /kg remimazolam could achieve satisfactory sedation effect. However, remimazolam as an ultra-short-acting sedative, has too short a duration of action, which results in its rapid metabolism during injection and therefore requires a large supplementary dose during endoscopy [29, 30]. Compared with the Group A, Group B had significantly less additional times and additional volume, and did not increase the incidence of adverse reactions. The 0.3 mg/kg dosing group that was available in the study for observation and comparison study was not selected in this study because the depth of sedation was similar to that of the first two groups when induction was performed at that dose in the preliminary study. The recovery time was slightly prolonged. There is little need for additional medication.Considering that we need patients to recover quickly and accurately control the dose of drugs for painless colonoscopy, this group was not set as the experimental group. Thus, the induction dose of remimazolam from 0.2 mg/kg to 0.25 mg/kg with 2.5 mg /kg additional dose is safe and effective.
In addition, 2 cases of intractable hiccup occurred within 2–3 min after the administration of remimazolam in this study. The possible reasons as follows: (a) The reaction caused by pharmacological effects of remimazolam or sufentanil or additives; (b) The reaction caused by the patient’s own tension; (c) Adverse reactions caused by endoscopic operation or air inflation to stimulate the intestine. Hiccup was relieved gradually when patients recovered to fully alert, without obvious discomfort; The published research has not found the explanation of this adverse reaction, so we should be cautious.
In addition, our study was limited by its sample size, single blind design and the age of the subjects. The cases are all from the data of a single center. Larger population and multi-center studies are needed to provide reference for painless colonoscopy.
Conclusions
In this trial, remimazolam (Remimazolam besylate) provided safe and effective sedation for colonoscopy and reduced the occurrence of adverse reactions such as hypotension, respiratory depression, and injection pain. The initial dose of remimazolam of 0.25 mg/kg and the supplementary dose of 2.5 mg/ kg can achieve satisfactory sedation induction and maintenance effects.
Data availability
All data generated or analysed during this study are included in this published article. Some of the raw data are not publicly available and are available from the authors on request.
Abbreviations
- ASA:
-
American Society of Anesthesiologists
- BIS:
-
Bispectral index
- BMI:
-
Body Mass Index
- DBP:
-
Diastolic blood pressure
- GABA:
-
γ-aminobutyric acid
- HR:
-
Heart rate
- MAP:
-
Mean arterial pressure
- MOAA/S:
-
Modified observer’s assessment ofalertness /scores
- NIBP:
-
Non-invasive blood pressure
- NS:
-
Normal saline
- RR:
-
Respiratory rate
- SBP:
-
Systolic blood pressure
- SPSS:
-
Statistic Package for Social Science
- SpO2 :
-
Pulse oxygen saturation
- VRS:
-
VerbalRating Scale
References
Fu YH, Yang YH, He JH. Research progress of clinical application of colonoscopy. Clin Med Res Pract. 2021;6(30):189–91.
Cao B, Tao F, Cheng XX, et al. Clinical study on the safety of painless colonoscopy (report of 1700 cases). China J Endoscopy. 2011;17(11):1196–200.
Shirota Y, Hirase Y, Suda T, Miyazawa M, Hodo Y, Wakabayashi T. More than half of hypoxemia cases occurred during the recovery period after completion of esophagogastroduodenoscopy with planned moderate sedation. Sci Rep. 2020;10(1):4312.
Sneyd JR, Absalom AR, Barends CRM, Jones JB. Hypotension during propofol sedation for colonoscopy: a retrospective exploratory analysis and meta-analysis. Br J Anaesth. 2022;128(4):610–22.
Dossa F, Medeiros B, Keng C, Acuna SA, Baxter NN. Propofol versus midazolam with or without short-acting opioids for sedation in colonoscopy: a systematic review and meta-analysis of safety, satisfaction, and efficiency outcomes. Gastrointest Endosc. 2020;91(5):1015–26. e7.
Sipe BW, Rex DK, Latinovich D, Overley C, Kinser K, Bratcher L, et al. Propofol versus midazolam/meperidine for outpatient colonoscopy: administration by nurses supervised by endoscopists. Gastrointest Endosc. 2002;55(7):815–25.
Ulmer BJ, Hansen JJ, Overley CA, Symms MR, Chadalawada V, Liangpunsakul S, et al. Propofol versus midazolam/fentanyl for outpatient colonoscopy: administration by nurses supervised by endoscopists. Clin Gastroenterol Hepatol. 2003;1(6):425–32.
Chen D, Taylor KP, Hall Q, Kaplan JM. The neuropeptides FLP-2 and PDF-1 act in Concert to arouse Caenorhabditis elegans Locomotion. Genetics. 2016;204(3):1151–9.
Cornett EM, Novitch MB, Brunk AJ, Davidson KS, Menard BL, Urman RD, et al. New benzodiazepines for sedation. Best Pract Res Clin Anaesthesiol. 2018;32(2):149–64.
Kilpatrick GJ, McIntyre MS, Cox RF, Stafford JA, Pacofsky GJ, Lovell GG, et al. CNS 7056: a novel ultra-short-acting benzodiazepine. Anesthesiology. 2007;107(1):60–6.
Upton RN, Somogyi AA, Martinez AM, Colvill J, Grant C. Pharmacokinetics and pharmacodynamics of the short-acting sedative CNS 7056 in sheep. Br J Anaesth. 2010;105(6):798–809.
Eisenried A, Schuttler J, Lerch M, Ihmsen H, Jeleazcov C. Pharmacokinetics and pharmacodynamics of remimazolam (CNS 7056) after continuous infusion in healthy male volunteers: part II. Pharmacodynamics of Electroencephalogram effects. Anesthesiology. 2020;132(4):652–66.
Schuttler J, Eisenried A, Lerch M, Fechner J, Jeleazcov C, Ihmsen H. Pharmacokinetics and pharmacodynamics of remimazolam (CNS 7056) after continuous infusion in healthy male volunteers: part I. Pharmacokinetics and Clinical Pharmacodynamics. Anesthesiology. 2020;132(4):636–51.
Rex DK, Bhandari R, Lorch DG, Meyers M, Schippers F, Bernstein D. Safety and efficacy of remimazolam in high risk colonoscopy: a randomized trial. Dig Liver Dis. 2021;53(1):94–101.
Chen SH, Yuan TM, Zhang J, Bai H, Tian M, Pan CX, et al. Remimazolam tosilate in upper gastrointestinal endoscopy: a multicenter, randomized, non-inferiority, phase III trial. J Gastroenterol Hepatol. 2021;36(2):474–81.
Chen X, Sang N, Song K, Zhong W, Wang H, Jiang J, et al. Psychomotor recovery following remimazolam-induced sedation and the effectiveness of Flumazenil as an antidote. Clin Ther. 2020;42(4):614–24.
Wu HX, Chen T, Chen JL, et al. Effect of low-dose etomidate pretreatment on propofol injection pain. Fujian Med J. 2021;43(05):61–4.
Chinese expert consensus. On sedation/anesthesia for digestive endoscopy. J Clin Anesthesiol. 2014(09):920–7.
Expert consensus on. Anesthesia management for common digestive endoscopic surgery. Chin J Dig Endoscopy. 2019(01):9–19.
Han X, Guo YH, Shi XD, Zhang XL. Interpretation of Chinese Guideline for Bowel Preparation for Coloniscopy (2019). Clin Focus. 2020;35(01):72–5.
Saari TI, Uusi-Oukari M, Ahonen J, Olkkola KT. Enhancement of GABAergic activity: neuropharmacological effects of benzodiazepines and therapeutic use in anesthesiology. Pharmacol Rev. 2011;63(1):243–67.
Doi M, Morita K, Takeda J, Sakamoto A, Yamakage M, Suzuki T. Efficacy and safety of remimazolam versus propofol for general anesthesia: a multicenter, single-blind, randomized, parallel-group, phase IIb/III trial. J Anesth. 2020;34(4):543–53.
Chen S, Wang J, Xu X, Huang Y, Xue S, Wu A, et al. The efficacy and safety of remimazolam tosylate versus propofol in patients undergoing colonoscopy: a multicentered, randomized, positive-controlled, phase III clinical trial. Am J Translational Res. 2020;12(8):4594–603.
Rex DK, Bhandari R, Desta T, DeMicco MP, Schaeffer C, Etzkorn K, et al. A phase III study evaluating the efficacy and safety of remimazolam (CNS 7056) compared with placebo and midazolam in patients undergoing colonoscopy. Gastrointest Endosc. 2018;88(3):427–e376.
Deng XM. Modern Anesthesiology. 4th Ed. Modern Anesthesiology. 4th Ed; 2014.
Sneyd JR, Absalom AR, Barends CRM, Jones JB. Hypotension during propofol sedation for colonoscopy: a retrospective exploratory analysis and meta-analysis. British journal of anaesthesia. 2022;128(4):610-22
Upton R, Martinez A, Grant C. A dose escalation study in sheep of the effects of the benzodiazepine CNS 7056 on sedation, the EEG and the respiratory and cardiovascular systems. Br J Pharmacol. 2008;155(1):52–61.
Upton RN, Martinez AM, Grant C. Comparison of the sedative properties of CNS 7056, midazolam, and propofol in sheep. Br J Anaesth. 2009;103(6):848–57.
Schüttler J, Eisenried A, Lerch M, Fechner J, Jeleazcov C, Ihmsen H. Pharmacokinetics and pharmacodynamics of remimazolam (CNS 7056) after continuous infusion in healthy male volunteers: part I. Pharmacokinetics and Clinical Pharmacodynamics. Anesthesiology. 2020;132(4):636–51.
Cardia L. Remimazolam: an ultrashort-acting intravenous anesthetic suitable for general anesthesia. Minerva Anestesiol. 2021;87(10):1059–63.
Acknowledgements
We appreciated the gastroenterologists of Hangzhou First People’s Hospital for cooperating with the study and providing experimental conditions the manuscript.Authors’ information (optional)
Funding
This study was supported in part by grants from Bethune Foundation for Good (ZHYX).
Author information
Authors and Affiliations
Contributions
Qirui Sun and Jiating Cheng contributed equally to this study. Study design: Qirui Sun, Jiating Cheng, Weiping Lei, Jianliang Sun. Acquisition or analysis of data: All authors. Drafting of the manuscript: Qirui Sun, Jiating Cheng. Critical revision of the manuscript: Qirui Sun, Xinlei Lu. Statistical analysis: Qirui Sun, Xinlei Lu, Weiping Lei. Obtained funding: Weiping Lei, Jianliang Sun. Administrative, technical, or material support: Yaqin Huang, Weiping Lei, Xinlei Lu, Jianliang Sun. Study supervision: Weiping Lei, Jianliang Sun.All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The experimental protocol was established, according to the ethical guidelines of the Helsinki Declaration and was approved by the Human Ethics Committee of Hangzhou First People’s Hospital, Zhejiang Province, China. Written informed consent was obtained from individual or guardian participants. All procedures in this study were conducted in accordance with the Human Ethics Committee of Hangzhou First People’s Hospital approved protocols.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sun, Q., Cheng, J., Lei, W. et al. The effects of remimazolam combined with sufentanil on respiration, circulation and sedation level in patients undergoing colonoscopy. BMC Anesthesiol 24, 252 (2024). https://doi.org/10.1186/s12871-024-02644-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-024-02644-0