
Abstract
Background
The erector spinae plane block (ESPB) is a novel regional block technique for pain management following thoracic surgeries. However, there are minimal cases in which the technique was used as the main anesthesia technique during surgery.
Case presentation
Here, we report the successful use of ESBP for applying anesthesia in a case during an emergent thoracotomy for performing pericardiotomy and loculated tamponade evacuation.
Conclusions
Using ESPB with a higher concentration of local anesthetics, in this case, prepared appropriate anesthesia for performing an emergent thoracotomy while avoiding multiple needle insertions and the risk of further hemodynamic instability.
Similar content being viewed by others

Background
The erector Spinae plane block (ESPB) is a novel regional block technique primarily introduced by Forero et al. in 2016 for managing severe neuropathic pain [1]. Since then, ESBP has been mainly used for pain management following thoracic surgeries [2]. However, there are minimal cases in which the technique was used as the main anesthesia technique during surgery. Here, we report the successful use of ESBP for applying anesthesia in a case during an emergent thoracotomy. A written informed consent was obtained from the patient to publish identifying information.
Case presentation
A patient in their 70s was first presented to the emergency department (ED) with complaints of orthopnea, leg edema, and melena. Her symptoms started several months ago and have progressed significantly during the last three days. She had a history of heart failure and underwent open surgical valve replacement for both mitral and aortic valves; for which, she had been taking various medications, including Warfarin. On review of the tests, the international normalized ratio (INR) was far above the normal range, and the hemoglobin (Hb) level was 3.8 mg/dl. On arrival to the ED, blood pressure (BP) was 100/50mmHg, and heart rate (HR) was 70/min. The patient was awake and alert; however, she was pale.
Cardiac monitoring and continuous pulse oximetry had been applied. A bedside echocardiography was performed which revealed cardiomegaly and mild to moderate pericardial effusion. With a provisional diagnosis of decompensated heart failure and gastrointestinal bleeding, the patient commenced on packed red blood cells (PRBCs) and fresh frozen plasma (FFP). The next day, the patient underwent both endoscopy and colonoscopy for approaching gastrointestinal bleeding.
Two days later, the patient’s dyspnea was increased, and in physical examination, an enlarged jugular venous pressure (JVP) was noted. The patient’s vital signs were BP = 95/45 mmHg, HR = 110/min, RR = 24/min, and SPO2 = 90% with a face mask. Emergency bedside echocardiography showed tamponade, for which pericardiocentesis was unsuccessful. According to the patient’s condition, history of previous heart surgery, high probability of the presence of pericardial adhesion, and loculated pericardial effusion, the patient was a candidate for an emergent thoracotomy. Therefore, she was transferred to the operating room (OR).
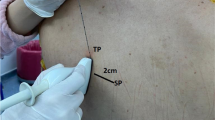
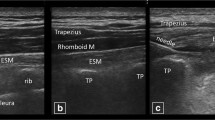
From admission to the ER until transferring to the OR, the patient received ten PRBC units and eight FFP units which makes Hb level to 8.9 mg/dL and INR to 1.26. In the OR, the patient was awake. However, she could not tolerate the supine position and refused general anesthesia. The patient’s oxygenation had been supported by a flow of 5–6 L/min of 100% oxygen via a face mask. After obtaining consent from the patient and coordinating with the surgeon, it was decided to perform ESPB on the left side via sitting position. Standard monitoring was established in addition to an arterial line obtained under local anesthesia. The tip of the scapula was identified as T7 and ultrasound-guided ESPB with an in-plane approach and high frequency linear transducer (Sonosite Edge II ultrasound machine 6–13 MHz) was performed by injecting 20 ml of Ropivacaine 0.5% in the fascia between the erector spinae muscle and the transverse processes of the 5th thoracic vertebrae. Then, 20 mg of intravenous ketamine was administrated. After 20 min, the thoracotomy incision site was checked by the pinprick test after ensuring sufficient analgesia, the patient was placed in the semi-lateral semi-sitting position. Limited left-side thoracotomy via 5th and 6th intercostal space between midaxillary and midclavicular lines with a length of 10 cm was performed. After that, a pericardiectomy was conducted, 200 mL of loculated serous fluid was removed, a water seal drainage was embedded, and the chest wall was sutured again. In all stages, the patient had complete anesthesia, and her hemodynamics were stable.
If, for any reason, the ESBP failed, plan B was to put the patient under general anesthesia, maintaining spontaneous breathing and avoiding positive pressure ventilation (PPV) until the removal of tamponade. Ketamine was intended as an induction agent. In case of insufficient spontaneous breathing, the plan was to use low volumes of mechanical ventilation. Inotropes and vasopressors were also available. Anesthesia was supposed to be maintained with an anesthetic balance technique using inhaled anesthetics and short-acting narcotics.
The patient was kept under observation for a while and then transferred to the cardiac surgery intensive care unit (ICU) to ensure proper recovery. The patient received no analgesic agent during the first 6 h post-surgery.
The drainage was removed on the 7th day of ICU admission, and the patient was transferred to the general ward. After 23 days of hospitalization, the patient was discharged with a satisfactory recovery, and no further complications were noted.
Discussion
The first choice of anesthesia for thoracotomy is almost always general anesthesia [3, 4]. However, the patient neither tolerated nor consented to that. The epidural, paravertebral, or intercostal nerve blocks are generally used for perioperative analgesia or to reduce the dosage of anesthetics [5, 6]. However, an altered INR is the most crucial contraindication for a central block. In addition, in the epidural technique, blocking the sympathetic chain may alter the patient’s hemodynamic, however, this was contraindicated due to her unstable presentation upon arrival to the OR.
Hence, peripheral blocks, including paravertebral block, serratus plane block (SPB), and ESPB, may be favored options in these conditions. In the paravertebral approach, albeit lower than the epidural, there is still a chance of distributing to the epidural area and causing further hemodynamic instability [7]. Intercostal nerve blocks needed multiple needling [8], which may not be a good choice in this anxious patient who had an altered INR and coagulopathy. A systematic review and meta-analysis by KOO et al. revealed that although ESPB is less efficient than paravertebral block, it is preferable to SPB [9].
We decided to apply ESPB as a peripheral block approach, which was performed by just one needle insertion far from the epidural space. Meanwhile, a higher concentration of local anesthetic was administered to achieve proper anesthesia at the surgery site.
ESPB is a regional analgesia technique that targets the dorsal and ventral rami of spinal nerve roots. It is a less invasive option due to the avoidance of the neuraxial and paravertebral spaces. Furthermore, it is a safe technique used in various surgical interventions [6, 10].
ESPB has been extensively used in perioperative pain management for adults and pediatric patients undergoing thoracotomy [11, 12]. Intermittent or continuous ESPB was also conducted [13, 14]. The evidence revealed that applying ESPB leads to decreasing intraoperative and postoperative opioid use [15]. However, ESBP is not a routine anesthetic technique and has been rarely reported to be used in this regard [16,17,18,19,20]. This case report presents a successful course of applying ESBP for conducting thoracotomy.
Conclusion
Using ESPB with a higher concentration of local anesthetics, in this case, prepared appropriate anesthesia for performing an emergency thoracotomy while avoiding multiple needle insertions and the risk of further hemodynamic instability.
Availability of data and materials
All data related to this case report are contained within the manuscript.
References
Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block: a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41(5):621–7.
Tsui BC, Fonseca A, Munshey F, McFadyen G, Caruso TJ. The erector spinae plane (ESP) block: a pooled review of 242 cases. J Clin Anesth. 2019;53:29–34.
Eldawlatly A, Turkistani A, Shelley B, El-Tahan M, Macfie A, Kinsella J, et al. Anesthesia for thoracic surgery: a survey of middle eastern practice. Saudi J Anaesth. 2012;6(3):192.
Shelley B, Macfie A, Kinsella J. Anesthesia for thoracic surgery: a survey of UK practice. J Cardiothorac Vasc Anesth. 2011;25(6):1014–7.
Wenk M, Schug SA. Perioperative pain management after thoracotomy. Curr Opin Anesthesiol. 2011;24(1):8–12.
Pascarella G, Costa F, Nonnis G, Strumia A, Sarubbi D, Schiavoni L, et al. Ultrasound guided parasternal block for perioperative analgesia in cardiac surgery: a prospective study. J Clin Med. 2023;12(5): 2060.
Norum HM, Breivik H. A systematic review of comparative studies indicates that paravertebral block is neither superior nor safer than epidural analgesia for pain after thoracotomy. Scand J Pain. 2010;1(1):12–23.
Schiavoni L, Nenna A, Cardetta F, Pascarella G, Costa F, Chello M, et al. Parasternal intercostal nerve blocks in patients undergoing cardiac surgery: evidence update and technical considerations. J Cardiothorac Vasc Anesth. 2022;36(11):4173–82.
Koo C-H, Lee H-T, Na H-S, Ryu J-H, Shin H-J. Efficacy of erector spinae plane block for analgesia in thoracic surgery: a systematic review and meta-analysis. J Cardiothorac Vasc Anesth. 2022;36(5):1387–95.
Mirkheshti A, Raji P, Komlakh K, Salimi S, Shakeri A. The efficacy of ultrasound-guided erector spinae plane block (ESPB) versus freehand ESPB in postoperative pain management after lumbar spinal fusion surgery: a randomized, non-inferiority trial. Eur Spine J. 2024. https://doi.org/10.1007/s00586-023-08101-9. Online ahead of print.
Mossad E, Chung E. 131 Erector spinae block for perioperative pain management in children undergoing thoracotomy. Reg Anesth Pain Med. 2021;70(Suppl 1):A69-A.
Chin KJ, Adhikary SD, Forero M. Erector Spinae plane (ESP) block: a new paradigm in regional anesthesia and analgesia. Curr Anesthesiol Rep. 2019;9:271–80.
Piraccini E, Biondi G, De Lorenzo E, Corso RM, Maitan S. Ultrasound-guided erector spinae block for post-thoracotomy pain syndrome in video-assisted thoracic surgery. Tumori J. 2020;106(6):NP46–8.
Krishna SN, Chauhan S, Bhoi D, Kaushal B, Hasija S, Sangdup T, et al. Bilateral erector spinae plane block for acute post-surgical pain in adult cardiac surgical patients: a randomized controlled trial. J Cardiothorac Vasc Anesth. 2019;33(2):368–75.
Pallu I, Boscoli SDS, Zaleski T, Andrade DPD, Cherubini GRL, Czepula AIDS, et al. Evaluation of pain and opioid consumption in local preemptive anesthesia and the erector spine plane block in thoracoscopic surgery: a randomized clinical trial. Rev Col Bras Cir. 2022;49:e20223291.
Pereira AM, Teixeira FM, Sampaio JP, Vieira MSRM. 93 instrumented lumbar spine surgery under spinal anesthesia and erector spinae block in a stage IV lung cancer patient–a case-report. Reg Anesth Pain Med. 2021;70(Suppl 1):A50-A.
Kimachi PP, Martins EG, Peng P, Forero M. The erector spinae plane block provides complete surgical anesthesia in breast surgery: a case report. A&A Pract. 2018;11(7):186–8.
Kang TH, Kim WJ, Lee JH. Efficacy of the erector spinae plane block with sedation for unilateral biportal endoscopic spine surgery and comparison with other anesthetic methods. Acta Neurochir (Wien). 2023;165(9):2651–63.
Kaya C, Dost B, Tulgar S. Sacral erector spinae plane block provides surgical anesthesia in ambulatory anorectal surgery: two case reports. Cureus. 2021;13(1):e12598.
Ahiskalioglu A, Tulgar S, Celik M, Ozer Z, Alici HA, Aydin ME. Lumbar Erector Spinae Plane Block as a Main Anesthetic Method for hip surgery in High Risk Elderly patients: initial experience with a magnetic resonance imaging. Eurasian J Med. 2020;52(1):16–20.
Acknowledgements
We would like to thank all the anesthesiology department staff of Imam Hosein Hospital who helped manage this patient.
Funding
None.
Author information
Authors and Affiliations
Contributions
A.S. and E.M. have contributed to the patient’s management, drafting/revising the manuscript, and the study concept. A.S. and E.M. declared their accountability for all parts of the article.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of the Shahid Beheshti University of Medical Sciences (SBMU) under the ethics code IR.SBMU.RETECH.REC.1402.423.
Consent for publication
A written informed consent was obtained from the patient to publish identifying information in an online open-access publication.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shakeri, A., Memary, E. Erector spinae plane block as an anesthesia technique for an emergent thoracotomy; a case report. BMC Anesthesiol 24, 57 (2024). https://doi.org/10.1186/s12871-024-02431-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-024-02431-x