
Abstract
Background
Based on the controversy surrounding pulmonary artery catheterization (PAC) in surgical patients, we investigated the interchangeability of cardiac index (CI) and systemic vascular resistance (SVR) measurements between ClearSight™ and PAC during living-donor liver transplantation (LDLT).
Methods
This prospective study included consecutively selected LDLT patients. ClearSight™-based CI and SVR measurements were compared with those from PAC at seven LDLT-stage time points. ClearSight™-based systolic (SAP), mean (MAP), and diastolic (DAP) arterial pressures were also compared with those from femoral arterial catheterization (FAC). For the comparison and analysis of ClearSight™ and the reference method, Bland-Altman analysis was used to analyze accuracy while polar and four-quadrant plots were used to analyze the trending ability.
Results
From 27 patients, 189 pairs of ClearSight™ and reference values were analyzed. The CI and SVR performance errors (PEs) exhibited poor accuracy between the two methods (51.52 and 51.73%, respectively) in the Bland-Altman analysis. CI and SVR also exhibited unacceptable trending abilities in both the polar and four-quadrant plot analyses. SAP, MAP, and DAP PEs between the two methods displayed favorable accuracy (24.28, 21.18, and 26.26%, respectively). SAP and MAP exhibited acceptable trending ability in the four-quadrant plot between the two methods, but not in the polar plot analyses.
Conclusions
During LDLT, CI and SVR demonstrated poor interchangeability, while SAP and MAP exhibited acceptable interchangeability between ClearSight™ and FAC.
Similar content being viewed by others
Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Hemodynamic instability frequently occurs during liver transplantation due to its surgical features, which include massive bleeding, manipulations of major vessels, and reperfusion of liver graft, as well as the recipient’s features, such as reduced systemic vascular resistance (SVR) and ventricular response [1]. Therefore, pulmonary artery catheterization (PAC) for continuous hemodynamic monitoring has traditionally been used in liver transplantation [2, 3]. However, PAC is an invasive procedure that potentially causes severe complications during its insertion or maintenance, such as pulmonary artery injury and ventricular arrhythmia [4]. Thus, its utility in surgical patients remains controversial, requiring a less-invasive hemodynamic monitoring method [5,6,7,8].
Several non-invasive hemodynamic monitoring techniques have been studied in various perioperative settings [9, 10]. In liver transplantation, several comparative studies have compared non-invasive cardiac output (CO) monitoring with thermodilution measurement via a PAC; however, these studies failed to yield satisfactory accuracy [11,12,13,14,15]. ClearSight™ (Edwards Lifesciences, Irvine, CA, USA) is a continuous, non-invasive finger-cuff arterial pressure monitoring device that uses photoplethysmographic technology [16] and enables the continuous measurement of CO through arterial pulse waveform analysis [9, 10, 16]. Previous studies have reported that finger arterial pulse analysis displays clinically acceptable interchangeability with conventional invasive hemodynamic monitoring in cardiac surgery and intensive care [17,18,19].
However, in liver transplantation, the interchangeability between ClearSight™ and conventional invasive hemodynamic monitoring has not yet been reported. Thus, we aimed to investigate their interchangeability by comparing hemodynamic variables, such as the cardiac index (CI), SVR, and blood pressure, obtained from ClearSight™ with those from conventional invasive hemodynamic monitoring via PAC and femoral arterial catheterization (FAC) during liver transplantation. We expect our results from liver transplantation to also provide valuable information regarding the usefulness of ClearSight™ in other major surgeries that are potentially complicated by hemodynamic instability.
Methods
Patients
This single-center, prospective, observational study was approved by our institutional review board (IRB No.2104-037-1209) and registered on the ClinicalTrials registry (NCT04909645; date of registration: 02/06/2021). This study was conducted in accordance with the principles of the 2013 Helsinki Declaration and followed good clinical practice guidelines. Patients who underwent scheduled living-donor liver transplantation (LDLT) were enrolled consecutively between May and December 2021. All patients received both verbal and written explanations of the trial and provided written informed consent. We excluded patients with persistent arrhythmias and a history of upper-extremity artery occlusion. Patients who had a perm catheter in the right internal jugular vein as well as contraindications for PAC [4], such as right-sided endocarditis, tumors, right-sided valve disease, and left bundle branch block, were also excluded.
Anesthetic management
After routine vital monitoring, general anesthesia was induced using a bolus injection of propofol (1.0–2.0 mg/kg) and a target-controlled infusion of remifentanil. Tracheal intubation was performed following adequate muscle relaxation achieved through the administration of rocuronium (1.2 mg/kg). Subsequently, volume-controlled ventilation was initiated at a tidal volume ranging from 6 to 8 mL/kg without the use of positive end-expiratory pressure while maintaining a fraction of inspiratory oxygen between 0.4 and 0.6. Anesthesia was maintained using sevoflurane and remifentanil. After inserting a 31-mm 20-gauge catheter (SuperCath™ 5, Medikit Co., Ltd., Tokyo, Japan) into the right radial artery, continuous arterial pressure monitoring was initiated, and a ClearSight™ monitor (Edwards Lifesciences, Irvine, CA, USA) was attached to the ipsilateral middle finger to measure CO and blood pressure using an EV1000™ monitor (Edwards Lifesciences, Irvine, CA, USA). Additionally, femoral arterial pressure monitoring was initiated after inserting a 3-French 8-cm catheter (Arterial Leader Cath, Vygon, Ecouen, France) into the right femoral artery. A pulmonary artery (PA) catheter (Swan Ganz CCOmbo CCO/SvO2™; Edward Lifesciences LLC, Irvine, CA, USA) was inserted through the right internal jugular vein. The tip of the PA catheter was confirmed to be correctly positioned in lung zone 3 using the pulmonary artery waveform, with the PA wedge pressure lower than the PA diastolic pressure. In addition, chest radiography was taken after the anesthetic induction. The PA catheter was connected to a Vigilance™ hemodynamic monitor (Edwards Lifesciences) to measure central venous pressure (CVP), CO, and CI. The pressure transducers (ClearSight™, pulmonary artery, CVP, femoral artery, radial artery) were zero-referenced to the right heart level. The ClearSight™ underwent auto-repeated self-calibration, while the Vigilance™ system was calibrated through pulmonary arterial blood sampling after confirming the PA catheter’s placement. And a fast flush test was conducted at 10-minute intervals to assess the quality of the femoral and radial arterial waveforms. Based on the attending anesthesiologist’s judgment, vasopressors (ephedrine, epinephrine, phenylephrine, vasopressin, and norepinephrine) were administered to maintain a femoral mean arterial pressure (MAP) of 65 mmHg or higher during the entire intraoperative period. Red blood cells were transfused to maintain a hemoglobin level > 8 g/dL. Fresh frozen plasma, platelets, and cryoprecipitate were transfused based on the rotational thromboelastometry results.
CI, SVR, and blood pressure reference values
CI measurement via the pulmonary artery thermodilution technique using a bolus injection of cold saline has not been implemented for over 20 years in our institution. Instead, continuous CI monitoring using a modified PAC with a heated filament has been used [20]. Therefore, we used the latter to obtain reference values for the CI and femoral arterial pressure (Fig. 1A), which is a more reliable blood pressure measure than radial arterial pressure during liver transplantation [3, 21]. The SVR reference value was calculated using the CVP value obtained from PAC and the MAP obtained from FAC (Fig. 1A).

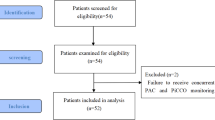
(a) The study protocol. (b) Flow diagram of the study. PAC; pulmonary artery catheterization, FAC; femoral artery catheterization; CI, cardiac index; SVR, systemic vascular resistance; SAP, systolic arterial pressure; MAP, mean arterial pressure; DAP, diastolic arterial pressure
Data collection
Based on the liver transplantation stage [22], each hemodynamic variable obtained from the reference method and ClearSight™ was recorded at the following seven time points (Fig. 1A): T1 (preanhepatic 1), induction complete; T2 (preanhepatic 2), 60 min after T1; T3 (anhepatic 1), 10 min after completion of recipient hepatectomy; T4 (anhepatic 2), 10 min after inferior vena cava (IVC) clamping; T5 (reperfusion), 5 min after reperfusion; T6 (neo-hepatic 1): 20 min after reperfusion; and T7 (neo-hepatic 2): 1 h after reperfusion. Continuous infusion of vasopressor and core temperature, which potentially affect the accuracy of finger arterial pulse analysis, were also recorded at each time point [23].
Statistical analysis
Based on previous studies on the accuracy of ClearSight™-derived CI in other surgeries [24, 25], we aimed to recruit a total of 30 patients, assuming a 10% dropout rate.
Bland–Altman analysis [26] was used to compare measured values between the reference method and ClearSight™, and the results are shown with bias and a 95% limit of agreement. The reference values for the CI and SVR were calculated using values obtained from PAC, and those for systolic arterial pressure (SAP), MAP, and diastolic arterial pressure (DAP) were those measured from FAC. Percentage error (PE) was calculated using Critchley and Critchley’s formula (1.96 × standard deviation/mean); for PEs < 30%, ClearSight™ was considered interchangeable with the reference method [27, 28]. The limits of agreement were calculated by reflecting the data measured several times from one patient [29].
Trending ability was analyzed using polar and four-quadrant plots [27, 28, 30]. In the four-quadrant plot, the horizontal axis was divided into four zones based on the change in value from the reference method, and the vertical axis reflected the change in value from ClearSight™. A correct quadrant was defined as a case wherein both the value obtained from the reference method and that from ClearSight™ were positive or negative (the upper-right and lower-left quadrants), and the exclusion zone was set at 0.3 L/min/m2 for the CI and 10% for SAP, MAP, and DAP [11]. The concordance rate was calculated as the proportion of the correct quadrant across all points, and concordance rates > 92% were considered clinically acceptable [27]. In the polar plot analysis, the angle from the line of identity (y = x) and magnitude of change by vector length reflected the agreement between the two methods [30]. The values are presented as the mean angle bias and radial limits of agreement. When the angular bias was less than ± 5 and radial limits of agreement less than ± 30°, the trending ability was considered acceptable [28, 30].
R (version 4.1.1 with R packages; R development Core Team, Vienna, Austria) using the moonBook package [31], and SAS (version 9.4; SAS Institute, Cary, US) software were used for all statistical analyses. A two-sided P value < 0.05 was considered to have statistical significance.
Results
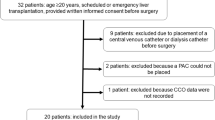
A total of 30 patients were enrolled in this study, and 189 measurements from 27 patients were included in the final analysis (Fig. 1B). Data from three patients were excluded from the analysis due to the following reasons: cancellation of surgery due to ST-segment elevation revealed after anesthetic induction, failed PAC due to repetitive arrhythmia, and the occurrence of intraoperative cardiac arrest during the preanhepatic phase. The baseline characteristics and perioperative variables are shown in Table 1. The percentage of patients with intraoperative norepinephrine infusion was 93.6% (26/27). None of the patients received epinephrine, vasopressin, or phenylephrine during the operation.
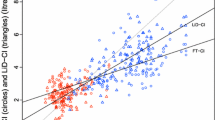
The Bland–Altman analyses are shown in Fig. 2. The bias and 95% limits of agreement between the CIs from PAC and those from ClearSight™ were 0 L/min/ m2 and − 1.70 to 1.70, and those between the SVRs from PAC and those from ClearSight™ were − 48.87 dyne.s/cm5 and − 708.08 to 610.35, respectively. The PEs of the CI and SVR exhibited poor accuracy (51.52% and 51.73%, respectively) (Table 2). The PEs of ClearSight™ for blood pressure measured at the femoral artery were 24.28%, 21.18%, and 26.26% for SAP, MAP, and DAP, respectively (Table 3; Fig. 2), indicating favorable accuracy.

(a) Bland–Altman analysis comparing the CI measured using ClearSight™ with that using PAC, showing multiple measurements per subject. (b) Bland–Altman analysis comparing SVR measured using ClearSight™ with that using PAC, showing multiple measurements per subject. (c) Bland–Altman analysis comparing SAP measured using ClearSight™ with that using FAC, showing multiple measurements per subject. (d) Bland–Altman analysis comparing MAP measured using ClearSight™ with that using FAC, showing multiple measurements per subject. (e) Bland–Altman analysis comparing DAP measured using ClearSight™ with that using FAC, showing multiple measurements per subject. The blue line indicates the mean bias, and the dashed lines indicate the 95% limits of agreement in each analysis. CI, cardiac index; PAC, pulmonary artery catheterization; SVR, systemic vascular resistance; SAP, systolic arterial pressure; MAP, mean arterial pressure; DAP, diastolic arterial pressure, FAC; femoral artery catheterization; SD, standard deviation
Four-quadrant plot and polar plot analyses were used to evaluate the trending ability of ClearSight™ for each reference method. In the four-quadrant plot analysis, the concordance rates of the CI and SVR measured between the two methods were 66.91% and 79.74%, respectively, exhibiting poor trending ability (Fig. 3). Similarly, the mean angular bias values (a radial limit of agreement) of the CI and SVR in the polar plot analysis were − 12° (74°) and − 5° (64°), respectively (Fig. 4). The concordance rates of SAP, MAP, and DAP between the two methods in the four-quadrant plot analysis were 92.62%, 93.55%, and 47.86%, respectively (Fig. 3). In the polar plot analysis, the mean angular bias values (a radial limit of agreement) of SAP, MAP, and DAP were 8° (47°), 1° (35°), and − 12° (83°), respectively (Fig. 4).

(a) Four-quadrant plot showing the concordance in the change in CI between ClearSight™ and PAC. (b) Four-quadrant plot showing the concordance in the change in SVR between ClearSight™ and PAC. (c) Four-quadrant plot showing the concordance in the change in SAP between ClearSight™ and FAC. (d) Four-quadrant plot showing the concordance in the change in MAP between ClearSight™ and FAC. (e) Four-quadrant plot showing the concordance in the change in DAP between ClearSight™ and FAC. The concordance rate was defined as the percentage of data points in which the change in the CI, SVR, SAP, MAP, and DAP of both methods goes in the same direction. The gray rectangle indicates the exclusion zone of 10%. CI, cardiac index; PAC, pulmonary artery catheterization; SVR, systemic vascular resistance; SAP, systolic arterial pressure; MAP, mean arterial pressure; DAP, diastolic arterial pressure; FAC; femoral artery catheterization

(a) Polar plots for examining the trending ability of CI change measured using ClearSight™ and PAC. (b) Polar plots for examining the trending ability of SVR change measured using ClearSight™ and PAC. (c) Polar plots for examining the trending ability of SAP change measured using ClearSight™ and FAC. (d) Polar plots for examining the trending ability of MAP change measured using ClearSight and FAC. (e) Polar plots for examining the trending ability of DAP change measured using ClearSight™ and FAC. CI, cardiac index; PAC, pulmonary artery catheterization; SVR, systemic vascular resistance; SAP, systolic arterial pressure; MAP, mean arterial pressure; DAP, diastolic arterial pressure; FAC; femoral artery catheterization
Discussion
This study failed to demonstrate clinically acceptable interchangeability of CI and SVR between ClearSight™ and the continuous thermodilution method using a PA catheter with a heating filament during liver transplantation. SAP and MAP estimated using ClearSight™ displayed favorable accuracy compared with those measured using FAC and exhibited acceptable trending ability in the four-quadrant plot analysis. To the best of our knowledge, this study is the first to compare continuous hemodynamic monitoring between ClearSight™ and conventional invasive hemodynamic monitoring methods in liver transplantation.
PAC has been used as a therapeutic intervention for monitoring several hemodynamic parameters in high-risk surgical patients [32]. It has also been established as a routine practice in liver transplantation [33]. However, due to the development of less-invasive hemodynamic monitors and the risk of fatal complications associated with PAC [34], the usefulness of PAC in high-risk surgeries has recently been debated [34]. A recent retrospective study reported no difference in postoperative outcomes between hemodynamic management via PAC and arterial waveform analysis (Flotrac/Vigileo monitoring) in patients undergoing liver transplantation [35]. In a recent survey conducted by the Society for the Advancement of Transplant Anesthesia, approximately half of the anesthesiologists in high-volume centers indicated that < 50% of liver transplantation requires PAC [36]. Additionally, this survey reported a decreased routine use of PAC in liver transplantation compared with previous surveys [36]. On this premise, we attempted to investigate the interchangeability between ClearSight™ and PAC in this study.
Here, ClearSight™ did not exhibit clinically acceptable interchangeability with PAC in terms of CO and SVR. Similarly, previous studies have also reported poor interchangeability in the CI and SVR between PAC and other less-invasive arterial pulse wave analyses during liver transplantation [14, 15, 37]. Patients with cirrhosis undergoing liver transplantation possess unique characteristics, such as hyperdynamic circulation and low SVR, which potentially increase the inaccuracy of arterial pulse wave analysis [15, 38, 39]. Additionally, rapid changes in hemodynamic status during liver transplantation occur due to massive bleeding, manipulation of the IVC, inflammatory mediators after reperfusion of the graft, and the common use of vasoactive drugs that affect vascular compliance, thus negatively affecting the accuracy of arterial pulse wave analysis, including ClearSight™ [1, 3, 22]. Hypothermia, which is common during liver transplantation, also might have affected the accuracy of these methods [19, 39]. The point at which CO in ClearSight™ was calculated using the algorithm based on patient-related variables (age, sex, height, and weight) from the estimated blood pressure curve also might have affected the results [40]. Therefore, ClearSight™ would have failed to exhibit acceptable interchangeability in liver transplantation.
In addition to CO and SVR, we investigated the interchangeability of blood pressure measurements between ClearSight™ and FAC. Previous studies have predominantly investigated the interchangeability between ClearSight™ and radial arterial pressure [16, 24, 25, 37]. However, to our best knowledge, none have investigated the interchangeability between ClearSight™ and FAC-derived central arterial pressure in surgical patients. A recent prospective study using finger arterial pulse contour analysis reported a strong correlation between it and FAC-derived blood pressure in intensive care unit patients [41]. Our results demonstrate acceptable congruence of SAP, MAP, and DAP between ClearSight™ and FAC as well as an acceptable trending ability of SAP and MAP estimated using the four-quadrant plot. Although the polar plot analysis results did not satisfy predefined acceptable criteria, controversy regarding the superiority of the four-quadrant or polar plot analysis persists [42]. Since femoral arterial pressure is more reliable in blood pressure assessment than radial arterial pressure in critically ill patients [43], the favorable agreement and trending ability between ClearSight™ and femoral arterial pressure potentially indicate its usefulness in blood pressure monitoring in high-risk surgical patients. Additionally, since ClearSight™ displayed clinically acceptable interchangeability of MAP even in liver transplantation complicated by hemodynamic instability, our results potentially support the usefulness of ClearSight™ as a reliable pressure monitor in other high-risk surgeries.
This study has a few limitations. First, the time interval for CO measurement differed between ClearSight™ and PAC (20 s and 1 min, respectively). Therefore, each method might have presented values from different time points. In addition, since hemodynamic fluctuation in liver transplantation is common, the time delay between them might have negatively affected the consistency between the two methods [44]. Second, we could not conduct an a priori sample size calculation. An estimate of the study subjects’ CI was required to calculate the appropriate number of subjects in this study [45]; however, it was difficult to estimate due to severe hemodynamic instability in liver transplantation patients. Moreover, the distinctive characteristics of living donor liver transplantation posed challenges in recruiting a large number of patients, thereby necessitating the execution of this study on a small sample size. Nevertheless, despite the limitations in sample size, this study provides valuable insights into the feasibility of noninvasive methods for patients with hyperdynamic circulation during liver transplantation. Third, inotrope and vasopressor infusion at each time point was not considered. These drugs could have influenced the pulse contour analysis [5]. Fourth, our study predominantly focused on the interchangeability of CI, SVR, and AP estimations between ClearSight™ and conventional invasive hemodynamic monitors. Therefore, the advantages of conventional invasive hemodynamic monitoring, such as pulmonary arterial wedge pressure via PAC and arterial blood gas analysis via FAC, were not considered in this study. Finally, although the usefulness of transesophageal echocardiography (TEE) has been reported in liver transplantation [3], TEE results were not included in this study because TEE monitoring is used selectively in hemodynamic monitoring during liver transplantation in our institution.
In conclusion, ClearSight™ failed to demonstrate clinically acceptable interchangeability of CI and SVR estimations with the transpulmonary thermodilution method in LDLT. Therefore, continuous CI and SVR measurements using ClearSight™ cannot replace those using PAC in liver transplantation.
Data Availability
The datasets generated during and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CI:
-
Cardiac index
- CVP:
-
Central venous pressure
- FAC:
-
Femoral arterial catheterization
- LDLT:
-
Living-donor liver transplantation
- MAP:
-
Mean arterial pressure
- PAC:
-
Pulmonary artery catheterization
- SVR:
-
Systemic vascular resistance
References
Beinover D, Mukhtar A, Wagener G, Wray C, Blasi A, Kronish K, et al. Hemodynamic instability during liver transplantation in patients with end-stage liver disease: a Consensus Document from ILTS, LICAGE, and SATA. Transplantation. 2021;105:2184–200.
De Wolf AM. 6/2/06 perioperative assessment of the cardiovascular system in ESLD and transplantation. Int Anesthesiol Clin. 2006;44:59–78.
Rudnick MR, Marchi LD, Plotkin JS. Hemodynamic monitoring during liver transplantation: a state of the art review. World J Hepatol. 2015;7:1302–11.
Evans DC, Doraiswamy VA, Prosciak MP, Silviera M, Seamon MJ, Rodriguez Funes V, et al. Complications associated with pulmonary artery catheters: a comprehensive clinical review. Scand J Surg. 2009;98:199–208.
Mehta Y, Arora D. Newer methods of cardiac output monitoring. World J Cardiol. 2014;6:1022–9.
Bender JS, Smith-Meek MA, Jones CE. Routine pulmonary artery catheterization does not reduce morbidity and mortality of elective vascular surgery: results of a prospective, randomized trial. Ann Surg. 1997;226:229–36. discussion 236-7.
Ramsey SD, Saint S, Sullivan SD, Dey L, Kelley K, Bowdle A. Clinical and economic effects of pulmonary artery catheterization in nonemergent coronary artery bypass graft surgery. J Cardiothorac Vasc Anesth. 2000;14:113–8.
Brown JA, Aranda-Michel E, Kilic A, Serna-Gallegos D, Bianco V, Thoma FW, et al. The impact of pulmonary artery catheter use in cardiac surgery. J Thorac Cardiovasc Surg. 2022;164(6):1965–73e6.
Saugel B, Cecconi M, Wagner JY, Reuter DA. Noninvasive continuous cardiac output monitoring in perioperative and intensive care medicine. Br J Anaesth. 2015;114:562–75.
Saugel B, Hoppe P, Nicklas JY, Kouz K, Körner A, Hempel JC, et al. Continuous noninvasive pulse wave analysis using finger cuff technologies for arterial blood pressure and cardiac output monitoring in perioperative and intensive care medicine: a systematic review and meta-analysis. Br J Anaesth. 2020;125:25–37.
Suparschi V, Le Bihan E, Toussaint A, Saptefrat D, Ben Abdallah H, Gloulou F, et al. Noninvasive assessment of Cardiac Index using impedance cardiography during liver transplantation surgery: a comparison with pulmonary artery thermodilution. Minerva Anestesiol. 2019;85:28–33.
Magliocca A, Rezoagli E, Anderson TA, Burns SM, Ichinose F, Chitilian HV. Cardiac output measurements based on the pulse Wave Transit Time and thoracic impedance exhibit Limited Agreement with Thermodilution Method during Orthotopic Liver Transplantation. Anesth Analg. 2018;126:85–92.
Wang DJ, Lee IS, Chou AH, Chen CY, Ting PC, Teng YH, et al. Non-invasive cardiac output measurement with electrical velocimetry in patients undergoing liver transplantation: comparison of an invasive method with pulmonary thermodilution. BMC Anesthesiol. 2018;18:138.
Lee M, Weinberg L, Pearce B, Scurrah N, Story DA, Pillai P, et al. Agreement in hemodynamic monitoring during orthotopic liver transplantation: a comparison of FloTrac/Vigileo at two monitoring sites with pulmonary artery catheter thermodilution. J Clin Monit Comput. 2017;31:343–51.
Murata Y, Imai T, Takeda C, Mizota T, Kawamoto S. Agreement between continuous cardiac output measured by the fourth-generation FloTrac/Vigileo system and a pulmonary artery catheter in adult liver transplantation. Sci Rep. 2022;12:11198.
Ameloot K, Palmers PJ, Malbrain ML. The accuracy of noninvasive cardiac output and pressure measurements with finger cuff: a concise review. Curr Opin Crit Care. 2015;21:232–9.
Broch O, Renner J, Gruenewald M, Meybohm P, Schöttler J, Caliebe A, et al. A comparison of the Nexfin® and transcardiopulmonary thermodilution to estimate cardiac output during coronary artery surgery. Anaesthesia. 2012;67:377–83.
Stover JF, Stocker R, Lenherr R, Neff TA, Cottini SR, Zoller B, et al. Noninvasive cardiac output and blood pressure monitoring cannot replace an invasive monitoring system in critically ill patients. BMC Anesthesiol. 2009;9:6.
Bogert LW, Wesseling KH, Schraa O, Van Lieshout EJ, de Mol BA, van Goudoever J, et al. Pulse contour cardiac output derived from non-invasive arterial pressure in cardiovascular disease. Anaesthesia. 2010;65:1119–25.
Zöllner C, Polasek J, Kilger E, Pichler B, Jaenicke U, Briegel J, et al. Evaluation of a new continuous thermodilution cardiac output monitor in cardiac surgical patients: a prospective criterion standard study. Crit Care Med. 1999;27:293–8.
Krenn CG, De Wolf AM. Current approach to intraoperative monitoring in liver transplantation. Curr Opin Organ Transplant. 2008;13:285–90.
Fabbroni D, Bellamy M. Anaesthesia for hepatic transplantation. BJA Educ. 2006;6:171–5. https://doi.org/10.1093/bjaceaccp/mkl040.
Saugel B, Kouz K, Scheeren TWL, Greiwe G, Hoppe P, Romagnoli S, et al. Cardiac output estimation using pulse wave analysis-physiology, algorithms, and technologies: a narrative review. Br J Anaesth. 2021;126:67–76.
Kanazawa H, Maeda T, Miyazaki E, Hotta N, Ito S, Ohnishi Y. Accuracy and trending ability of blood pressure and Cardiac Index measured by ClearSight System in patients with reduced ejection fraction. J Cardiothorac Vasc Anesth. 2020;34:3293–9.
Sumiyoshi M, Maeda T, Miyazaki E, Hotta N, Sato H, Hamaguchi E, et al. Accuracy of the ClearSight™ system in patients undergoing abdominal aortic aneurysm surgery. J Anesth. 2019;33:364–71.
Bland JM, Altman DG. Agreement between methods of measurement with multiple observations per individual. J Biopharm Stat. 2007;17:571–82.
Critchley LA, Lee A, Ho AM. A critical review of the ability of continuous cardiac output monitors to measure trends in cardiac output. Anesth Analg. 2010;111:1180–92.
Critchley LA, Critchley JA. A meta-analysis of studies using bias and precision statistics to compare cardiac output measurement techniques. J Clin Monit Comput. 1999;15:85–91.
Zou GY. Confidence interval estimation for the Bland-Altman limits of agreement with multiple observations per individual. Stat Methods Med Res. 2013;22:630–42.
Critchley LA, Yang XX, Lee A. Assessment of trending ability of cardiac output monitors by polar plot methodology. J Cardiothorac Vasc Anesth. 2011;25:536–46.
Moon K. (2015). R statistics and graphs for medical papers. Hannarae Seoul. ISBN 978-89-5566-179-8.
Gidwani UK, Goel S. The pulmonary artery catheter in 2015: the Swan and the Phoenix. Cardiol Rev. 2016;24:1–13.
Schumann R, Mandell MS, Mercaldo N, Michaels D, Robertson A, Banerjee A, et al. Anesthesia for liver transplantation in United States academic centers: intraoperative practice. J Clin Anesth. 2013;25:542–50.
Navas-Blanco JR, Vaidyanathan A, Blanco PT, Modak RK. CON: pulmonary artery catheter use should be forgone in modern clinical practice. Ann Card Anaesth. 2021;24:8–11.
Villa AM, Pagano M, Fallabrino G, Piccioni F, Manzi RC, Codazzi D et al. Comparison Between Swan-Ganz Catheter and Minimally Invasive Hemodynamic Monitoring During Liver Transplantation: Report of a Monocentric Case Series. Transplant Proc. 2019;51:2943-7.
Crouch C, et al. Adult liver transplant anesthesiology practice patterns and resource utilization in the United States: survey results from the society for the advancement of transplant anesthesia. Clin Transpl. 2022;36:e14504. https://doi.org/10.1111/ctr.14504.
Shih BF, Huang PH, Yu HP, Liu FC, Lin CC, Chung PC et al. Cardiac Output Assessed by the Fourth-Generation Arterial Waveform Analysis System Is Unreliable in Liver Transplant Recipients. Transplant Proc. 2016;48:1170-5.
Biancofiore G, Critchley LA, Lee A, Bindi L, Bisà M, Esposito M, et al. Evaluation of an uncalibrated arterial pulse contour cardiac output monitoring system in cirrhotic patients undergoing liver surgery. Br J Anaesth. 2009;102:47–54.
Sakka SG, Kozieras J, Thuemer O, van Hout N. Measurement of cardiac output: a comparison between transpulmonary thermodilution and uncalibrated pulse contour analysis. Br J Anaesth. 2007;99:337–42.
Truijen J, van Lieshout JJ, Wesselink WA, Westerhof BE. Noninvasive continuous hemodynamic monitoring. J Clin Monit Comput. 2012;26:267–78.
Ameloot K, et al. Validation study of Nexfin(R) continuous non-invasive blood pressure monitoring in critically ill adult patients. Minerva Anestesiol. 2014;80:1294–301.
Saugel B, Grothe O, Wagner JY. Tracking changes in Cardiac output: statistical considerations on the 4-Quadrant plot and the Polar plot methodology. Anesth Analg. 2015;121:514–24.
Dorman T, Breslow MJ, Lipsett PA, Rosenberg JM, Balser JR, Almog Y, et al. Radial artery pressure monitoring underestimates central arterial pressure during vasopressor therapy in critically ill surgical patients. Crit Care Med. 1998;26:1646–9.
Kouz K, Michard F, Bergholz A, Vokuhl C, Briesenick L, Hoppe P, et al. Agreement between continuous and intermittent pulmonary artery thermodilution for cardiac output measurement in perioperative and intensive care medicine: a systematic review and meta-analysis. Crit Care. 2021;25:125.
Montenij LJ, Buhre WF, Jansen JR, Kruitwagen CL, de Waal EE. Methodology of method comparison studies evaluating the validity of cardiac output monitors: a stepwise approach and checklist. Br J Anaesth. 2016;116:750–8.
Acknowledgements
We would like to thank the Medical Research Collaborating Center of Seoul National University Hospital for statistical analysis and Editage (www.editage.co.kr) for English language editing.
Funding
This study was supported by a grant from Seoul National University Hospital (No. 0420210520).
Author information
Authors and Affiliations
Contributions
Conceptualization: Lee H-J, Yang S-M.Acquisition of data: Cho H-Y, Hwang IE.Analysis and interpretation of data: Cho H-Y, Lee H-J, Yang S-M.Methodology: Lee H-J, Lee HC, Kim WH.Writing - original draft: Cho H-Y, Lee H-JWriting - review & editing: Lee H-J, Kim WH, Yang S-M.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This single-center, prospective, observational study was approved by our institutional review board (IRB No.2104-037-1209) and registered on the ClinicalTrials registry (NCT04909645; date of registration: 02/06/2021). This study was conducted in accordance with the principles of the 2013 Helsinki Declaration and followed good clinical practice guidelines. Patients who underwent scheduled living-donor liver transplantation (LDLT) were enrolled between May and December 2021. All patients received both verbal and written explanations of the trial and provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Cho, HY., Lee, HJ., Hwang, I.E. et al. Comparison of invasive and non-invasive measurements of cardiac index and systemic vascular resistance in living-donor liver transplantation: a prospective, observational study. BMC Anesthesiol 23, 359 (2023). https://doi.org/10.1186/s12871-023-02302-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-023-02302-x