
Abstract
Purpose
Critically ill patients with sepsis account for significant disease morbidity and healthcare costs. Low muscle mass has been proposed as an independent risk factor for poor short-term outcomes, although its effect on long-term outcomes remains unclear.
Methods
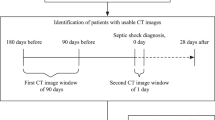
Retrospective cohort analysis of patients treated at a quaternary care medical center over 6 years (09/2014 - 12/2020). Critically ill patients meeting Sepsis-3 criteria were included, with low muscle mass defined by \(\le\) 5th percentile skeletal muscle index, measured at the L3 lumbar level (L3SMI) on Computed-Tomography (CT) scan (\(\le\) 41.6 cm2/m2 for males and \(\le\) 32.0 cm2/m2 for females). L3SMI was calculated by normalizing the CT-measured skeletal muscle area to the square of the patient’s height (in meters). Measurements were taken from abdominal/pelvic CT scan obtained within 7 days of sepsis onset. The prevalence of low muscle mass and its association with clinical outcomes, including in-hospital and one-year mortality, and post-hospitalization discharge disposition in survivors, was analyzed. Unfavorable post-hospitalization disposition was defined as discharge to a location other than the patient’s home.
Results
Low muscle mass was present in 34 (23%) of 150 patients, with mean skeletal muscle indices of 28.0 ± 2.9 cm2/m2 and 36.8 ± 3.3 cm2/m2 in females and males, respectively. While low muscle mass was not a significant risk factor for in-hospital mortality (hazard ratio 1.33; 95% CI 0.64 – 2.76; p = 0.437), it significantly increased one-year mortality after adjusting for age and illness severity using Cox multivariate regression (hazard ratio 1.9; 95% CI 1.1 – 3.2; p = 0.014). Unfavorable post-hospitalization discharge disposition was not associated with low muscle mass, after adjusting for age and illness severity in a single, multivariate model.
Conclusion
Low muscle mass independently predicts one-year mortality but is not associated with in-hospital mortality or unfavorable hospital discharge disposition in critically ill patients with sepsis.
Similar content being viewed by others


Introduction
Sepsis is defined as the life-threatening organ dysfunction that is caused by a dysregulated host response to infection [1]. Particularly adverse clinical outcomes are observed in septic patients who are older than 65 years [2], although advances in critical care therapy have allowed these patients to live longer and experience significant, previously unseen morbidity. The frequent coexistence of sarcopenia and sepsis in older patients has created a need to understand how these conditions interact to influence patient outcomes [3,4,5]. This knowledge may allow clinicians to plan for appropriate rehabilitation and nursing care, early in course of hospitalization in high-risk patients. It may also facilitate discussions by clinicians with patients and their families regarding anticipated disease prognosis and long-term goals of medical care.
Sarcopenia is a syndrome defined by both loss of muscle mass and muscle function [6, 7], the latter being challenging to establish in critically ill patients. Skeletal muscle index, measured at the L3 lumber level of Computer-Tomography images (L3SMI), has therefore been described as a surrogate for sarcopenia [8]. A recent, prospective study of 187 patients confirmed that a low L3SMI significantly correlated with age and mid-arm muscle circumference among males, and was associated with poor survival even after adjusting for age and sex [9]. The use of Computer-Tomography (CT) images to quantify total body skeletal muscle dates back almost two decades [10], although other measures of low muscle mass are being increasingly employed today. Dual energy X-ray absorptiometry [11], magnetic resonance imaging [12], ultrasound [13], and bioelectrical impedance analysis [14] can also be employed for measuring muscle mass. However, accurate measurements of muscle mass together with the wide availability and rapidity of CT imaging makes it particularly well-suited to the care of critically ill patients, who often cannot tolerate prolonged testing.
The first study that investigated the role of muscle mass in septic patients was conducted in 2017, reporting an increased in-hospital mortality in older patients with sepsis and low muscle mass [15]. Several studies conducted since then have been limited by short intervals to patient follow-up [16], as evidenced by a meta-analysis of post-sepsis outcomes in 2396 patients that reported early (in-hospital or 1-month) mortality as the primary measured outcome [17]. This limitation is not insignificant, since much of the disease morbidity related to sepsis occurs in the weeks to months following acute illness [18].
The importance of investigating sarcopenia as an independent risk factor for poor post-septic outcomes is underlined by aging global populations and the resultant demographic profile of those patients who are increasingly seeking healthcare [19]. In the present study, we hypothesized that low muscle mass would adversely predict long-term outcomes in critically ill patients with sepsis. To investigate our hypothesis, we performed a retrospective analysis of critically ill patients meeting Sepsis-3 criteria [1]. Besides one-year mortality as the primary outcome, we investigated the effect of low muscle mass on in-hospital mortality and unfavorable post-hospitalization discharge disposition. We used the latter as a surrogate marker of quality-of-life following patients’ index hospitalization. Specifically, unfavorable discharge disposition was defined as hospital transfer to a long-term rehabilitation or nursing facility, rather than home.
Methods
Study design
This was a single-center, retrospective cohort analysis of patients hospitalized at Penn State Milton S. Hershey Medical Center, a quaternary care medical center, between 09/2014 and 12/2020. Adults aged 18 years and older, who were identified as critically ill based the use of Centers for Medicare and Medicaid Services, Current Procedural Terminology (CPT) codes of 99291 or 99292, and who were diagnosed with sepsis according to the International Classification of Diseases, Ninth Edition, Clinical Modification (ICD-9-CM) sepsis codes were electronically screened for potential inclusion in the study. Patients who did not have a Computed-Tomography (CT) scan of their abdomen performed within 7 days of index hospitalization were then excluded. Given the known limitations of using administrative data such as International Classification of Diseases, Ninth Edition, Clinical Modification (ICD-9-CM) sepsis codes for identifying actual incidences of this disease [20, 21], research investigators manually ascertained which of the remaining patients met Sepsis-3 criteria [1]. A diagnosis of sepsis required that a patient experienced a change in sequential organ failure assessment (SOFA) score of two or more, in the setting of clinically suspected or microbiologically proven infection, in accordance with the Sepsis-3 criteria [1].
Demographic data, medical comorbidities and short- and long-term clinical outcomes were obtained from the electronic medical record. Medical comorbidities were identified using ICD-9 billing codes. Severity of acute illness was defined by Acute Physiology and Chronic Health Evaluation (APACHE) II and Sequential Organ Failure Assessment (SOFA) scores [22, 23], which were calculated by the research investigators. The manuscript was written according to the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) criteria [24].
Assessment of low muscle mass
Axial CT scan images, 3.0 mm in thickness and taken at the L3 vertebral level were obtained from the Picture Archiving and Communication System (PACS), in Digital Imaging and Communication in Medicine (DICOM) format. Abdominal and/or pelvic CT imaging performed within 7 days of the date of index hospitalization were used to define low muscle mass. Specifically, low muscle mass was defined as \(\le\) 5th percentile of skeletal muscle index of a sex-matched, reference population (41.6 cm2/m2 for males and 32.0 cm2/m2 for females), as previously described [16, 25]. Skeletal muscle area was measured manually by using the freely-available ImageJ software (version 1.53t, U. S. National Institutes of Health, Bethesda, Maryland, USA) [26], as illustrated in Fig. 1 and using methods previously described [27]. Both CT images obtained with and without intravenous contrast were used in the calculation of skeletal muscle area, as previously reported [28]. Since muscle mass is related to age, we also analyzed the age-adjusted effects of low muscle mass on clinical outcomes. We used an age cutoff of 70 years to define ‘older’ versus ‘younger’ patients with sepsis, based on data from previous epidemiologic studies [2, 29, 30].

Measuring skeletal muscle area on L3 axial slice Computer-Tomography (CT) Image, Using the National Institutes of Health ImageJ. Radio density thresholds were selected to correlate with those of skeletal muscle, with lower and upper thresholds of − 29 and 150 Hounsfield units, respectively. A Outer perimeter of the abdominal muscles is first delineated (yellow tracing) and area calculated, B The process is repeated for the inner perimeter of abdominal muscles (yellow tracing), C Vertebral area is further excluded (yellow tracing). The difference between measures equates to the area of skeletal muscle at the L3 level
Clinical outcomes
The primary outcome of one-year mortality was defined from the time of sepsis diagnosis during patients’ index hospitalization. In-hospital mortality, a secondary outcome, was defined as the occurrence of death during patients’ index hospitalization. ‘Favorable’ discharge disposition was defined as transfer of sepsis survivors from hospital directly to their home at the end of their index hospitalization, while ‘unfavorable’ discharge disposition was defined as transfer from hospital to a rehabilitation facility (skilled nursing facility or inpatient rehabilitation facility) or hospice care. All follow-up data for clinical outcomes was obtained from the electronic medical record > 18 months following the date of hospitalization of the latest septic patient included in the cohort, to allow sufficient time for mortality data to be reflected in the electronic medical record.
Statistical analysis
Our sample size of 150 patients was based on two recent, comparable, retrospective cohort studies that assessed the effects of low muscle mass on short-term, clinical outcomes [15, 16]. For binary and nominal outcomes, we constructed frequencies and percentages as descriptive statistics, and implemented Fisher’s exact test statistics to compare patients with and without low muscle mass. For continuous outcomes, we constructed median and inter-quartile ranges (IQR) as descriptive statistics and implemented Wilcoxon rank-sum tests to compare groups with and without low muscle mass. One-year survival was defined as death within 365 days of discharge from index hospitalization and was analyzed via Kaplan–Meier survival curves and log-rank tests. In-hospital survival was similarly analyzed using survival status at hospital discharge. Cox regression was used to estimate the effect of muscle mass on in-hospital and one-year survival, correcting for SOFA and APACHE II illness severity scores. For this Cox regression, the proportional hazard assumption was assessed and found to be satisfied. Multivariable logistic regression was used to analyze the effect of muscle mass on the binary outcome of discharge disposition, adjusted for illness severity. The assumptions of logistic regression were satisfied as the observations were independent of each other and variables were found not to be too highly correlated with each other. Analyses were performed using R v4.1.2 (R core team, 2022). In all statistical analyses, the significance level was set at p = 0.05. Results with a p value less than or equal to 0.05 were considered statistically significant.
Results
Study population
Of the 150 patients that were included, 34 patients (23%) met criteria for pre-existing low muscle mass (Fig. 2). Age, SOFA and APACHE II scores for patients with low muscle mass were higher than those having preserved muscle mass (Table 1). Sex- and age-specific body composition parameters are shown Table 2.

Flow diagram demonstrating numbers of individuals included and excluded at each stage of the study
Association between low muscle mass and one-year survival
Table 3 presents the results of the univariable analysis of clinical outcomes in patients having low and preserved muscle mass. In univariate analysis, low muscle mass significantly decreased one-year survival, with an estimated survival probability at one-year of 29.4% (95% CI: 17.5%-49.5%) in these patients, versus 62% (95% CI: 54%-72%) in patients with preserved muscle mass (p = 0.0005). One-year survival probability for patients with low versus preserved muscle mass is shown in Fig. 3A (hazard ratio = 2.4, 95% CI: 1.44–3.9, p < 0.001). After adjusting for age, APACHE II and SOFA score by Cox multivariable regression, low muscle mass remained an independent risk factor for one-year mortality (hazard ratio 1.9; 95% CI 1.1 – 3.2; p = 0.014) (Fig. 3B). For each one-unit increase in APACHE II, the risk of death within one year increased by a factor of 1.05 (95% CI: 1.00 – 1.09, p = 0.027). Similarly, for each one-unit increase in SOFA score, the risk of death within one year increased by a factor of 1.19 (95% CI: 1.09 – 1.31, p < 0.001). However, age did not emerge as a significant risk factor for the one-year survival outcome (Fig. 3B).

Association Between Low Muscle Mass and One-year Mortality. A Kaplan–Meier survival curves demonstrating the effect of low muscle mass on one-year mortality, in septic patients. 95% confidence intervals are shown. B Cox multivariable regression assessing the effect of low muscle mass on one-year mortality when adjusting for age and severity of illness by SOFA and APACHE II scores
Association between low muscle mass and in-hospital mortality
In univariable analysis, low muscle mass non-significantly decreased in-hospital survival (hazard ratio 1.93; 95% CI: 0.98 – 3.78; p = 0.056). In-hospital survival probability for patients with low versus preserved muscle mass is shown in Fig. 4A. After adjusting for age, SOFA score and APACHE II by Cox multivariable regression, low muscle mass was not a significant risk factor for in-hospital mortality (hazard ratio 1.33; 95% CI 0.64 – 2.76; p = 0.437) (Fig. 4B). For each one-unit increase in APACHE II, the risk of death in the hospital shows a trend towards an increase by a factor of 1.06, although this did not reach statistical significance (95% CI: 0.997 – 1.12, p = 0.061). For each one-unit increase in SOFA score, the risk of death in the hospital increased significantly by a factor of 1.236 (95% CI: 1.10 – 1.39, p < 0.001). Age did not emerge as a significant risk factor for in-hospital mortality (Fig. 4B).

Association Between Low Muscle Mass and In-hospital Mortality. A Kaplan–Meier survival curves demonstrating the effect of low muscle mass on in-hospital mortality, in septic patients. 95% confidence intervals are shown. B Cox multivariable regression assessing the effect of low muscle mass on in-hospital mortality when adjusting for age and severity of illness by SOFA and APACHE II scores
Association between low muscle mass and hospital discharge disposition
Univariable logistic regression analysis revealed that the proportion of patients experiencing unfavorable post-hospital discharge disposition was higher in patients having low muscle mass, affecting 67% of these patients (odds ratio 3.4; 95% CI: 1.3 – 9.8; p = 0.017) (Table 4). However, in multivariate logistic regression adjusted for age, APACHE II and SOFA score, the odds of having an unfavorable hospital discharge were not significant in patients having low muscle mass (odds ratio 1.92, 95% CI: 0.63 - 6.12, p = 0.253). Younger septic patients were less likely to experience unfavorable disposition compared to older patients, by a factor of 0.3 (95% CI: 0.11 - 0.70, p = 0.007). Patients with higher APACHE II score also had an increased likelihood of an unfavorable discharge disposition (OR = 1.1, 95% CI: 1.03 –1.24, p = 0.01) (Fig. 5).

Logistic analysis assessing the effect of low muscle mass on discharge disposition when adjusting for age and severity of illness by SOFA and APACHE II score
Discussion
Rapid and accurate assessments of sarcopenia have gained increasing traction amongst clinicians seeking to risk-stratify patients requiring medical care [31, 32]. In the present analysis, we used low muscle mass as a surrogate for sarcopenia, with numerical cut-offs for low muscle mass that were derived from a race-matched population described in a prior investigation [16]. We observed a 23% prevalence of pre-existing low muscle mass in critically ill patients with sepsis, as compared with a reported prevalence ranging between 5 and 31% [15, 16]. We also identified low muscle mass as an independent risk factor for one-year mortality, although it did not increase the risk for in-hospital mortality or for unfavorable hospital discharge disposition.
While our investigation did not find an association between low muscle mass and short-term mortality following sepsis, Oh et al. reported both an increase in short- and long-term mortality risk, in a single-center, retrospective study of patients with septic shock and sarcopenia (defined by abdominal muscle area on CT scan) [33]. However, it is important to note that this study only included patients with shock, who inherently experience higher mortality rates as compared with patients having sepsis alone [34]. Additionally, the study by Oh et al. did not evaluate the impact of sarcopenia on post-hospitalization discharge status, which could serve as a surrogate measure for quality of life in survivors of critical illness. Our findings align more closely with those reported in a prospective, single-center investigation of 47 sepsis patients, concluding that pre-existing sarcopenia is independently associated with poor long-term functional status and increased one-year mortality [35]. Interestingly, the latter study demonstrated that, while sepsis-induced critical illness leads to an acute and persistent loss of muscle mass at three months, it does not have the same effect on long-term functional status and one-year mortality as pre-existing sarcopenia does [35].
The juxtaposed findings of unchanged in-hospital mortality and increased one-year mortality, in critically ill patients with sepsis and pre-existing low muscle mass, is notable. It is plausible that patients with significant medical comorbidities, including low muscle mass, survive their index hospitalization but are then more likely to require the intensive support provided by skilled nursing services and rehabilitation facilities following discharge from the hospital. One-year mortality data may provide more objective insight into the long-term effects of muscle dysfunction in patients who survive hospitalization but continue to experience high post-hospitalization care needs. Further prospective research is needed to discern the influences of low muscle mass on post-hospitalization care.
Our investigation does not allow us to differentiate between acute loss of muscle mass due to sepsis and other factors affecting critically ill patients [36], and chronic loss of muscle mass. However, it is essential to consider that skeletal muscle plays a significant role in the influence of body composition on clinical outcomes, as it governs crucial functions like mobility, strength, and balance [37]. Several studies have shown a clear association between reduced muscle mass and unfavorable outcomes, including decreased ventilator-free and ICU days [38] and shorter overall survival [39, 40]. Moreover, sepsis induces hypermetabolism and inflammation, leading to protein breakdown, which is further exacerbated by inadequate nutrition [41]. The immobility resulting from critical illness also contributes to muscle disuse and atrophy [42].
The combination of low muscle mass and sepsis is likely to produce a synergistic negative effect in critically ill patients. While the retrospective nature of our investigation precludes us from determining causal effects, it is plausible that low muscle mass acts as both a causative factor and as an outcome associated with a poor long-term prognosis. When low muscle mass is identified in a patient, clinicians can take several steps to intervene and address this issue. Assuming that sepsis is being appropriately managed, nutritional support is of utmost importance for maintaining and building muscle mass [43]. Physical therapy and exercise, including early mobility and ambulation, are also particularly important and supported by an extensive body of literature that associates these interventions with improved clinical outcomes [44]. Respiratory therapy and protocolized daily spontaneous awakening and breathing trials, in mechanically ventilated patients, may lead to shorter duration of mechanical ventilation and earlier mobility, thus preserving muscle mass [45, 46]. Collaborative care amongst a multidisciplinary care team of physicians, nurses, dieticians, and physical therapists can provide comprehensive care in a challenging patient population, thus improving outcomes.
Unlike frailty assessments, which require an interview of patients or their families to assess slowness, weakness, weight loss and exhaustion [47, 48], image-based assessments of muscle mass do not require reliable information about one’s past medical history. This is a crucial advantage when caring for critically ill patients, since these patients often suffer from confusion and/or encephalopathy and are often admitted emergently to the hospital in the absence of family members who could corroborate their medical history. Body mass index (BMI) provides an objective measure of body proportions, and it has been associated with long-term prognosis including mortality [49]. However, BMI does not differentiate between weight derived from fat, muscle, bone, or water. An elevated BMI could result from either a high body fat content or significant muscle mass. Assessments like SMA/SMI offer a more nuanced understanding of an individual's body composition. CT imaging-based risk assessment tools are also particularly useful in sepsis since these patients often undergo imaging as part of their medical work-up and the results are rapidly available within the electronic medical record.
Strengths of our study include a complete data set of one-year outcomes for all patients, and the validation of sepsis diagnoses by research investigators, according to contemporary Sepsis-3 criteria. Its main limitations are its retrospective nature, its predominantly Caucasian population (reflective of the healthcare system’s catchment area), and its single-center design. Selection bias may have been introduced by the inadvertent exclusion of patients that did not undergo an abdominal CT scan because the origin of sepsis was clearly of non-abdominal origin. While in-hospital mortality was not different between septic patients with and without low muscle mass, the former group did experience significantly shorter median survival times, which could potentially affect statistical comparison of one-year mortality rates. Furthermore, comorbidities were primarily based on ICD-9 codes (potential underreporting bias) and critical illness was defined by billing information provided by the physician. The latter definition of critical illness would not necessarily mean that a patient was admitted to an intensive care unit for sepsis care, as a physician can also bill for critical care therapy in an emergency department setting. The inclusion of critically ill patients with sepsis, a population that experiences high mortality rates and frequent discharge to a rehabilitation facility, may also necessarily limit the external validity of our results. However, this population accounts for a large proportion of the morbidity and healthcare costs, and it is therefore of interest to epidemiologists, physicians, and healthcare administrators alike [50].
Conclusions
Low muscle mass, as indicated by a reduced L3SMI measured on abdominal CT within 7 days of sepsis onset, is independently associated with increased one-year mortality but is not associated with hospital mortality or unfavorable discharge disposition. These findings have significant implications for clinical management, research, and quality of life in patients with sepsis. For clinicians, regular assessment of muscle mass, possibly through L3SMI measurements, could become a routine aspect of sepsis patient evaluations. Identifying at-risk patients early may facilitate targeted interventions, such as nutritional support or physical therapy, to counteract muscle loss and potentially improve long-term outcomes. Given the demonstrated association between low muscle mass and one-year mortality, future research should delve deeper into understanding the mechanisms behind this correlation. Moreover, intervention studies could be designed to explore ways of preserving or increasing muscle mass in sepsis patients and to evaluate their impact on both short-term and long-term outcomes. Regarding patient function, a deeper comprehension of the epidemiology and clinical consequences of low muscle mass can guide strategies to enhance both survival rates and the functional well-being of sepsis survivors. By highlighting the potential repercussions of muscle atrophy in critically ill sepsis patients, this study underscores the need for multi-disciplinary approaches that go beyond immediate clinical management, encompassing aspects of rehabilitation, nutritional guidance, and long-term patient care.
Availability of data and materials
All data resulting from this analysis is contained within the manuscript.
References
Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–10.
Lu J, Liu J, Zhu L, Zhang Y, Li A. The effect of age on the clinical characteristics and innate immune cell function in the patients with abdominal sepsis. Front Physiol. 2022;13:952434.
Rantanen T. Muscle strength, disability and mortality. Scand J Med Sci Sports. 2003;13(1):3–8.
Sakuma K, Aoi W, Yamaguchi A. Current understanding of sarcopenia: possible candidates modulating muscle mass. Pflugers Arch. 2015;467(2):213–29.
Mitchell WK, Williams J, Atherton P, Larvin M, Lund J, Narici M. Sarcopenia, dynapenia, and the impact of advancing age on human skeletal muscle size and strength; a quantitative review. Front Physiol. 2012;3:260.
Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010;39(4):412–23.
Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyere O, Cederholm T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(4):601.
Portal D, Hofstetter L, Eshed I, Dan-Lantsman C, Sella T, Urban D, et al. L3 skeletal muscle index (L3SMI) is a surrogate marker of sarcopenia and frailty in non-small cell lung cancer patients. Cancer Manag Res. 2019;11:2579–88.
Portal D, Melamed G, Segal G, Itelman E. Sarcopenia as Manifested by L3SMI Is Associated with Increased Long-Term Mortality amongst Internal Medicine Patients-A Prospective Cohort Study. J Clin Med. 2022;11(12):3500.
Shen W, Punyanitya M, Wang Z, Gallagher D, St-Onge MP, Albu J, et al. Total body skeletal muscle and adipose tissue volumes: estimation from a single abdominal cross-sectional image. J Appl Physiol (1985). 2004;97(6):2333–8.
Scafoglieri A, Clarys JP. Dual energy X-ray absorptiometry: gold standard for muscle mass? J Cachexia Sarcopenia Muscle. 2018;9(4):786–7.
Stokes T, Tripp TR, Murphy K, Morton RW, Oikawa SY, Lam Choi H, et al. Methodological considerations for and validation of the ultrasonographic determination of human skeletal muscle hypertrophy and atrophy. Physiol Rep. 2021;9(1):e14683.
Joskova V, Patkova A, Havel E, Najpaverova S, Uramova D, Kovarik M, et al. Critical Evaluation of Muscle Mass Loss as a Prognostic Marker of Morbidity in Critically Ill Patients and Methods for Its Determination. J Rehabil Med. 2018;50(8):696–704.
Sergi G, De Rui M, Stubbs B, Veronese N, Manzato E. Measurement of lean body mass using bioelectrical impedance analysis: a consideration of the pros and cons. Aging Clin Exp Res. 2017;29(4):591–7.
Shibahashi K, Sugiyama K, Kashiura M, Hamabe Y. Decreasing skeletal muscle as a risk factor for mortality in elderly patients with sepsis: a retrospective cohort study. J Intensive Care. 2017;5:8.
Baggerman MR, van Dijk DPJ, Winkens B, van Gassel RJJ, Bol ME, Schnabel RM, et al. Muscle wasting associated co-morbidities, rather than sarcopenia are risk factors for hospital mortality in critical illness. J Crit Care. 2020;56:31–6.
Liu W, Hu CH, Zhao SP. Sarcopenia and mortality risk of patients with sepsis: a meta-analysis. Int J Clin Pract. 2022;2022:4974410.
Kahn JM, Le T, Angus DC, Cox CE, Hough CL, White DB, et al. The epidemiology of chronic critical illness in the United States*. Crit Care Med. 2015;43(2):282–7.
Kline KA, Bowdish DM. Infection in an aging population. Curr Opin Microbiol. 2016;29:63–7.
Jolley RJ, Sawka KJ, Yergens DW, Quan H, Jette N, Doig CJ. Validity of administrative data in recording sepsis: a systematic review. Crit Care. 2015;19(1):139.
Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348(16):1546–54.
Ferreira FL, Bota DP, Bross A, Melot C, Vincent JL. Serial evaluation of the SOFA score to predict outcome in critically ill patients. Jama-J Am Med Assoc. 2001;286(14):1754–8.
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818–29.
von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4(10):e296.
van der Werf A, Langius JAE, de van der Schueren MAE, Nurmohamed SA, van der Pant K, Blauwhoff-Buskermolen S, et al. Percentiles for skeletal muscle index, area and radiation attenuation based on computed tomography imaging in a healthy Caucasian population. Eur J Clin Nutr. 2018;72(2):288–96.
Schneider CA, Rasband WS, Eliceiri KW. NIH Image to ImageJ: 25 years of image analysis. Nat Methods. 2012;9(7):671–5.
Gomez-Perez S, McKeever L, Sheean P. Tutorial: a step-by-step guide (version 2.0) for measuring abdominal circumference and skeletal muscle from a single cross-sectional computed-tomography image using the National Institutes of Health ImageJ. J Parenter Enteral Nutr. 2020;44(3):419–24.
Gomez-Perez SL, Haus JM, Sheean P. Measuring abdominal circumference and skeletal muscle from a single cross-sectional computed tomography image: a step-by-step guide for clinicians using National Institutes of Health ImageJ (vol 40, pg 308, 2016). J Parenter Enteral Nutr. 2016;40(5):742–3.
Prest J, Sathananthan M, Jeganathan N. Current trends in sepsis-related mortality in the United States. Crit Care Med. 2021;49(8):1276–84.
Kotfis K, Wittebole X, Jaschinski U, Sole-Violan J, Kashyap R, Leone M, et al. A worldwide perspective of sepsis epidemiology and survival according to age: Observational data from the ICON audit. J Crit Care. 2019;51:122–32.
Alvarez-Bustos A, Rodriguez-Sanchez B, Carnicero-Carreno JA, Sepulveda-Loyola W, Garcia-Garcia FJ, Rodriguez-Manas L. Healthcare cost expenditures associated to frailty and sarcopenia. BMC Geriatr. 2022;22(1):747.
Tjeertes EKM, van Fessem JMK, Mattace-Raso FUS, Hoofwijk AGM, Stolker RJ, Hoeks SE. Influence of frailty on outcome in older patients undergoing non-cardiac surgery - a systematic review and meta-analysis. Aging Dis. 2020;11(5):1276–90.
Oh HJ, Kim JH, Kim HR, Ahn JY, Jeong SJ, Ku NS, et al. The impact of sarcopenia on short-term and long-term mortality in patients with septic shock. J Cachexia Sarcopenia Muscle. 2022;13(4):2054–63.
Shankar-Hari M, Phillips GS, Levy ML, Seymour CW, Liu VX, Deutschman CS, et al. Developing a new definition and assessing new clinical criteria for septic shock: for the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):775–87.
Cox MC, Booth M, Ghita G, Wang Z, Gardner A, Hawkins RB, et al. The impact of sarcopenia and acute muscle mass loss on long-term outcomes in critically ill patients with intra-abdominal sepsis. J Cachexia Sarcopenia Muscle. 2021;12(5):1203–13.
Puthucheary ZA, Rawal J, McPhail M, Connolly B, Ratnayake G, Chan P, et al. Acute skeletal muscle wasting in critical illness. JAMA. 2013;310(15):1591–600.
Prado CM, Purcell SA, Alish C, Pereira SL, Deutz NE, Heyland DK, et al. Implications of low muscle mass across the continuum of care: a narrative review. Ann Med. 2018;50(8):675–93.
Moisey LL, Mourtzakis M, Cotton BA, Premji T, Heyland DK, Wade CE, et al. Skeletal muscle predicts ventilator-free days, ICU-free days, and mortality in elderly ICU patients. Crit Care. 2013;17(5):R206.
Weijs PJM, Looijaard WGPM, Dekker IM, Stapel SN, Girbes AR, Oudemans-van Straaten HM, et al. Low skeletal muscle area is a risk factor for mortality in mechanically ventilated critically ill patients. Crit Care. 2014;18(2):R12.
Akahoshi T, Yasuda M, Momii K, Kubota K, Shono Y, Kaku N, et al. Sarcopenia is a predictive factor for prolonged intensive care unit stays in high-energy blunt trauma patients. Acute Med Surg. 2016;3(4):326–31.
Chiolero R, Revelly JP, Tappy L. Energy metabolism in sepsis and injury. Nutrition. 1997;13(9 Suppl):45S-51S.
Hasselgren PO, Menconi MJ, Fareed MU, Yang H, Wei W, Evenson A. Novel aspects on the regulation of muscle wasting in sepsis. Int J Biochem Cell Biol. 2005;37(10):2156–68.
Gomes F, Baumgartner A, Bounoure L, Bally M, Deutz NE, Greenwald JL, et al. Association of nutritional support with clinical outcomes among medical inpatients who are malnourished or at nutritional risk an updated systematic review and meta-analysis. JAMA Netw Open. 2019;2(11):e1915138.
Kayambu G, Boots R, Paratz J. Physical therapy for the critically ill in the ICU: a systematic review and meta-analysis. Crit Care Med. 2013;41(6):1543–54.
Kollef MH, Shapiro SD, Silver P, St John RE, Prentice D, Sauer S, et al. A randomized, controlled trial of protocol-directed versus physician-directed weaning from mechanical ventilation. Crit Care Med. 1997;25(4):567–74.
Woo HY, Oh SY, Lee H, Ryu HG. Evaluation of the association between decreased skeletal muscle mass and extubation failure after long-term mechanical ventilation. Clin Nutr. 2020;39(9):2764–70.
Veld LPMOH, van Rossum E, Kempen GIJM, de Vet HCW, Hajema K, Beurskens AJHM. Fried phenotype of frailty: cross-sectional comparison of three frailty stages on various health domains. BMC Geriatr. 2015;15:77.
Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146–56.
Xu H, Cupples LA, Stokes A, Liu CT. Association of obesity with mortality over 24 years of weight history: findings from the Framingham Heart Study. JAMA Netw Open. 2018;1(7):e184587.
Buchman TG, Simpson SQ, Sciarretta KL, Finne KP, Sowers N, Collier M, et al. Sepsis among medicare beneficiaries: 3. The methods, models, and forecasts of sepsis, 2012–2018. Crit Care Med. 2020;48(3):302–18.
Acknowledgements
We would like to acknowledge Dr. Vernon Chinchilli for his mentorship and guidance with data analysis.
Funding
Funding was provided by the National Institute of General Medical Sciences, grant #K08GM138825 (ASB).
Author information
Authors and Affiliations
Contributions
N.D. and S.S. performed the measurements, A.B. and K.K. were involved in planning and supervising the work, A.B., N.D. and X.W. processed the experimental data and performed the analysis. N.D., S.S. B.M., X.W. and A.B. drafted the manuscript and designed the figures. All authors discussed the results, edited the manuscript, and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The need for study approval was waived by The Penn State College of Medicine Institutional Review Board of the Human Studies Protection Office on May 10, 2021 (ref# 17613). The Penn State College of Medicine Institutional Review Board of the Human Studies Protection Office also waived the need for Informed Consent. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Darden, N., Sharma, S., Wu, X. et al. Long-term clinical outcomes in critically ill patients with sepsis and pre-existing low muscle mass: a retrospective cohort study. BMC Anesthesiol 23, 313 (2023). https://doi.org/10.1186/s12871-023-02274-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-023-02274-y