
Abstract
Background
This study was conducted to investigate the effects and safety of remimazolam versus propofol on cerebral oxygen saturation and cerebral hemodynamics during the induction of general anesthesia in patients receiving carotid endarterectomy (CEA), so as to provide theoretical basis for better clinical application of remimazolam.
Methods
Forty-three patients (60–75 years old) with carotid artery stenosis (carotid artery stenosis greater than 70%) were randomly divided into the remimazolam group (R group) and the propofol group (P group). Anesthesia was induced with remimazolam (0.3 mg/kg) or propofol (1.5-2 mg/kg) individually. At time of admission (T0), post-anesthesia induction (T1), consciousness disappears (T2), 1 min after loss of consciousness (T3), 2 min after loss of consciousness (T4) and pre-endotracheal intubation (T5), measurement in patients with regional cerebral oxygen saturation (SrO2), average blood flow velocity (Vm), resistance index (RI), mean arterial pressure (MAP), heart rate (HR) and cardiac index (CI) were recorded.
Results
SrO2 increased significantly in both groups after induction of anesthesia compared with baseline (P < 0.05) and decreased after loss of consciousness (P < 0.05). There was no difference in the mean value of the relative changes in SrO2 between the groups. Meanwhile, the Vm, RI, HR and CI of each time point between two groups showed no statistically significant difference (P > 0.05) while MAP in group P at T5 was lower than that in group R individually(P < 0.05). In each group, Vm, HR, CI and MAP at T2-T5 were all significantly reduced compared with T1, with statistically differences(P < 0.05). Specifically, there was no difference of RI at each time between or within groups(P > 0.05).
Conclusions
Our study revealed that remimazolam can be administered safely and effectively during the induction of general anesthesia for carotid endarterectomy in elder population and it demonstrated superiority in hemodynamic changes compared with propofol.
Clinical trial registration
This trial was retrospectively registered with the Chinese Clinical Trial Registry. Registration number: ChiCTR2300070370. Date of registration: April 11, 2023.
Similar content being viewed by others

Introduction
Carotid artery stenosis is a major reason of stroke in elderly, accounting for about 20% of all cases and leads to high mortality and heavy economic burden [1, 2]. Carotid endarterectomy (CEA) remains the recommended treatment for the prevention of stroke in symptomatic patients with carotid artery stenosis, which is usually performed under general anesthesia [3, 4]. Most of patients are elderly accompanied with cardiovascular diseases, so severe hemodynamic fluctuations are easy to occur during the induction period of general anesthesia, which may not only exacerbate the preoperative cerebral blood supply deficiency, but also cause cerebral hypoxia and thereby lead to postoperative nervous system function deficiency [5, 6]. Therefore, for patients with severe carotid artery stenosis, due to the impairment of carotid pressure receptors and cerebral blood flow automatic regulation, choosing anesthetics which has less adverse effects and protects from cerebral ischemia or hypoxia is necessary.
Cerebral oxygen saturation (SrO2) can reflect the balance of oxygen supply and demand of brain tissue, which is related to the arterial oxygen saturation, hemoglobin, cerebral blood flow (CBF) and cerebral metabolic rate of oxygen (CMRO2). Thus, monitoring SrO2 is a noninvasive method to observe the changes in CBF and predict the occurrence of cerebral ischemia during the induction of general anesthesia [7]. Meanwhile, transcranial doppler (TCD) can measure mean blood velocity (Vm) and resistance index (RI) of the middle cerebral artery. Thus, we are able to investigate cerebral blood flow and oxygen saturation using these indexes.
Propofol is frequently used intravenously for the induction of sedation during general anesthesia, which is often associated with hemodynamic depression. Previous studies have shown that anesthesia induction with propofol decreased the CBF as CMRO2 was reduced due to the different degrees of blood pressure decline [8], and may break the cerebral oxygen balance. In addition, there were gender differences in the effect of propofol anesthesia on perioperative cerebral oxygenation under general anesthesia in patients undergoing CEA, female patients had significantly lower regional cerebral oxygen saturation values compared with male patients during clamping of the carotid artery [9]. Remimazolam is an ultrashort-acting benzodiazepine inducing sedation with rapid onset, good control of the depth of anesthesia, full and predictable recovery, a benign safety profile particularly in terms of hemodynamic effects [10]. According to the latest researches, remimazolam provided adequate procedural sedation for endoscopy and its actual anesthetic effect is not inferior to that of traditional anesthesia-inducing drugs [11]. Remimazolam has the same efficacy as propofol in induction and maintenance of general anesthesia [12]. However, the use of remimazolam for induction of general anesthesia in patients undergoing carotid endarterectomy has not been reported.
Hence, we tested the hypothesis that remimazolam will maintain CBF and SrO2 better than propofol in terms of carotid endarterectomy as a sedative for the induction of general anesthesia. To validate this, we compared the SrO2 and cerebral hemodynamics during the anesthesia induction.
Methods
Study design
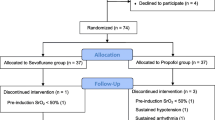
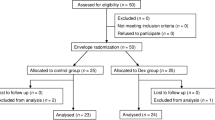
This randomized clinical trial was approved by the Institutional Review Board of The Dushu Lake Hospital Affiliated to Soochow University (Fig. 1), all methods were carried out in accordance with relevant guidelines and regulations. 43 Patients (average age 67.20 ± 4.29) scheduled to undergo CEA under general anesthesia were randomly allocated into the propofol group or remimazolam group using Excel program RAND function. Patients excluded from this study included mentally disabled patients, patients with ASA class ≥ V, alcohol or drug abusers, patients being administered drugs that may affect study considered by researchers. The indications for CEA in this study are symptomatic patients with stenosis > 70% confirmed by ultrasound and all CEAs performed in this study were primary repairs.

Enrolment flow diagram
Experimental procedure
After patient arriving in the operating room, 5-lead electrocardiography, pulse oximetry, and non-invasive automatic blood pressure cuff were implemented for basic monitoring. INVOS cerebral oximeter (Somanetics, Troy, MI, USA) was applied for monitoring of operative side SrO2. To assess the depth of anesthesia, BIS® A-2000™ (Aspect Medical Systems, Natick, MA, USA) was attached to the contralateral forehead. A 20-gauge catheter was placed in the radial artery after local anesthetic infiltration to monitor continuous arterial blood pressure and CI (Cardiac Index) by using Flotrac/vigileo system (Edwards Lifesciences, Irvine, Ca, USA). Meanwhile, ultrasonic probe was placed on the temporal window with frequency set at 2 MHz and depth set at 50-55 mm to monitor the cerebral blood flow velocity.
The induction of general anesthesia was performed via infusion of 0.3 mg/kg remimazolam in R group or 1.5-2 mg/kg propofol in P group within 30 s [13, 14]. Additional dose was given with 2.5 mg remimazolam or 50 mg propofol if the BIS > 60 after 3 min. When adequate sedation (BIS = < 60) was achieved and confirmation of the loss of consciousness, sufentanil(3ug/kg) and cis-atracurium(2 mg/kg) was given to fulfill endotracheal intubation. General anesthesia was maintained by sevoflurane by adjust concentration to achieve a BIS value of 40–60.
Cerebral oxygen saturation and hemodynamics record
This study set several time points to record index during the whole process of the induction of anesthesia in both groups. Specifically, after admission of patient, the basal levels of SrO2, MAP, HR, CI, RI and Vm were recorded as T0. Data were recorded simultaneously and continuously after induction of anesthesia(T1), loss of consciousness(T2), every 1 min for 2 min after loss of consciousness(T3-T4) and before intubation(T5).
Statistical analysis
Previous studies [15]in patients receiving CEA showed maximal decreases in SrO2 of 8.1% ± 6.2% after induction in the propofol group. Therefore, assuming maximal decreases in SrO2 of 3% in remimazolam group, the sample size was calculated to show the difference between groups and 18 patients per group were required to achieve adequate power (P = 0.05; β = 0.8) to detect a difference. Patients’ characteristics, intraoperative variables and indexes between groups were analyzed using Student’s t-test or Pearson’s chi-square test. Continuous variables, including SrO2, blood pressure and heart rate, were analyzed by repeated measures analysis of variance (ANOVA) within each group. Comparisons between groups at each time point were made using two-tailed unpaired t-test. Statistical analysis was performed using the IBM SPSS Statistics version 19 (IBM, Chicago, IL, USA). All data are expressed as means ± standard deviation and P < 0.05 was considered to be statistically significant.
Results
A total of 43 patients were included initially and randomized 21 to remimazolam group, 22 to propofol group. Among these patients, one patient of the remimazolam group with low SrO2 (pre-induction basal value < 50%) and 2 patients of the propofol group that showed sustained hypotension or arrhythmia intraoperatively were excluded. patients’ characteristics including gender, weight, height and BMI were similar in both groups (Table 1). Meanwhile, there were no significant differences in intraoperative values of degree of carotid stenosis, total anesthesia time and total operation time between the groups (Table 2).
Values are mean ± SD or numbers
SrO2 changes in groups
SrO2 increased significantly at T1 in both groups compared with baseline(T0) in remimazolam group and propofol group(P < 0.05). However, there was no difference in the change of SrO2 between remimazolam group and propofol group(P > 0.05) at each time point from T1-T5. Each group showed a downstream trend from T2-T5 (Fig. 2).

Cerebral oxygen saturation (SrO2) changes at post-induction of anesthesia(T1), loss of consciousness(T2), every 1 min for 2 min after loss of consciousness(T3-T4) and pre-intubation(T5). Data are expressed as mean ± standard deviation. *P < 0.05 vs. Baseline in each group
CBF changes in groups
CBF index including RI and Vm were similar from induction to pre-intubation and there were no significant differences between the remimazolam group and propofol group (Fig. 3). Vm showed a downward trend from T1-T5 in each group while RI appeared to be steady at each time point.

Hemodynamics index changes from T0 to T5. Changes in (A) mean arterial pressure (MAP), (B) heart rate (HR), (C) mean flow velocity (Vm), (D) resistance index (RI), (E) cardiac index (CI) from pre-induction of anesthesia until before intubation. Data are expressed as mean ± standard deviation. *P < 0.05 vs. Baseline in each group. + P < 0.05 vs. between two groups
Hemodynamics index in groups
The changes in hemodynamics index including MAP, HR and CI were consistent which showed a downward trend from T1-T5 in remimazolam group and propofol group. And there was no difference of HR or CI at each time point in two groups. It was worth noting that MAP of P group was lower than that of R group(P < 0.05) at T5(Fig. 3).
BIS value in groups
The changes in BIS value showed a downward trend from T0-T4 in remimazolam group and propofol group, and both rise in reflex at T5. The statistics show that the BIS value of P group was lower than that of R group(P < 0.05) at T1-3 and T5, but there was no difference at T4 (Fig. 4).

BIS value changes at post-induction of anesthesia(T1), loss of consciousness(T2), every 1 min for 2 min after loss of consciousness(T3-T4) and pre-intubation(T5). Data are expressed as mean ± standard deviation. *P < 0.05 vs. between two groups
Discussion
Cerebral oxygen detector was used to detect the cerebral oxygen saturation of patients, which is a non-invasive real-time detection to analyze the oxygen supply level of patients’ brain tissue [16, 17]. Relevant studies have shown that the long-term low SrO2 level is closely related to the occurrence of postoperative adverse reactions, neurological recovery, length of hospital stay and mortality [18]. Therefore, SrO2 is often used in clinical anesthesia as a regulation and detection indicator to evaluate critically ill patients, extracorporeal circulation surgery and cerebrovascular disease surgery, predicting the prognosis of patients and preventing the occurrence of adverse events through this indicator [19].
In our study, remimazolam was noninferior compared with propofol in terms of oxygen saturation. SrO2 increased rapidly during induction and then slowly returned to baseline while preparing for endotracheal intubation. This may be accompanied by increased oxygen supply due to ventilation through the mask and decreased cerebral oxygen metabolism due to anesthesia drugs. Besides, mean and minimal SrO2 were similar between both groups but average values of minimal SrO2 were lower in P group than that in R group, which may be relevant with the reduction of cardiac output caused by propofol.
Decreased cardiac output during induction of general anesthesia or imbalance of cerebral perfusion pressure/cerebrovascular resistance may be the reason of decreased cerebral perfusion and thus decreased cerebral oxygen supply. The results of this study showed that the levels of Vm, CI and HR decreased during anesthesia induction, reached the minimum value before intubation in both groups. However, it was noted that propofol has a greater influence on patients’ blood pressure, leading to a larger decrease in MAP in group P after induction. This result suggests that, compared with propofol, remimazolam may have more advantages in hemodynamics of patients as anesthesia inducing drug, and this result is basically consistent with previous research results [20, 21].
However, the vascular resistance index RI remained basically stable at each time point, with no statistically significant change amplitude or difference between the two groups. We consider that the patients in this study are all elderly patients with poor regulation ability of their own blood vessels, and severe internal carotid artery stenosis induces blood–brain barrier injury and impairs the autoregulation to interrupt vasodilation or vasoconstriction [22,23,24].
Data from the research showed that after the induction of general anesthesia, the BIS value of P group was lower than that of R group due to the effect of remimazolam was slowly [25], and BIS values of two groups were similar until 2 min after loss of consciousness, indicating that remimazolam has similar sedative effect as propofol during the induction of general anesthesia.
To our knowledge, this is the first study applying remimazolam for the induction of anesthesia on carotid endarterectomy. We found that remimazolam-sufentanil anesthesia induction was comparable with propofol-sufentanil anesthesia induction in an aspect of preserving the SrO2 and maintaining hemodynamics in patients undergoing carotid endarterectomy. Furthermore, due to the small sample size and the lack of preoperative and postoperative follow-up in this study, more samples should be included and further research is required.
Conclusions
Remimazolam-sufentanil anesthesia induction was comparable with propofol-sufentanil anesthesia induction in an aspect of preserving the SrO2 and stabilizing hemodynamics in patients undergoing carotid endarterectomy.
Data Availability
The datasets analysed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- CEA:
-
Carotid endarterectomy
- SrO2 :
-
Cerebral oxygen saturation
- Vm:
-
Average blood flow velocity
- RI:
-
Resistance index
- MAP:
-
Mean arterial pressure
- HR:
-
Heart rate
- CI:
-
Cardiac index
- CBF:
-
Cerebral blood flow
- CMRO2 :
-
Cerebral metabolic rate of oxygen
References
Aber A, Howard A, Woods HB, Jones G, Michaels J. Impact of carotid artery stenosis on quality of life: a systematic review. The patient. 2019;12(2):213–22. PMID: 30328068.
Boudoulas KD, Triposciadis F, Geleris P, Boudoulas H. Coronary atherosclerosis: pathophysiologic basis for diagnosis and management. Prog Cardiovasc Dis. 2016;58(6):676–92. PMID: 27091673.
Silver FL, Mackey A, Clark WM, Brooks W, Timaran CH, Chiu D, Goldstein LB, Meschia JF, Ferguson RD, Moore WS, Howard G, Brott TG, CREST Investigators. Safety of stenting and endarterectomy by symptomatic status in the carotid revascularization endarterectomy Versus Stenting Trial (CREST). Stroke. 2011;42(3):675–80. PMID: 21307169.
Vinogradov RA, Pykhteev VS, Martirosova KI, Lashevich KA. Perioperative complications prognosis in carotid endarterectomy. Khirurgiia (Mosk). 2018;(1):82–5. PMID: 29376964.
Chen DY, Kuo YS, Hsu HL, Yan FX, Liu HL, Chen CJ, Tseng YC. Loss of labelling efficiency caused by carotid stent in pseudocontinuous arterial spin labelling perfusion study. Clin Radiol. 2016;71(1):e21-7. PMID: 26620708.
Egawa J, Inoue S, Nishiwada T, Tojo T, Kimura M, Kawaguchi T, Taniguchi S, Furuya H, Kawaguchi M. Effects of anesthetics on early postoperative cognitive outcome and intraoperative cerebral oxygen balance in patients undergoing lung surgery: a randomized clinical trial. Can J Anaesth. 2016;63(10):1161–9. PMID: 27412465.
Moritz S, Kasprzak P, Arlt M, Taeger K, Metz C. Accuracy of cerebral monitoring in detecting cerebral ischemia during carotid endarterectomy: a comparison of transcranial Doppler sonography, near-infrared spectroscopy, stump pressure, and somatosensory evoked potentials. Anesthesiology. 2007;107(4):563–9. PMID: 17893451.
Matsuoka T, Ishiyama T, Shintani N, Kotoda M, Mitsui K, Matsukawa T. Changes of cerebral regional oxygen saturation during pneumoperitoneum and Trendelenburg position under propofol anesthesia: a prospective observational study. BMC Anesthesiol. 2019;19(1):72. PMID: 31092197.
Cura Z, Oc B, Arun O, Oc M, Duman I, Duman A. Effects of Sevoflurane and Propofol Anesthesia on cerebral oxygenation in patients undergoing carotid endarterectomy. Turk Neurosurg. 2022;32(1):76–82. PMID: 34664695.
Sneyd JR, Rigby-Jones AE. Remimazolam for anaesthesia or sedation. Curr Opin Anaesthesiol. 2020;33(4):506–11. PMID: 32530890.
Pastis NJ, Yarmus LB, Schippers F, Ostroff R, Chen A, Akulian J, Wahidi M, Shojaee S, Tanner NT, Callahan SP, Feldman G, Lorch DG Jr, Ndukwu I, Pritchett MA, Silvestri GA. PAION Investigators. Safety and Efficacy of Remimazolam compared with placebo and midazolam for moderate Sedation during Bronchoscopy. Chest. 2019;155(1):137–46. PMID: 30292760.
Doi M, Hirata N, Suzuki T, Morisaki H, Morimatsu H, Sakamoto A. Safety and efficacy of remimazolam in induction and maintenance of general anesthesia in high-risk surgical patients (ASA Class III): results of a multicenter, randomized, double-blind, parallel-group comparative trial. J Anesth. 2020;34(4):491–501. PMID: 32303884.
Gallardo-Hernandez AG, Hernandez-Perez AL, Ordoñez-Espinosa G, Sanchez-Lopez A, Revilla-Monsalve C, Islas-Andrade S. Clinical testing of propofol geriatic dose for sedation designed via in silico trial. Comput Methods Programs Biomed. 2016;132:21–7. PMID: 27282224.
Chen Yu, Shu C. Zhu Xiao gang, Ji Fuhai. Sedative effect of remimazolam for induction of general anesthesia in elderly patients. Chin J Anesthesiology. 2020;40(8):3.
Park S, Yook K, Yoo KY, Choi JI, Bae HB, You Y, Jin B, Jeong S. Comparison of the effect of sevoflurane or propofol anesthesia on the regional cerebral oxygen saturation in patients undergoing carotid endarterectomy: a prospective, randomized controlled study. BMC Anesthesiol. 2019;19(1):157. PMID: 31421685.
Casati A, Spreafico E, Putzu M, Fanelli G. New technology for noninvasive brain monitoring: continuous cerebral oximetry. Minerva Anestesiol. 2006;72(7–8):605–25. PMID: 16865080.
Ogasawara K, Konno H, Yukawa H, Endo H, Inoue T, Ogawa A. Transcranial regional cerebral oxygen saturation monitoring during carotid endarterectomy as a predictor of postoperative hyperperfusion. Neurosurgery. 2003;53(2):309 – 14; discussion 314-5. PMID: 12925245.
LaManna JC. Cerebral angioplasticity: the anatomical contribution to ensuring Appropriate Oxygen Transport to Brain. Adv Exp Med Biol. 2018;1072:3–6. PMID: 30178315.
Pavlisko ND, Killos M, Henao-Guerrero N, Riccó CH, Werre S. Evaluation of tissue hemoglobin saturation (StO2) using near-infrared spectroscopy during hypoxemia and hyperoxemia in Beagle dogs. Vet Anaesth Analg. 2016;43(1):18–26. PMID: 25818866.
Doi M, Morita K, Takeda J, Sakamoto A, Yamakage M, Suzuki T. Efficacy and safety of remimazolam versus propofol for general anesthesia: a multicenter, single-blind, randomized, parallel-group, phase IIb/III trial. J Anesth. 2020;34(4):543–53. PMID: 32417976.
Chen S, Wang J, Xu X, Huang Y, Xue S, Wu A, Jin X, Wang Q, Lyu J, Wang S, Li Y, Yu Y, Ai D, Luo A, Min S, Li L, Zou X, Liu J, Lv P, Chai X, Sun X, Zhao Z, Zhang J. The efficacy and safety of remimazolam tosylate versus propofol in patients undergoing colonoscopy: a multicentered, randomized, positive-controlled, phase III clinical trial. Am J Transl Res. 2020;12(8):4594–603. PMID: 32913533.
Steiner LA, Johnston AJ, Chatfield DA, Czosnyka M, Coleman MR, Coles JP, Gupta AK, Pickard JD, Menon DK. The effects of large-dose propofol on cerebrovascular pressure autoregulation in head-injured patients. Anesth Analg. 2003;97(2):572–6. PMID: 12873955.
Chen J, Liu J, Xu WH, Xu R, Hou B, Cui LY, Gao S. Impaired dynamic cerebral autoregulation and cerebrovascular reactivity in middle cerebral artery stenosis. PLoS ONE. 2014;9(2):e88232. PMID: 24505442.
Grüne F, Klimek M. Cerebral blood flow and its autoregulation - when will there be some light in the black box? Br J Anaesth. 2017;119(6):1077–9. PMID: 29156025.
Upton RN, Martinez AM, Grant C. Comparison of the sedative properties of CNS 7056, midazolam, and propofol in sheep. Br J Anaesth. 2009;103(6):848–57. PMID: 19797247.
Acknowledgements
We thank our departmental colleagues for their help in this study.
Funding
This study was supported by Suzhou Science and Technology Bureau, Jiangsu, China (No. SZM2021002, No. SZM2021003).
Author information
Authors and Affiliations
Contributions
JLG, CDY and QYJ conceived and designed the experiments. JLG, CDY and QYJ wrote, reviewed and revised the manuscript; JLG, CDY and QYJ developed the methodology; JLG, CDY and JL analyzed and interpreted the data; JL supervised the study. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All study participants provided informed consent, and the study design was approved by Institutional Ethics Committee of the Dushu Lake Hospital Affiliated to Soochow University (approval number: 210070).
Consent for publication
Not applicable.
Competing interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Gao, J., Yang, C., Ji, Q. et al. Effect of remimazolam versus propofol for the induction of general anesthesia on cerebral blood flow and oxygen saturation in elderly patients undergoing carotid endarterectomy. BMC Anesthesiol 23, 153 (2023). https://doi.org/10.1186/s12871-023-02095-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-023-02095-z