
Abstract
Background
Data on the efficacy of non-invasive ventilation (NIV) after progression of respiratory failure in patients who have already received oxygen therapy, or CPAP outside ICU is limited. The study aimed to find predictors of NIV failure based on breathing pattern, gas exchange, and accessory respiratory muscles evaluation in patients who progressed to moderate-to-severe COVID-19 ARDS.
Methods
This was a prospective observational study in patients with moderate-to-severe COVID-19-ARDS on NIV (n = 80) admitted to COVID-ICU of Sechenov University. The combined success rate for conventional oxygen and CPAP outside ICU was 78.6% (440 of 560 patients). The primary endpoints were intubation rate and mortality. We measured respiratory rate, exhaled tidal volume (Vte), mean peak inspiratory flow (PIF), inspiratory time (Ti), PaO2, SpO2, end-tidal carbon dioxide (PETCO2), and Patrick score, and calculated ROX index, PaO2/FiO2, ventilatory ratio, and alveolar dead space (Vdalv/Vt) on Days 1, 3, 5, 7, 10, and 14. For all significant differences between NIV success and failure groups in measured data, we performed ROC analysis.
Results
NIV failure rate in ICU after deterioration of respiratory failure outside ICU was 71.3% (n = 57). Patients with the subsequent NIV failure were older at inclusion, more frail, had longer duration of disease before ICU admission, and higher rate of CPAP use outside ICU. ROC-analysis revealed that the following respiratory parameters after 48 h of NIV can serve as a predictors for NIV failure in moderate-to-severe COVID-19-associated ARDS: PaO2/FiO2 < 112 mmHg (AUROC 0.90 (0.93–0.97), p < 0.0001); PETCO2 < 19.5 mmHg (AUROC 0.84 (0.73–0.94), p < 0.0001); VDalv/VT > 0.43 (AUROC 0.78 (0.68–0.90), p < 0.0001); ROX-index < 5.02 (AUROC 0.89 (0.81–0.97), p < 0.0001); Patrick score > 2 points (AUROC 0.87 (0.78–0.96), p = 0.006).
Conclusion
In patients who progressed to moderate-to-severe COVID-19-ARDS probability of NIV success rate was about 1/3. Prediction of the NIV failure can be made after 48 h based on ROX index < 5.02, PaO2/FiO2 < 112 mmHg, PETCO2 < 19.5 mmHg, and Patrick score > = 2.
Trial registration
ClinicalTrials.gov identifier: NCT04667923, registered on 16/12/2020.
Similar content being viewed by others

Background
Acute respiratory failure (ARF) in COVID-19 is characterized by predominantly pulmonary dysfunction [1] and relatively low lung recruitability [2,3,4] that substantiate widespread use of noninvasive respiratory support methods such as constant positive airway pressure (CPAP), high-flow oxygen therapy (HFOT), and conventional oxygen therapy [5,6,7].
Observational studies and meta-analysis of these studies have shown high efficacy of non-invasive ventilation (NIV) in COVID-19-associated acute respiratory failure (ARF) outside the intensive care unit (ICU) [5]. The efficacy of NIV after the deterioration of respiratory failure in patients who already received conventional oxygen or CPAP outside ICU is less evident [8]. Moreover, NIV may delay tracheal intubation and increase patient self-inflicted lung injury (P-SILI), the extent of which depends on ventilatory settings, interface, and respiratory mechanics [9, 10].
Nevertheless, data on the prediction of NIV failure based on physiological respiratory parameters are limited, especially when it concerns patient respiratory drive, ventilator-derived data, alveolar dead space, and work of accessory respiratory muscles [11,12,13].
The study aimed to find predictors of NIV failure based on breathing pattern, gas exchange, and accessory respiratory muscles evaluation in patients who didn’t respond to the combination therapy of glucocorticoids + tocilizumab/olokizumab with conventional oxygen or CPAP outside ICU and progressed to moderate-to-severe COVID-19-ARDS.
Methods
Study design
This was a prospective observational clinical study (ClinicalTrials.gov NCT04667923, registered on 16/12/2020) conducted in the COVID-ICU of Sechenov University (Moscow, Russia) from October 1, 2020, to May 31, 2021. The study was approved by the Institutional Ethics Committee (reference number: 20–20, date of approval 15/07/2020). All methods were performed under the Declaration of Helsinki and the international ethical guidelines for human biomedical research. Written informed consent was waived owing to the observational nature of the study.
Patients
Patients with COVID-19-associated acute respiratory failure receiving oxygen therapy (< 15 l/min on the non-rebreather mask) or continuous positive airway pressure (CPAP) with CPAP machines with oxygen flow < 15 l/min were daily screened for eligibility. We included screened patients with at least one of the following criteria: fatigue, excessive visible work of accessory respiratory muscles assessed by Patrick scale (4–5 points) [14], SpO2 < 92%. Before the entry into the study, we performed a 2-h «NIV trial» in the ICU: we switched oxygen or CPAP therapy to non-invasive ventilation using the NIV ventilator (Trilogy 202, Philips Respironics, USA) using an oro-nasal face mask for at least 2 h to assess patients’ tolerance and need for urgent intubation (CPAP 8 (8–8) cmH2O plus Pressure Support 10 (8–12) cm H2O, FiO2 85 (70–100)%) to achieve the following: SpO2 92–96%, exhaled tidal volume < 10 ml/kg of predicted body weight (PBW), decrease in respiratory rate, and visible work of accessory respiratory muscles. Patients were enrolled in the study if they could tolerate NIV after 2 h of NIV and didn't have the signs of deterioration (e.g., fatigue, Patrick scale 4–5 points, SpO2 < 92% on FiO2 100%, respiratory rate > 35 per min, life-threatening heart rhythm abnormalities and/or systolic blood pressure < 80 mmHg despite norepinephrine at a dose > 2 μg/kg/min with signs of hypoperfusion, Glasgow coma score < 14 points). We used these signs of deterioration as intubation criteria for all patients throughout the study. Patients, who didn’t tolerate a 2-h NIV trial were urgently intubated and not included in the study. Exclusion criteria were: pregnancy, age less than 18 or more than 85 years, life-threatening heart rhythm abnormalities and/or systolic blood pressure < 80 mmHg despite norepinephrine at a dose > 2 μg/kg/min, primary lung diseases (e.g. interstitial lung diseases, lung emphysema) or tumor metastases in lungs, chronic decompensated diseases with extrapulmonary organ dysfunction (tumor progression, liver cirrhosis, congestive heart failure), Glasgow coma score < 14 points, inability to swallow, upper airways obstruction. All patients were in a self-prone position most of the time (not less than 16 h per day) [15,16,17], except patients with body mass index (BMI) > 35 kg/m2 (we placed them in lateral positions). All patients were alert or sedated in case of agitation or discomfort with a propofol infusion of 0.3–4 mg/kg/h up to the Richmond Agitation-Sedation Score (RASS) -1–2 points. All patients received methylprednisolone 1 mg/kg/day or dexamethasone 16 mg/day for at least 10 days, and interleukin-6(-receptor) inhibitors (tocilizumab 4 mg/kg or olokizumab 128 mg).
We did not change the PEEP level throughout the study. We corrected the pressure support level every day to achieve a minimum tolerable level (the Tobin index (respiratory rate/tidal volume) of less than 70) and Vte < 8 ml/kg IBW. NIV failure was determined as at least one of the following at preset Inspiratory pressure of 26 cmH2O and FiO2 100%: fatigue, Patrick scale > = 3 points, SpO2 < 92%, apnoea, hemodynamic instability, or Glasgow coma score < 14 points.
Measurements
If the patient tolerated NIV and did not have signs of deterioration after 2 h of NIV, we readjusted FiO2 to reach the target SpO2, set minimal Pressure support level to achieve Vte < 8 ml/kg IBW and Tobin index < 70, and performed the following measurements for 10 min of observation (Day 1): mean respiratory rate (RR), air leak, mean and maximum exhaled tidal volume (Vte), mean peak inspiratory flow (PIF), minimum and maximum inspiratory time (Ti), SpO2 with the ROX index calculation [6, 18,19,20,21], and work of accessory respiratory muscles by Patrick scale [14]. After that, we placed a mainstream capnograph between the mask and ventilatory circuit and asked the patient to make deep exhalation until the alveolar plateau was reached, and measured end-tidal carbon dioxide (PETCO2). The final series of the survey included measurements of the respiratory pattern parameters at higher (+ 4 cmH2O) and lower (-4 cmH2O) pressure support levels—«the inspiratory pressure trial»: the mean and maximal tidal volume, mean peak inspiratory flow, mean inspiratory time, respiratory rate, and mean minute ventilation. All measurements were repeated on days 3, 5, 7, 10, and 14. After final analysis, we retrospectively calculated the HACOR score [22] at the same time points.
In patients after NIV failure, during the first 24 h after intubation, we measured plateau pressure and calculated the driving pressure at PEEP 8–10-12–14 cm of water and VT 6 ml/kg PBW, and VT + 100 ml and VT + 200 ml at PEEP 8 cmH2O, plot static pressure volume-curve at PEEP levels of 5 and 14 cmH2O (will be published elsewhere).
Laboratory tests
After respiratory measurements, we performed arterial blood gases analysis, calculated arterial partial oxygen tension to inspiratory oxygen fraction (PaO2/FiO2) ratio, alveolar dead space (VDalv/VT), and ventilatory ratio (VR).
Endpoints and statistical analysis
The primary endpoints were intubation rate and in-hospital mortality. Secondary endpoints included: PaO2/FiO2 ratio, ventilatory ratio, ROX index, alveolar dead space, mean and maximum expired tidal volume, maximum peak inspiratory flow, and accessory respiratory muscles workload (Patrick’s scale) on Day 1, 3, 5, 7, 10, and 14 of NIV.
Descriptive statistics included proportions for categorical and median (interquartile range) for continuous variables. No imputation was made for missing data. To assess differences between NIV success and NIV failure groups, we performed the Mann–Whitney U test for continuous variables and Chi-square or Fisher exact test for categorical variables. We performed ROC analysis for NIV failure prediction in case of significant differences between groups. We used Friedman test for variable dynamics within the group. A two-sided p < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS Statistics version 27.0 (IBM, Armonk, NY, USA).
Results
We consecutively assessed for eligibility 684 and enrolled 80 patients (Fig. 1). Baseline demographic and laboratory characteristics, comorbidities, and medications of all patients and subgroups of NIV success, and NIV failure are summarised in Table 1. Patients with the subsequent NIV failure were older at inclusion, frailer, had a longer duration of disease before ICU admission, and higher incidence of CPAP therapy outside ICU (38.6% vs 8.7%) (Table 1). Clinical Frailty Score at inclusion is presented in Fig. 2. Overall, the combined success rate outside ICU for conventional oxygen and CPAP was 78.6% (440 of 560 patients)(Fig. 1).

The study cohort selection

Clinical frailty score in NIV success (green) and NIV failure (blue) groups
Primary outcomes
Non-invasive ventilation failure rate was 71.3% (n = 57). All patients in the NIV failure group were intubated and mechanically ventilated, and all patients died (3 patients died on ECMO, others were not eligible for ECMO because they met exclusion criteria for ECMO, mainly age restriction (> 65 years).
Secondary outcomes
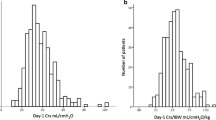
Table 2 displays respiratory parameters on day 1, 3, 5, 7, 10, and 14 in all patients, NIV success and NIV failure groups. The first day of non-invasive ventilation in our study (not less than 2 h after NIV start) was associated with PaO2/FiO2 levels corresponding to moderate-to-severe ARDS (99.9 (80.0–128.5) mmHg), high alveolar dead space with hypercapnia, high ventilatory ratio, and low ROX-index (Fig. 3, Table 2). Data on Day 1 showed significant differences in widely used oxygenation and ventilation indices between NIV success and NIV failure groups, such as PaO2/FiO2, SpO2/FiO2, VDalv/VT, ROX index, and Patrick scale (Fig. 3, Table 2). But ROC analysis for these variables on Day 1 showed poor predictive value. Surprisingly, respiratory rate and ventilatory ratio being rather high, was not different at Day 1 between groups.

The gas exchange and respiratory pattern in NIV success and NIV failure groups during 14 days. A PaO2/FiO2. B Respiratory Rate. C ROX index. D End-tidal carbon dioxide. E Alveolar dead space to tidal volume ratio. F Patrick score. Data on NIV success (green) and NIV failure (blue) are presented as medians and 95% confidence intervals (A-E), boxplots (F). The x-axis represents days after initiation of non-invasive ventilation. Abbreviations: PaO2- partial pressure of oxygen in arterial blood; FiO2—inspiratory oxygen fraction; VDalv—alveolar dead space; VT- tidal volume; PetCO2—end-tidal partial pressure of carbon dioxide. * p-value < 0.05, comparison between NIV success and NIV failure groups (Mann-Whitney U test). ** p-value < 0.01, comparison between NIV success and NIV failure groups (Mann-Whitney U test). § p-value < 0.001, comparison between NIV success and NIV failure groups (Mann-Whitney U test)
Our data and ROC analysis showed that respiratory parameters on Day 3 (approximately 48 h after inclusion) could use as predictors of NIV failure in moderate-to-severe COVID-19-associated ARDS. Patients with NIV success showed a significant increase in PaO2/FiO2, SpO2/FiO2, ROX index, and a decrease in respiratory rate and Patrick score on Day 3, while alveolar dead space in this subgroup remained stable (Table 2, Fig. 3). On the opposite, in the NIV failure group PaO2/FiO2, SpO2/FiO2, ROX index didn’t improve, the respiratory rate even increased, and the Patrick scale showed visible work of the accessory respiratory muscles (Table 2, Fig. 3). Similar data were obtained in the retrospective analysis of the HACOR score (Supplement, Table S2, Figs. S2 and S3).
We didn’t find statistically significant differences in the respiratory pattern measured by the ventilator between NIV success, and NIV failure groups except for maximal and minimal inspiratory time on Day 3 (that were shorter in NIV failure), minute ventilation on Day 3 (that were higher in NIV failure), and peak inspiratory flow in Day 5 (that was higher in NIV failure group) (Table 2). Exhaled tidal volumes were not different between groups at all study points. Patients with NIV success showed a progressive decrease in the minute ventilation (by reducing the respiratory rate), peak inspiratory flow, and increase in inspiratory time (Table 2).
Patients within the NIV failure group had 1.0 (0.5–3.0) points of the non-respiratory SOFA on the day of intubation (Table 2). In NIV success group (n = 23) and in NIV failure group (n = 57) the duration of NIV in ICU was 6 (3–10) days vs 4 (2–8) days, respectively (p = 0.103). On Day 3 100% of NIV success patients remained on NIV, while in the NIV failure group it was only 71.9%, and decreased to 45.6% by the 96 h of ICU-NIV (Day 5) (Table 2).
NIV failure prediction
ROC analysis revealed that gas exchange parameters and accessory respiratory muscles involvement (Patrick score) after 48 h of NIV could serve as a tool for the prediction of NIV failure in moderate-to-severe COVID-19-associated ARDS: PaO2/FiO2 < 112 mmHg (Se 85%, Sp 83%, AUROC 0.90 (0.93–0.97), p < 0.001); PETCO2 < 19,5 mmHg (Se 68%, Sp 83%, AUROC 0.84 (0.73–0.94), p < 0.001); VDalv/VT > 0.43 (Se 70%, Sp 70%, AUROC 0.78 (0.68–0.90), p < 0.0001); ROX-index < 5.02 (Se 78%, Sp 83%, AUROC 0.89 (0.81–0.97), p < 0.001); Patrick score > = 2 points (Se 71%, Sp 90%, AUROC 0.87 (0.78–0.96), p = 0.006)(Fig. 4). Also, increase in the peak inspiratory flow from Day 1 to Day 3 > 4.5 l/min predicted NIV failure (Se 68%, Sp 70%, AUROC 0.72 (0.60–0.85), p = 0.003)(Figure S1). Data on the NIV failure prediction by retrospectively collected HACOR score presented in Supplement (Fig. S3).

Prediction of NIV failure after 48 h basing on gas exchange and respiratory pattern parameters (ROC curves). A PaO2/FiO2. B Respiratory Rate. C ROX index. D End-tidal carbon dioxide. E Alveolar dead space to tidal volume ratio. F Patrick score. Abbreviations: PaO2- partial pressure of oxygen in arterial blood; FiO2—inspiratory oxygen fraction; VDalv—alveolar dead space; VT- tidal volume; PetCO2- end-tidal partial pressure of carbon dioxide
Odds ratios for these variables for NIV failure prediction were: 16.9 (4.6–62.4) 95% CI for ROX index < 5.02 (p < 0.001), 21.0 (5.6–78.3) 95% CI for PaO2/FiO2 < 112 mmHg (p < 0.001), 9.9 (2.8–35.0) 95% CI for PETCO2 < 19.5 mmHg (p < 0.001), 21.0 (5.6–78.3) 95% CI for Patrick score > = 2 (p < 0.003), 5.5 (2.1–20.1) 95% CI for VDalv/Vt > 43% (p < 0.001), and 4.4 (1.4–13.6) 95% CI for RR > 27 (p < 0.001) (Fig. 5).

Prediction of NIV failure after 48 h basing on gas exchange and respiratory pattern parameters (Odds ratios). Data presented as odds ratio and 95% confidence interval. Abbreviations: PaO2- partial pressure of oxygen in arterial blood; FiO2—inspiratory oxygen fraction; VDalv—alveolar dead space; VT- tidal volume; PetCO2- end-tidal partial pressure of carbon dioxide, RR—respiratory rate
The results of our study can be summarized as follows: 1. In patients who didn’t respond to the combination of glucocorticoids + tocilizumab/olokizumab with conventional oxygen or CPAP outside ICU, and progressed to moderate-to-severe COVID-19 ARDS, escalation of the respiratory support to noninvasive ventilation had about 1/3 probability of the NIV success. 2. The probability of NIV failure was higher in older and/or frail patients, in patients with a longer duration of COVID-19 before a NIV start, and, probably, in patients who didn’t respond to CPAP outside ICU (as compared to conventional oxygen). 3. In patients who didn’t respond to the combination of glucocorticoids + tocilizumab/olokizumab with conventional oxygen or CPAP outside ICU, progressed to moderate-to-severe COVID-19-ARDS, and escalated to NIV, prediction of the NIV failure must be made after 48 h based on respiratory physiological parameters such as the ROX index < 5.02, PaO2/FiO2 < 112 mmHg, PETCO2 < 19.5 mmHg, and Patrick score > = 2. 4. «The inspiratory pressure trial» had a low impact on the prediction of NIV failure (see Supplemental material). 5. The attempt to decrease pressure support level should be made in order to decrease lung strain if the patient has no signs of deterioration of the respiratory failure during such trial.
Discussion
We used noninvasive ventilation as a primary tool given mono-organ lung dysfunction, relatively low lung recruitability [2,3,4], and high risk of severe nosocomial pneumonia in these patients due to a combination of factors, such as medical immunosuppression, high prevalence of nosocomial multidrug-resistant strains, comorbidities, and advanced age. Using NIV as a primary tool, we assumed that NIV may delay the time for tracheal intubation and increase the risk of P-SILI due to higher tidal volumes and intense respiratory efforts during NIV. The summary effect of NIV in COVID-19 may be the result of mortality reduction due to less prevalence of ventilator-associated pneumonia caused by resistant strains and mortality increase due to delayed intubation because of longer exposure to P-SILI.
Spontaneous breathing during NIV/CPAP can be harmful in patients with COVID-19-ARDS due to P-SILI, although the clinical data are limited [23, 24]. We didn’t evaluate stress and strain per se but focused on some parameters that may reflect P-SILI, such as tidal volume, peak inspiratory flow, and work of accessory respiratory muscles. Some studies in non-COVID ARF have shown that tidal volumes greater than 10 ml/kg of ideal body weight have been associated with NIV failure [25]. Moreover, Pressure Support ventilation may be more harmful than CPAP [26]. In our study, mean exhaled tidal volumes were close to 7–8 ml/kg of IBW, and didn’t differ between NIV success, and NIV failure groups as in a recently published feasibility study [13]. Pressure support levels in both subgroups of the COVID-NIV study were about 6 to 10 cmH2O above the PEEP level and increased during the time course in patients with subsequent NIV failure. One might assume that strain in NIV will be higher than in HFOT. The multicenter cohort trial based on data from the first wave of the COVID-19 pandemic showed increased mortality in the subgroup of NIV as compared to standard or high-flow oxygen [27]. On the contrary, randomized trials RECOVERY-RS and HENIVOT showed reduced tracheal intubation rate in the NIV group than in the HFOT group [6, 7].
Predicting NIV failure in COVID-19-ARDS by physiological variables can draw confusing results. First of all, lung involvement, distribution of the lung infiltrates, the lung recruitability, and the risk of lung overdistension can be major factors for the efficacy and the safety of noninvasive (and invasive) ventilation. Unfortunately, data concerning physiological, lung CT or other stratification before the start of any respiratory support strategy is scarce [27,28,29,30,31]. We found the difference in the percentage of lung involvement between NIV success and NIV failure groups, but didn’t find a significant difference in the lung CT scan picture—it was predominant bilateral diffuse ground glass opacities with a low prevalence of lung consolidation, and absence of gravity-dependent distribution of the infiltrates (neither L-, nor H-phenotype) [32]. We suggest that the greater lung involvement in the NIV failure group could lead to greater lung strain. Reanalysing data of several multicenter trials on mechanical ventilation in ARDS before the COVID-19 era, Amato et al. found that low lung recruitability could predict mortality in mechanically ventilated ARDS patients [33]. In the early days of the COVID-19 pandemic, L.Gattinoni et al. postulated low (L) and highly (H) recruitable phenotypes of COVID-19-related ARF, which could be a simple tool for stratification of respiratory support [32]. After that, several physiological studies in mechanically ventilated patients with COVID-19 [2, 3] and our recently published data from observational trial COVID-VENT [4] showed low lung recruitability in patients after NIV failure. We can hypothesize that the patients in our study had low lung recruitability, which may explain the high prevalence of NIV failure.
Second, the main tool for stratification in NIV, CPAP, and HFOT studies in COVID-19-associated ARF remains the oxygenation status (for example, PaO2/FiO2 ratio), less frequently the ventilatory status (for example, ventilatory ratio and respiratory rate), or both (for example, ROX index). But the interpretation of such stratification is often misleading. Some observational and randomized studies measured FiO2 during supplemental oxygenation through the face mask [6, 29] which led to overestimation of FiO2, underestimation of PaO2/FiO2 [34], and, as a result, overestimation of the efficacy of noninvasive respiratory support especially in severe or moderate-to-severe COVID-19-ARDS. In these studies, the application of CPAP or NIV resulted in a dramatic increase in PaO2/FiO2 during the first hours. For example, in an observational study by Coppadoro et al. [29], correct measurement of FiO2 during helmet-NIV demonstrated only a 22% NIV success rate in severe and about 55% in moderate COVID-19-ARDS (as compared to 50 and 83%, respectively, when FiO2 was measured during oxygen therapy via a face mask). In the HENIVOT randomized study [6], PaO2/FiO2 increased nearly two-fold in an hour after switching from a Venturi mask to a helmet which can be at least partially explained by the correct FiO2 measurement in a bi-tube ventilatory circuit of the ICU ventilator. It’s hard to distinguish the recruitment effect and correct FiO2 measurement after switching from low-flow oxygen to NIV/CPAP in these studies. On the opposite, in our trial, oxygenation status was assessed by online FiO2 measurement in the circuit during NIV in dynamics in patients with moderate-to-severe COVID-19-associated ARF, and we found that increase in this index during 48 h after the NIV start (> 112 mmHg) associated with NIV success, possibly reflecting the potential for lung recruitment in this subgroup of patients. If we make a correct comparison of the NIV success rate between the COVID-NIV study and the study by Coppadoro et al. [29] (during the helmet phase of the study, where FiO2 measurements were taken at the helmet inlet), we would see similar results in the moderate-to-severe COVID-19-ARDS category (28.7 vs 22.0%, respectively). Post hoc analysis of the HENIVOT study showed, that more profound stratification of patients using not only PaO2/FiO2, but in combination with dyspnoea score, and PaCO2 could predict the efficacy of NIV and HFNO [30]. The ROX index in our study showed a similar cut-off value for NIV failure as it was in the original study by Roca (< 4.88) [18] and COVID-19 studies using NIV [6]. Also, we focused our attention on CO2 removal (ventilation per se). So, we found predictive values for CO2 removal impairment after 48 h of NIV, such as low PETCO2 (< 19.5 mmHg) and high alveolar dead space (> 43.0%), but not ventilatory ratio (that was 2–3 times normal without differences between NIV success and NIV failure groups). Our data on physiological predictors of NIV failure are in line with the study by Wendel-Garcia PD et al., where authors retrospectively investigated noninvasive respiratory support in COVID-19-associated ARF in 3 subgroups—standard oxygen, HFOT, and NIV [8]. In this study, patients in the NIV subgroup had moderate ARDS at the beginning of NIV (PaO2/FiO2 157 [124–205] mmHg), dead space of 51, and 88% NIV failure rate. The main difference between patients’ characteristics of the COVID-NIV study and the abovementioned study was age—patients in the COVID-NIV study were older (71.5 [62–80] vs 63 [53–69]) and therefore, probably, frailer. The PaO2/FiO2 ratio in the COVID-NIV study was less than in Wendel-Garcia’s study.
Third, only several papers focused attention on accessory respiratory muscles as a predictor of the NIV failure in COVID-19-associated ARF [35,36,37] that were based on pilot clinical observational studies without definite cut-off values for physiological variables. In our study, an increase in peak inspiratory flow and visible (even mild) work of accessory respiratory muscles were predictors of NIV failure. Similar data were obtained in a recently published pilot study by Dargent A et al., that demonstrated the feasibility of non-invasive assessment of respiratory drive and breathing pattern during a 30-min CPAP session (negative airway pressure generated during the first 100 ms of an occluded inspiration (P0.1), tidal volume, inspiratory flow, and inspiratory time), «although it was not predictive for the intubation» [13].
The next point in the discussion of predicting NIV failure and mortality is the grade of systemic inflammatory response. We would like to mention the subclass analysis of COVID-19-ARDS performed by Sinha P et al., which demonstrated a correlation between the mortality rate and the degree of systemic inflammation [38]. In their study patients with Class 2 COVID-19-ARDS had a threefold increase in the ventilatory ratio, levels of inflammatory markers, and extremely high mortality (68, or 88%, depending on corticosteroid use) [38]. This subclass of COVID-19-ARDS resembles the patients in our study.
Also, the important factors that predicted NIV failure were age and frailty, as were shown in the Italian multicenter study of noninvasive respiratory support outside ICU WARd-COVID [31]. Our study demonstrated that elderly patients with advanced COVID-19 who didn’t respond to initial respiratory support had a higher risk of NIV failure, and in these patients, intubation and mechanical ventilation did not improve the outcome.
Data on NIV success rates outside ICU can be misleading. The meta-analysis found a very high NIV success rate outside ICU overall (about 72%), but many studies excluded patients with a ‘do-not-intubate’ (DNI) order from the analysis, who accounted for about 25%, and mortality among them reached 91% [5]. In our study, we also observed high efficiency of CPAP and low-flow oxygen outside the ICU (Fig. 1), but a high level of NIV failure when CPAP therapy outside the ICU failed. We didn’t use DNI orders (out of the law in Russia), but many patients from our cohort could be classified as DNI according to comparable studies.
One might say that in our study we procrastinated intubation. Data on the influence of timing of intubation on mortality is based on observational studies only. A systematic review and meta-analysis of these studies (N = 12, n = 8944) found no significant effect of timing of intubation on the outcome, and the duration of mechanical ventilation [39]. Moreover, in a sensitivity analysis comparing «intubation without versus with a prior trial of high-flow nasal cannula, or noninvasive mechanical ventilation was still not associated with a statistically detectable difference on all-cause mortality» [39]. The observational nature of these studies and the absence of predefined criteria for NIV failure made the conclusion of the meta-analysis incomplete. Tsolaki VS et al. showed us that the duration of respiratory distress (defined as PaO2/FiO2 < 100 and/or respiratory rate > 30) can lead to the progression of COVID-19-ARDS and worse outcomes [40]. In our study, we found that a long time from disease onset and hospital admission was associated with NIV failure, which could reflect more advanced disease (greater lung involvement, as seen in Table 1) and/or lower recruitability during the time course of COVID-19 (no increase in PaO2/FiO2 in NIV failure group over time, Table 2).
Early ECMO can be lifesaving in selected patients with COVID-19 [41,42,43]. We suggest that patients with progression of COVID-19 to moderate-to-severe ARDS without improvement in gas exchange after 48 h of NIV should be considered for ECMO. Having very high mortality after NIV failure in these patients, we can speculate that NIV failure in these patients may be one of the indications for ECMO, although they can be classified as «ECMO, no, never» with comparable mortality rate, as shown by Levy D et al. in Greater Paris [44].
To summarise our physiological considerations, we can say that the high rate of NIV failure in patients of the COVID-NIV study corresponds to other studies when we compare it with the correct measurements of physiological parameters, age, and frailty.
Our study had several limitations. First of all, it had an observational design. Second, it covered predominantly elderly patients with advanced COVID-19-associated ARF with a high risk of nosocomial infection caused by resistant strains in whom initial respiratory support (low-flow oxygen or CPAP outside ICU) failed. Third, we didn’t measure markers of P-SILI such as esophageal pressure, transpulmonary pressure, functional residual capacity, or end-expiratory lung volumes.
Conclusions
In patients with COVID-19 who didn’t respond to the combination of glucocorticoids + tocilizumab/olokizumab with conventional oxygen (or CPAP) outside ICU, progressed to moderate-to-severe COVID-19-ARDS, and escalated to NIV, NIV success rate is about 30%. Prediction of NIV failure can be made after 48 h based on respiratory physiological parameters such as the ROX index < 5.02, PaO2/FiO2 < 112 mmHg, PETCO2 < 19.5 mmHg, and Patrick score > = 2.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ARDS:
-
Acute respiratory distress syndrome
- ARF:
-
Acute respiratory failure
- AUROC:
-
Area under receiver operator curve
- BMI:
-
Body mass index
- CPAP:
-
Continuous positive airway pressure
- ECMO:
-
Extracorporeal merman oxygenation
- FiO2 :
-
Inspiratory fraction of oxygen
- HFOT:
-
High-flow oxygen therapy
- IBW:
-
Ideal body weight
- ICU:
-
Intensive care unit
- NIV:
-
Noninvasive ventilation
- P0.1:
-
Negative airway pressure generated during the first 100 ms of an occluded inspiration
- PaCO2 :
-
Arterial carbon dioxide tension
- PaO2 :
-
Partial pressure of oxygen in arterial blood
- PETCO2 :
-
End-expiratory carbon dioxide tension
- PIF:
-
Peak inspiratory flow
- P-SILI:
-
Patient self-inflicted lung injury
- RASS:
-
Richmond Agitation-Sedation Score
- ROC:
-
Receiver operator curve
- RR:
-
Respiratory rate
- SpO2 :
-
Peripheral oxygen saturation
- Ti:
-
Inspiratory time
- VDalv/VT:
-
Alveolar dead space
- VR:
-
Ventilatory ratio
- VT:
-
Tidal volume
- Vte:
-
Exhaled tidal volume
References
Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW, the Northwell COVID-19 Research Consortium, Barnaby DP, Becker LB, Chelico JD, Cohen SL, Cookingham J, Coppa K, Diefenbach MA, Dominello AJ, Duer-Hefele J, Falzon L, Gitlin J, Hajizadeh N, Harvin TG, Hirschwerk DA, Kim EJ, Kozel ZM, Marrast LM, Mogavero JN, Osorio GA, Qiu M, Zanos TP. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized With COVID-19 in the New York City area. JAMA. 2020;323(20):2052–9. https://doi.org/10.1001/jama.2020.6775.
Roesthuis L, van den Berg M, van der Hoeven H. Advanced respiratory monitoring in COVID-19 patients: use less PEEP! Crit Care. 2020;24(1):230. https://doi.org/10.1186/s13054-020-02953-z.
Sella N, Zarantonello F, Andreatta G, Gagliardi V, Boscolo A, Navalesi P. Positive end-expiratory pressure titration in COVID-19 acute respiratory failure: electrical impedance tomography vs. PEEP/FiO2 tables. Crit Care. 2020;24:540.
Yaroshetskiy AI, Avdeev SN, Politov ME, Nogtev PV, Beresneva VG, Sorokin YD, Konanykhin VD, Krasnoshchekova AP, Merzhoeva ZM, Tsareva NA, Trushenko NV, Mandel IA, Yavorovskiy AG. Potential for the lung recruitment and the risk of lung overdistension during 21 days of mechanical ventilation in patients with COVID-19 after noninvasive ventilation failure: the COVID-VENT observational trial. BMC Anesthesiol. 2022;22(1):59. https://doi.org/10.1186/s12871-022-01600-0.
Cammarota G, Esposito T, Azzolina D, Cosentini R, Menzella F, Aliberti S, Coppadoro A, Bellani G, Foti G, Grasselli G, Cecconi M, Pesenti A, Vitacca M, Lawton T, Ranieri VM, Di Domenico SL, Resta O, Gidaro A, Potalivo A, Nardi G, Brusasco C, Tesoro S, Navalesi P, Vaschetto R, De Robertis E. Noninvasive respiratory support outside the intensive care unit for acute respiratory failure related to coronavirus-19 disease: a systematic review and meta-analysis. Crit Care. 2021;25(1):268. https://doi.org/10.1186/s13054-021-03697-0.
Grieco DL, Menga LS, Cesarano M, Rosà T, Spadaro S, Bitondo MM, Montomoli J, Falò G, Tonett T, Cutuli SL, Pintaudi G, Tanzarella ES, Piervincenzi E, Bongiovanni F, Dell’Anna AM, Delle Cese L, Berardi C, Carelli S, Bocci MG, Montini L, Bello G, Natalini D, De Pascale G, Velardo M, Volta CA, Ranieri VM, Conti G, Maggiore SM, Antonelli M. COVID-ICU Gemelli Study Group. Effect of Helmet Noninvasive Ventilation vs High-Flow Nasal Oxygen on Days Free of Respiratory Support in Patients With COVID-19 and Moderate to Severe Hypoxemic Respiratory Failure: The HENIVOT Randomized Clinical Trial. JAMA. 2021;325(17):1731–43. https://doi.org/10.1001/jama.2021.4682.
Perkins GD, Ji C, Connolly BA, Couper K, Lall R, Baillie JK, Bradley JM, Dark P, Dave C, De Soyza A, Dennis AV, Devrell A, Fairbairn S, Ghani H, Gorman EA, Green CA, Hart N, Hee SW, Kimbley Z, Madathil S, McGowan N, Messer B, Naisbitt J, Norman C, Parekh D, Parkin EM, Patel J, Regan SE, Ross C, Rostron AJ, Saim M, Simonds AK, Skilton E, Stallard N, Steiner M, Vancheeswaran R, Yeung J, McAuley DF, RECOVERY-RS Collaborators. Effect of noninvasive respiratory strategies on intubation or mortality among patients with acute hypoxemic respiratory failure and COVID-19: the RECOVERY-RS randomized clinical trial. JAMA. 2022;327(6):546–558;327(6):546–58. https://doi.org/10.1001/jama.2022.0028.
Wendel-Garcia PD, Mas A, González-Isern C, Ferrer R, Máñez R, Masclans JR, Sandoval E, Vera P, Trenado J, Fernández R, Sirvent JM, Martínez M, Ibarz M, Garro P, Lopera JL, Bodí M, Yébenes-Reyes JC, Triginer C, Vallverdú I, Baró A, Bodí F, Saludes P, Valencia M, Roche-Campo F, Huerta A, Cambra FJ, Barberà C, Echevarria J, Peñuelas O, Mancebo J, UCIsCAT study group. Non-invasive oxygenation support in acutely hypoxemic COVID-19 patients admitted to the ICU: a multicenter observational retrospective study. Crit Care. 2022;26(1):37. https://doi.org/10.1186/s13054-022-03905-5.
Weaver L, Das A, Saffaran S, Yehya N, Scott TE, Chikhani M, Laffey JG, Hardman JG, Camporota L, Bates DG. High risk of patient self-inflicted lung injury in COVID-19 with frequently encountered spontaneous breathing patterns: a computational modelling study. Ann Intensive Care. 2021;11(1):109. https://doi.org/10.1186/s13613-021-00904-7.
Grieco DL, Menga LS, Eleuteri D, Antonelli M. Patient self-inflicted lung injury: implications for acute hypoxemic respiratory failure and ARDS patients on non-invasive support. Minerva Anestesiol. 2019;85(9):1014-23. https://doi.org/10.23736/S0375-9393.19.13418-9.
Tonelli R, Fantini R, Tabbì L, Castaniere I, Pisani L, Pellegrino MR, Della Casa G, D’Amico R, Girardis M, Nava S, Clini EM, Marchioni A. Early inspiratory effort assessment by esophageal manometry predicts noninvasive ventilation outcome in de novo respiratory failure. A pilot study. Am J Respir Crit Care Med. 2020;202(4):558–67. https://doi.org/10.1164/rccm.201912-2512OC.
Esnault P, Cardinale M, Hraiech S, Goutorbe P, Baumstrack K, Prud’homme E, Bordes J, Forel JM, Meaudre E, Papazian L, Guervilly C. High respiratory drive and excessive respiratory efforts predict relapse of respiratory failure in critically Ill patients with COVID-19. Am J Respir Crit Care Med. 2020;202(8):1173–8. https://doi.org/10.1164/rccm.202005-1582LE.
Dargent A, Hombreux A, Roccia H, Argaud L, Cour M, Guérin C. Feasibility of non-invasive respiratory drive and breathing pattern evaluation using CPAP in COVID-19 patients. J Crit Care. 2022;69: 154020. https://doi.org/10.1016/j.jcrc.2022.154020.
Patrick W, Webster K, Ludwig L, Roberts D, Wiebe P, Younes M. Noninvasive positive-pressure ventilation in acute respiratory distress without prior chronic respiratory failure. Am J Respir Crit Care Med. 1996;153(3):1005–11. https://doi.org/10.1164/ajrccm.153.3.8630538.
Munshi L, Del Sorbo L, Adhikari NKJ, Hodgson CL, Wunsch H, Meade MO, Uleryk E, Mancebo J, Pesenti A A, Ranieri VM VM, Fan E E. Prone position for acute respiratory distress syndrome. A systematic review and meta-analysis. Ann Am Thorac Soc. 2017;14(Supplement_4):S280–8. https://doi.org/10.1513/AnnalsATS.201704-343OT.
Zang X, Wang Q, Zhou H, Liu S, Xue X, COVID-19 Early Prone Position Study Group. Efficacy of early prone position for COVID-19 patients with severe hypoxia: a single-center prospective cohort study. Intensive Care Med. 2020;46(10):1927–9. https://doi.org/10.1007/s00134-020-06182-4.
Jagan N, Morrow LE, Walters RW, Klein LP, Wallen TJ, Chung J, Plambeck RW. The Positioned study: prone positioning in nonventilated coronavirus disease 2019 patients-a retrospective analysis. Crit Care Explor. 2020;2(10): e0229. https://doi.org/10.1097/CCE.0000000000000229.
Roca O, Caralt B, Messika J, Samper M, Sztrymf B, Hernández G, García-de-Acilu M, Frat JP, Masclans JR, Ricard JD. An Index Combining Respiratory Rate and Oxygenation to Predict Outcome of Nasal High-Flow Therapy. Am J Respir Crit Care Med. 2019;199(11):1368–76. https://doi.org/10.1164/rccm.201803-0589OC.
Carteaux G, Pons M, Morin F, Tuffet S, Lesimple A, Badat B, Haudebourg AF, Perier F, Deplante Y, Guillaud C, Schlemmer F, Fois E, Mongardon N, Khellaf M, Jaffal K, Deguillard C, Grimbert P, Huguet R, Razazi K, de Prost N, Templier F, Beloncle F, Mercat A, Brochard L, Audard V, Lim P, Richard JC, Savary D, Mekontso DA. Continuous positive airway pressure for respiratory support during COVID-19 pandemic: a frugal approach from bench to bedside. Ann Intensive Care. 2021;11(1):38. https://doi.org/10.1186/s13613-021-00828-2.
Leszek A, Wozniak H, Giudicelli-Bailly A, Suh N, Boroli F, Pugin J, Grosgurin O, Marti C, Le Terrier C, Quintard H. Early measurement of ROX index in intermediary care unit is associated with mortality in intubated COVID-19 patients: a retrospective study. J Clin Med. 2022;11(2):365. https://doi.org/10.3390/jcm11020365.
Fink DL, Goldman NR, Cai J, El-Shakankery KH, Sismey GE, Gupta-Wright A, Tai CX. Ratio of oxygen saturation index to guide management of COVID-19 pneumonia. Ann Am Thorac Soc. 2021;18(8):1426–8. https://doi.org/10.1513/AnnalsATS.202008-934RL.
Duan J, Han X, Bai L, Zhou L, Huang S. Assessment of heart rate, acidosis, consciousness, oxygenation, and respiratory rate to predict noninvasive ventilation failure in hypoxemic patients. Intensive Care Med. 2017;43(2):192–9. https://doi.org/10.1007/s00134-016-4601-3.
Tobin MJ, Laghi F, Jubran A. P-SILI is not justification for intubation of COVID-19 patients. Ann Intensive Care. 2020;10(1):105.
Tobin MJ, Jubran A, Laghi F. P-SILI as justification for intubation in COVID-19: readers as arbiters. Ann Intensive Care. 2020;10(1):156.
Carteaux G, Millán-Guilarte T, De Prost N, Razazi K, Abid S, Thille AW, Schortgen F, Brochard L, Brun-Buisson C, Mekontso DA. Failure of noninvasive ventilation for de novo acute hypoxemic respiratory failure: role of tidal volume. Crit Care Med. 2016;44(2):282–90. https://doi.org/10.1097/CCM.0000000000001379.
Sakuraya M, Okano H, Masuyama T, Kimata S, Hokari S. Efficacy of non-invasive and invasive respiratory management strategies in adult patients with acute hypoxaemic respiratory failure: a systematic review and network meta-analysis. Crit Care. 2021;25(1):414. https://doi.org/10.1186/s13054-021-03835-8.
COVID-ICU group, for the REVA network, COVID-ICU investigators. Benefits and risks of noninvasive oxygenation strategy in COVID-19: a multicenter, prospective cohort study (COVID-ICU) in 137 hospitals. Crit Care. 2021;25(1):421. https://doi.org/10.1186/s13054-021-03784-2
Mauri T, Spinelli E, Scotti E, Colussi G, Basile MC, Crotti S, Tubiolo D, Tagliabue P, Zanella A, Grasselli G, Pesenti A. potential for lung recruitment and ventilation-perfusion mismatch in patients with the acute respiratory distress syndrome from Coronavirus disease 2019. Crit Care Med. 2020;48:1129–34.
Coppadoro A, Benini A, Fruscio R, Verga L, Mazzola P, Bellelli G, Carbone M, Mulinacci G, Soria A, Noè B, Beck E, Di Sciacca R, Ippolito D, Citerio G, Valsecchi MG, Biondi A, Pesci A, Bonfanti P, Gaudesi D, Bellani G, Foti G. Helmet CPAP to treat hypoxic pneumonia outside the ICU: an observational study during the COVID-19 outbreak. Crit Care. 2021;25(1):80. https://doi.org/10.1186/s13054-021-03502-y.
Grieco DL, Menga LS, Cesarano M, Spadaro S, Bitondo MM, Berardi C, Rosà T, Bongiovanni F, Maggiore SM, Antonelli M, COVID-ICU Gemelli Study Group. Phenotypes of patients with COVID-19 who have a positive clinical response to helmet noninvasive ventilation. Am J Respir Crit Care Med. 2022;205(3):360–4. https://doi.org/10.1164/rccm.202105-1212LE.
Bellani G, Grasselli G, Cecconi M, Antolini L, Borelli M, De Giacomi F, Bosio G, Latronico N, Filippini M, Gemma M, Giannotti C, Antonini B, Petrucci N, Zerbi SM, Maniglia P, Castelli GP, Marino G, Subert M, Citerio G, Radrizzani D, Mediani TS, Lorini FL, Russo FM, Faletti A, Beindorf A, Covello RD, Greco S, Bizzarri MM, Ristagno G, Mojoli F, Pradella A, Severgnini P, Da Macallè M, Albertin A, Ranieri VM, Rezoagli E, Vitale G, Magliocca A, Cappelleri G, Docci M, Aliberti S, Serra F, Rossi E, Valsecchi MG, Pesenti A, Foti G. Noninvasive ventilatory support of patients with COVID-19 outside the intensive care units (WARd-COVID). Ann Am Thorac Soc. 2021;18(6):1020–6. https://doi.org/10.1513/AnnalsATS.202008-1080OC.
Gattinoni L, Chiumello D, Caironi P, Busana M, Romitti F, Brazzi L, Camporota L. COVID-19 pneumonia: different respiratory treatments for different phenotypes? Intensive Care Med. 2020;46:1099–102.
Amato MB, Meade MO, Slutsky AS, Brochard L, Costa EL, Schoenfeld DA, Stewart TE, Briel M, Talmor D, Mercat A, Richard JC, Carvalho CR, Brower RG. Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med. 2015;372(8):747–55.
Coudroy R, Frat JP, Girault C, Thille AW. Reliability of methods to estimate the fraction of inspired oxygen in patients with acute respiratory failure breathing through non-rebreather reservoir bag oxygen mask. Thorax. 2020;75(9):805–7. https://doi.org/10.1136/thoraxjnl-2020-214863.
Apigo M, Schechtman J, Dhliwayo N, et al. Development of a work of breathing scale and monitoring need of intubation in COVID-19 pneumonia. Crit Care. 2020;24:477. https://doi.org/10.1186/s13054-020-03176-y.
Giustivi D, Bottazzini F, Belliato M. Respiratory Monitoring at Bedside in COVID-19 Patients. J Clin Med. 2021;10(21):4943. https://doi.org/10.3390/jcm10214943.
Nadeem A, Fanapour P, Apigo M, Kim S, George S. COVID-19 Pneumonia: Guiding the Decision to Intubate Based on Work of Breathing Assessment Independent of Oxygenation. Int J Crit Care Emerg Med. 2021;7:126. https://doi.org/10.23937/2474-3674/1510126.
Sinha P, Furfaro D, Cummings MJ, Abrams D, Delucchi K, Maddali MV, He J, Thompson A, Murn M, Fountain J, Rosen A, Robbins-Juarez SY, Adan MA, Satish T, Madhavan M, Gupta A, Lyashchenko AK, Agerstrand C, Yip NH, Burkart KM, Beitler JR, Baldwin MR, Calfee CS, Brodie D, O’Donnell MR. Latent class analysis reveals COVID-19-related acute respiratory distress syndrome subgroups with differential responses to corticosteroids. Am J Respir Crit Care Med. 2021;204(11):1274–85. https://doi.org/10.1164/rccm.202105-1302OC.
Papoutsi E, Giannakoulis VG, Xourgia E, et al. Effect of timing of intubation on clinical outcomes of critically ill patients with COVID-19: a systematic review and meta-analysis of non-randomized cohort studies. Crit Care. 2021;25:121. https://doi.org/10.1186/s13054-021-03540-6.
Tsolaki VS, Zakynthinos GE, Mantzarlis KD, Deskata KV, Papadonta ME, Gerovasileiou ES, Manoulakas EE, Zakynthinos E, Pantazopoulos IN, Makris DA. Driving pressure in COVID-19 acute respiratory distress syndrome is associated with respiratory distress duration before intubation. Am J Respir Crit Care Med. 2021;204(4):478–81. https://doi.org/10.1164/rccm.202101-0234LE.
Barbaro RP, MacLaren G, Boonstra PS, Iwashyna TJ, Slutsky AS, Fan E, Bartlett RH, Tonna JE, Hyslop R, Fanning JJ, Rycus PT, Hyer SJ, Anders MM, Agerstrand CL, Hryniewicz K, Diaz R, Lorusso R, Combes A, Brodie D. Extracorporeal life support organization. Extracorporeal membrane oxygenation support in COVID-19: an international cohort study of the extracorporeal life support organization registry. Lancet. 2020;396:1071–8.
Mustafa AK, Alexander PJ, Joshi DJ, Tabachnik DR, Cross CA, Pappas PS, Tatooles AJ. Extracorporeal membrane oxygenation for patients with COVID-19 in severe respiratory failure. JAMA Surg. 2020;155:990–2.
Le Breton C, Besset S, Freita-Ramos S, Amouretti M, Billiet PA, Dao M, Dumont LM, Federici L, Gaborieau B, Longrois D, Postel-Vinay P, Vuillard C, Zucman N, Lebreton G, Combes A, Dreyfuss D, Ricard JD, Roux D. Extracorporeal membrane oxygenation for refractory COVID-19 acute respiratory distress syndrome. J Crit Care. 2020;60:10–12
Levy D, Lebreton G, Pineton de Chambrun M, Hékimian G, Chommeloux J, Bréchot N, Luyt CE, Leprince P, Combes A, Schmidt M. Outcomes of patients denied extracorporeal membrane oxygenation during the COVID-19 pandemic in greater Paris, France. Am J Respir Crit Care Med. 2021;204(8):994–7. https://doi.org/10.1164/rccm.202105-1312L.
Acknowledgements
Not applicable
Funding
No funding source.
Author information
Authors and Affiliations
Contributions
AIY: study design, data collection, analysis and interpretation, script writing and revision; ZMM: data collection; NAT: data collection; NVT: data collection; GSN: data collection; VDK: data analysis and interpretation; APK: data collection; SNA: study design, data interpretation, manuscript revision. All authors revised the drafted manuscript, and all read and approved its final version.
Authors’ information
Not applicable
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Institutional Ethics Committee of Sechenov University (approval number: 20–20, date of approval 15/07/2020). All methods were performed in accordance with the Declaration of Helsinki and the international ethical guidelines for human biomedical research. Written informed consent was waived owing to the observational nature of the study. The waiver was approved by the Institutional Ethics Committee of Sechenov University (approval number: 20–20).
Consent for publication
Not applicable.
Competing interests
AIY reported personal fees from GE, Philips Respironics, Covidien, Fisher & Paykel, Drager, Triton Electronics, Mindray, Pfizer, BBraun, Gilead outside the submitted work. SNA reported personal fees from Behringer Ingelheim, Pfizer, Novartis, AstraZeneca, Chiesi outside the submitted work. No other disclosers were reported.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yaroshetskiy, A.I., Merzhoeva, Z.M., Tsareva, N.A. et al. Breathing pattern, accessory respiratory muscles work, and gas exchange evaluation for prediction of NIV failure in moderate-to-severe COVID-19-associated ARDS after deterioration of respiratory failure outside ICU: the COVID-NIV observational study. BMC Anesthesiol 22, 307 (2022). https://doi.org/10.1186/s12871-022-01847-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-022-01847-7