
Abstract
Background
The number of caesarean deliveries has been increasing. Although intrathecal morphine (ITM) can relieve pain and is widely applied in caesarean deliveries, it is associated with many side effects. Transversus abdominis plane block (TAPB), a new analgesic technology, has also began playing a certain role after caesarean delivery, with fewer adverse effects. This study mainly compares the analgesic and adverse effects of ITM and TAPB in caesarean delivery.
Methods
We systematically searched PubMed, Cochrane Library, EMBASE, and Web of Science, for randomised controlled trials (RCTs) published before 9 October, 2020 to compare the effects of ITM and TAPB. Primary outcome of the study was the pain score at rest 24 h after caesarean delivery, whereas the secondary outcomes were the pain score at movement 24 h after operation, postoperative nausea and vomiting (PONV), itching, and morphine consumption. For the outcome assessment, we conducted a sensitivity analysis.
Result
Six RCTs involving 563 patients and meeting the study inclusion criteria were included in this study. Results indicated no significant difference in the pain score between ITM and TAPB at 24 h of rest or movement. The sensitivity analysis results indicated that the resting pain score (95% CI = − 1.27 to − 0.28; P = 0.002) and 24-h moving pain score (95% CI = − 1.8 to − 0.07; P = 0.03) of the ITM group were lower than those of the TAPB group. The consumption of morphine in the ITM group was lower than in the TAPB group (95% CI = 1.92 to 4.87; P < 0.00001); however, in terms of adverse reactions, the incidence of pruritus (95% CI = 1.17 to 8.26; P = 0.02) and PONV (95% CI = 1.92 to 4.87, P < 0.00001) in the ITM group was higher than in the TAPB group.
Conclusion
Parturients in the ITM and TAPB groups exhibited similar analgesic effects. However, in the sensitivity analysis performed by eliminating the studies causing heterogeneity, the ITM group was found to have superior analgesic effects compared with the TAPB group, with less morphine consumption. Differently, the TAPB group displayed less side effects such as PONV. Therefore, TAPB is still a valuable analgesia option for patients who cannot use ITM for analgesia after caesarean delivery or those having a high risk of PONV.
Trial registration
Registration number: Registered on Prospero with the registration number of CRD42020210135.
Similar content being viewed by others

Introduction
The rate of caesarean delivery has been increasing annually because of social and psychological reasons [1]. Postoperative pain not only brings psychological torture to patients but also has a certain degree of impact on the recovery of patients after surgery and wound recovery [2, 3]. For parturients after caesarean delivery, the lack of analgesia affects the maternal postpartum recovery, breast-feeding, and baby development on the hand, whereas on the other hand, it increases the risk of postpartum depression [4, 5]. Approximately 500,000 women in Europe have been reported to experience acute postoperative pain annually [3]. Therefore, exploring effective analgesic methods for parturients after caesarean delivery is essential.
Intrathecal morphine (ITM) is considered the “gold standard” for providing analgesia after caesarean delivery. ITM can make hydrophilic morphine easily reach the cerebrospinal fluid and rapidly act on the central nervous system [6]. Therefore, the use of ITM can provide a superior analgesic effect after caesarean delivery compared with the systemic opioid analgesia technique [7, 8]. Although ITM has obvious analgesic advantages, its side effects such as nausea, vomiting, itching, and even respiratory depression restrict its further application [9, 10].
With the rapid development of the ultrasound technology, the use of transversus abdominis plane block (TAPB) in regional anaesthesia is becoming increasingly popular. Local anesthetics are mainly injected between the superficial layer of transversus abdominis plane and deep layer of internal oblique muscle, thus blocking the anterior abdominal wall afferent nerve of T6-L1 [11]. Recent studies have indicated that TAPB may play a vital role as an effective pain block of somatic surface pain induced by incision, which is much more obvious than the visceral pain caused by the traditional transverse incision [12, 13]. According to the newest PROSPECT guideline, TAPB improve pain relief, increase patient satisfaction, and result in a reduction of rescue analgesia; the potential side effects of these regional analgesic techniques are also limited, and therefore, their use is recommended for providing analgesia to patients [14].
Some meta-analyses on patient-controlled intravenous analgesia, quadratus lumborum block, and intrathecal morphine injection are available in literature. However, most of these studies have discussed the analgesic effect of a combination of TAPB and ITM. Some researchers believe that in case of postoperative analgesia with ITM, the addition of TAPB cannot further alleviate the pain. Only one meta-analysis compared the analgesic effect of TAPB and ITM after caesarean delivery [15]. Results of this meta-analysis indicated that ITM produces a superior analgesic effect compared with TAPB at rest 24 h after surgery; however, the evidence was not convincing since only two RCTs were included in the meta-analysis. In the present study, we aimed to synthesize the available data through updated systematic review and meta-analysis to assess, whether the analgesic effect and side effects of ITM differ from those of TAPB after caesarean delivery.
Methods
This systematic review and meta-analysis was conducted in accordance with the newest PRISMA recommendation [16] and was registered on Prospero (number: CRD420210135). Two researchers (YTR and HXM) searched PubMed, Cochrane Library and EMBASE from inception to 9 October, 2020 without restriction on language and region of publication. The PRISMA checklist is provided in Additional file 1.
A comprehensive search strategy by using relevant search terms, which were selected from Medical Subject Headings, EMBASE Subject Headings, and Entry terms, was employed. The databases were explored using a search algorithm with Boolean operators: ‘(transversus abdominis plane block OR transversus abdominis block OR abdominal muscle block OR TAP) AND (spinal Injections OR intrathecal injections OR intraspinal injection OR ITM) AND (caesarean section OR caesarean delivery OR abdominal deliveries OR C Section OR postcaesarean section)’.
Study selection
The determination of inclusion and exclusion criteria for selection of studies preceded our meta-analysis. Inclusion criteria were as follows: study participants comprising adult female; patients with American Society of Anesthesiologists grade ≤ 3; spinal anesthesia being the preferred mode; parturients with caesarean section/delivery; and pfannenstiel incision being the surgical approach. Exclusion criteria were as follows: observational or retrospective study; patients’ BMI ≥ 40; and study participants having a history of drug allergy and opioid tolerance. Two researchers (YTR and HXM) selected the studies meeting the inclusion criteria for full-text reading by reviewing the title and abstract. Differences at any time point were resolved by a third researcher (WRR). The authors then performed additional literature searches of the clinical trials registry (www.clinicaltrials.gov).
Data extraction
The two researchers (YTR and HXM) independently extracted the following data (Table 1): number of participants; age; weight; drugs; analgesic methods of the control and the intervention group; methods of anaesthesia; and additional medications. Discrepancies were resolved through consensus or, if necessary, through discussion with the third author (WRR).
Data were extracted for synthesis either directly from the paper through extrapolation from graphs by using Plot digitizer (http://www.plotdigitizer.sourceforge.net) or by contacting the corresponding authors for the required data, if direct extraction was not possible. We extracted continuous results as the mean and standard deviation. If no direct data were available in the original text, we extracted the data from the graph. If the median was displayed, we used Hozo and other formulas to convert the median and range into mean and standard deviation [17].
Quality of the reviewed trials was assessed using the Cochrane Risk of Bias tool independently by two of the authors (YTR and HXM).
Outcome
We considered the pain score at rest 24 h after operation as the primary outcome and converted the evaluation criteria of 0–100 points into 0–10 points for the analysis. If the data in the original article reported both the visceral and somatic scores, we selected the higher of the two pain scores for the data analysis. The pain score at movement 24 h after operation, PONV, incidence of itching, and morphine consumption were considered the secondary outcomes.
Postoperative morphine requirement was compared between the groups. Other forms of opiate analgesia were converted into intravenous morphine equivalents as follows: oral tramadol (1: 20), parenteral fentanyl (100: 1), and intravenous oxycodone (1: 1) [18, 19].
Data analysis
Continuous variables are presented as the 95% confidence interval and mean difference (MD). For presenting dichotomous variables, the odds ratio (OR) is used. The I2 value was used to evaluate the heterogeneity between the studies, and I2 of values > 50% suggested significant heterogeneity between the studies [20]. For continuous data, we determined MD. For assessing the outcome, we performed a sensitivity analysis by using the leave-one-out approach to identify the possible sources of heterogeneity. All statistical analyses were performed in Review Manager 5.3.
Risk of bias assessment
Two authors (YTR and HXM) independently assessed the methodological quality of each study by using the Cochrane Collaboration Risk of Bias tool for RCTs [21]. This tool can be used to assess random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and other biases. The risk of bias was classified as high, low, and unclear. Disagreements between the two reviewers regarding the overall risk of bias assessment were resolved through discussion and consensus.
Result
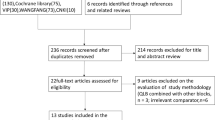
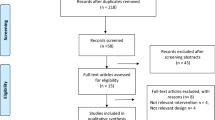
A total of 369 studies were identified through the systematic database search. After screening for duplicate studies, we obtained 338 records. Thirty full-text publications were assessed for eligibility after reviewing the title and abstract. We excluded 24 studies because the participants, interventions, or outcomes did not meet our inclusion criteria or because the study was not an RCT. Finally, we included a total of 6 RCTs for the analysis [22,23,24,25,26,27]. Figure 1 depicts a flow chart of the study selection process.

Flow chart showing selection of articles for review
Study characteristics
Table 1 summarises the characteristics and outcomes of the 6 RCTs selected according to the inclusion criteria. All included studies were published before October 2020. The sample size of these studies ranged from 40 to 180. Most of the included RCTs had used 10 mg–12.75 mg bupivacaine with or without opioid for spinal anaesthesia, and one [25] of these studies had used epinephrine additionally in the bupivacaine for spinal anaesthesia. In all the studies, the use of 0.1 mg–0.2 mg morphine in the ITM group was documented. For local blockade in the TAPB group, four RCTs [22,23,24,25] had used bupivacaine, whereas the other two trials [26, 27] had used ropivacaine. In a study comparing ITM and TAPB [25], 75 μg clonidine added as an adjuvant in combination with ropivacaine was administered to the TAPB group.
Quality assessment
Figure 2 presents the risk of bias of all the RCTs. According to the Cochrane Risk of Bias tool, four trials [22, 23, 25, 26] were found to have a high risk of bias. Of all the trials, 3 trials [23, 25, 26] exhibited a high risk of attrition bias, 2 trials [22, 26] exhibited a high risk of other bias, and one trial [22] exhibited a high risk of selection bias. Unclear risk of bias was documented in four trials [22,23,24, 27] owing to the selection bias, detection bias, attrition bias, or reporting bias.

Quality assessment of included trials. Green circle = low risk of bias; red circle = high risk of bias; yellow circle = unclear risk of bias
Primary outcome
Pain scores at rest 24 h after operation
Five studies involving 474 patients had reported pain scores at rest 24 h after surgery [22,23,24,25,26]. No significant difference was noted in the pain score between the ITM and TAPB groups (MD = − 0.47; 95% CI = − 1.33 to 0.40; I2 = 79%; P = 0.29) (Fig. 3). Results of the sensitivity analysis are presented in Table 2. The direction of the primary outcome was found to change after the RCT by Kwikiriza was excluded. The results indicated that the pain score of the ITM group was lower than that of the TAPB group, indicating that ITM produces superior analgesic effects than TAPB (MD = − 0.77; 95% CI = − 1.27 to − 0.28; I2 = 0%; P = 0.002), which further indicated that the meta-analysis has poor robustness. The source of bias is further analysed in the discussion section.

Forest plot showing pain scores at rest 24 h after surgery
Secondary outcome
Pain scores at movement 24 h after surgery
Five studies involving 474 patients had reported pain scores at movement 24 h after surgery [22,23,24,25,26]. No significant difference was observed in the pain score between the ITM and TAPB groups (MD = − 0.59; 95% CI = − 1.47 to 0.29; I2 = 83%; P = 0.19) (Fig. 4). Results of the sensitivity analysis are summarised in Table 3. After the exclusion of Kwikiriza’s RCT, the pain score of the ITM group was found to be lower than that of the TAPB group (MD = − 0.94; 95% CI = − 1.80 to − 0.07; I2 = 62%; P = 0.03), although heterogeneity between the studies was still observed. After discussion, we concluded that a high risk of attrition bias in a study [25] may be the cause of heterogeneity.

Forest plot showing pain scores at movement 24 h after surgery
PONV 24 h
The incidence of PONV was recorded in five articles, with a total of 519 (were reported) cases (Fig. 5) [22, 23, 25,26,27]. In these trials, higher incidence of postoperative nausea and/or vomiting had been reported in the ITM group than in the TAPB group, and the difference was statistically significant (OR = 3.06; 95% CI = 1.92 to 4.87; P < 0.00001; Fig. 5), with mild heterogeneity (I2 = 26%).

Forest plot showing the incidence of postoperative nausea and vomiting after surgery
Morphine consumption
A total of 287 people had reported to have consumed morphine 24 h after operation (Fig. 6) [24,25,26]. Morphine consumption between the ITM and TAPB groups was found to differ significantly (MD = − 8.04; 95% CI = − 13.12 to − 2.95; I2 = 66%; P = 0.002), which indicated that ITM analgesia causes a certain reduction in the postoperative morphine demand compared with that in the TAPB group.

Forest plot showing the consumption of morphine 24 h after surgery
Itching 24 h after surgery
Pruritus 24 h after surgery was reported in 6 studies involving 560 patients (Fig. 7) [22,23,24,25,26,27]. In one study [24], patients were asked to subjectively express whether itching or not, and the itching were graded. However, the degree of itching was not evaluated in other studies and only the number of pruritus requiring treatment was reported, which cause the high heterogeneity. Therefore, we discarded the number of people with itching that did not require treatment in this study [24], and the incidence of itching was found to be higher in the ITM group than in the TAPB group (OR = 3.11; 95% CI = 1.17 to 8.26; P = 0.02) (Fig. 7), that may be a source of heterogeneity.

Forest plot showing the incidence of itching after surgery
Discussion
In this systematic review and meta-analysis, the results of six RCTs were included to compare the analgesic effects of ITM and TAPB after caesarean delivery. The results showed no significant difference in pain scores between the ITM and TAPB groups. However, a high heterogeneity was observed across the included RCTs. Therefore, we conducted a sensitivity analysis, and after excluding a study, we found that the analgesic effect of ITM is superior to that of TAPB at rest and movement. In addition, the demand for morphine in the ITM group was found to be lesser than in the TAPB group. Although no significant difference was observed in the incidence of postoperative pruritus between the ITM and TAPB groups, the incidence of PONV was higher in the ITM group than in the TAPB group.
None of the meta-analyses have individually and systematically compared the analgesic effects of ITM and TAPB after caesarean delivery yet. Among the existing analgesic methods used after caesarean delivery, ITM is undoubtedly the first choice of anesthesiologists [28]. Although morphine can produce relatively superior analgesic effects, its adverse reactions (such as nausea, vomiting and respiratory depression) have limited its application [9]. Studies have found that morphine can be detected in the breast milk of mothers who use ITM for analgesia, which may affect newborns. Although the increased incidence of adverse events in infants during the maternal morphine treatment has not been reported, close monitoring of infants is indispensable [29]. Therefore, researchers are exploring an optimal analgesic method. With the rapid development of the ultrasound technology, ultrasound-guided TAPB has attracted extensive attention. The traditional pfannenstiel incision is chosen as the surgical approach, and its area is within the range of T6-L1 that can be blocked by TAPB, which also provides a theoretical basis for using TAPB for analgesia after caesarean section [30].
Previously, one meta-analysis was conducted to compare ITM and TAPB for multimodal analgesia after caesarean delivery [15]; however, this study focused on investigating the analgesic effects of a combination of TAPB and ITM. This meta-analysis indicated that the parturients who receive ITM and TAPB display a slight blocking effect and only the early postoperative movement pain score could be reduced. In another meta-analysis by Mishriky, although the authors had compared the analgesic effects between ITM and TAPB further analyses could not be performed and conclusions could not be derived because of the small size and excessive bias among the included studies. In the present meta-analysis, we included sufficient number of studies, evaluated the quality of included studies, compared the effects of ITM and TAPB for postcaesarean analgesia through various outcomes, and analysed the heterogeneity across studies.
In this meta-analysis, multiple outcome indicators suggest excessive heterogeneity. Using the leave-one-out method, we identified Kwikiriza’s RCT [22] as the source of heterogeneity across the studies. Possible reasons for the heterogeneity are as follows: 1. Kwikiriza’s RCT was conducted in Uganda, which is a poverty-stricken region in Africa, with limited postoperative care and resources. In this region, mothers do not receive postoperative analgesia on time, and cannot complete postoperative follow-up independently. 2. Most of the mothers in this region possess a low level of education and perceive pain as common problem; they do not actively report mild pain unless being repeatedly asked by researchers, which causes biases in the reported results.
In our meta-analysis, parturients in the ITM group displayed superior analgesic effects and less postoperative demand for morphine, however, postoperative adverse reactions were more in this group. Although the incidence of postoperative pruritus in the ITM and TAPB groups was not significantly different, the incidence of PONV in the TAPB group was much lower than in the ITM group, which is also an advantage of the TAPB technology. A suitable approach to apply the advantages of TAPB to multimodal analgesia may provide an important direction to our future research.
This study has some limitations. First, the number of included studies were small and the number of samples was insufficient. With further relevant research, our understanding of ITM and TAPB will continue to expand. In addition, one study in our meta-analysis was from a developing area, and its outcome presents a high risk of bias. Second, pregnant women with a history of caesarean delivery were not excluded, and the multipara had used ITM or TAPB for postoperative analgesia after an earlier caesarean delivery. If the randomised treatment in this study is inconsistent with the pattern previously used in multipara, they may have doubts about the analgesic effect, thus breaking the blindness. Third, different doses and concentrations of local anaesthetics had been used in the studies, and corresponding drugs such as paracetamol and dexamethasone had also been used after surgery. Although these postoperative drugs had been used in both groups, the usage of these drugs increases the complexity of the present study. Finally, he detailed information about the technique used in TAPB was not available. TAPB is completed under either ultrasound or landmark positioning; however, different methods may produce different blocking effects, and exploration of these effects may be the focus of future studies.
Conclusion
In conclusion, our meta-analysis indicated that ITM can produce superior analgesic effects in parturients after caesarean delivery and decrease the postoperative demand for morphine compared with TAPB. In addition, the incidence of itching was comparable between the groups, whereas the incidence of PONV was reported to be higher in the ITM group. Thus, TAPB could be recommended as a valuable analgesia option for patients who cannot use ITM for analgesia after caesarean delivery or those having a high risk of nausea and vomiting.
Further studies should focus on post-caesarean analgesia in developing countries. According to reports, most deliveries in the world occur in these countries [31]. However, due to the lack of personnel and economy in these countries, achieving optimum care and superior anaesthesia technology is difficult. More RCTs are needed to explore the most effective method for administering postpartum analgesia under unfavorable conditions such as lack of resources, which may also be the focus of our future study.
Availability of data and materials
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- OR:
-
Odds ratio
- CI:
-
Confidence interval
- MD:
-
Mean difference
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- RCTs:
-
Randomized controlled trials
- MeSH:
-
Medical Subject Heading
- ITM:
-
Intrathecal morphine
- TAPB:
-
Transversus abdominis plane block
- PONV:
-
Postoperative nausea and vomiting
References
Wang BS, Zhou LF, Coulter D, Liang H, Zhong Y, Guo YN, et al. Effects of caesarean section on maternal health in low risk nulliparous women: a prospective matched cohort study in Shanghai. China BMC Pregnancy Childbirth. 2010;10(1):78. https://doi.org/10.1186/1471-2393-10-78.
Leung AY. Postoperative pain management in obstetric anesthesia--new challenges and solutions. J Clin Anesth. 2004;16(1):57–65. https://doi.org/10.1016/j.jclinane.2003.02.012.
Eisenach JC, Pan PH, Smiley R, Lavand'homme P, Landau R, Houle TT. Severity of acute pain after childbirth, but not type of delivery, predicts persistent pain and postpartum depression. Pain. 2008;140(1):87–94. https://doi.org/10.1016/j.pain.2008.07.011.
Wittels B, Scot DT, Sinatra RS. Exogenous opioids in human breast Milk and acute neonatal NeurobehaviorA preliminary study. Anesthesiology. 1990;73(5):864–9. https://doi.org/10.1097/00000542-199011000-00012.
EISENACH JC, GRICE SC, DEWAN DM. Patient-controlled analgesia following cesarean SectionA comparison with epidural and intramuscular narcotics. Anesthesiology. 1988;68(3):444–7. https://doi.org/10.1097/00000542-198803000-00023.
Liu SS, Block BM, Wu CL. Effects of perioperative central Neuraxial analgesia on outcome after coronary artery bypass SurgeryA meta-analysis. Anesthesiology. 2004;101(1):153–61. https://doi.org/10.1097/00000542-200407000-00024.
Wu CL, Cohen SR, Richman JM, Rowlingson AJ, Courpas GE, Cheung K, et al. Efficacy of postoperative patient-controlled and continuous infusion epidural analgesia versus intravenous patient-controlled analgesia with OpioidsA meta-analysis. Anesthesiology. 2005;103(5):1079–88. https://doi.org/10.1097/00000542-200511000-00023.
Lim Y, Jha S, Sia A, Rawal N. Morphine for post-caesarean section analgesia: intrathecal, epidural or intravenous? Singap Med J. 2005;46(8):392–6.
Sultan P, Halpern SH, Pushpanathan E, Patel S, Carvalho B. The effect of intrathecal morphine dose on outcomes after elective cesarean delivery: a meta-analysis. Anesth Analg. 2016;123(1):154–64. https://doi.org/10.1213/ANE.0000000000001255.
Deer TR, Pope JE, Hayek SM, Lamer TJ, Veizi IE, Erdek M, et al. The Polyanalgesic consensus conference (PACC): recommendations for intrathecal drug delivery: guidance for improving safety and mitigating risks. Neuromodulation. 2017;20(2):155–76. https://doi.org/10.1111/ner.12579.
Sanderson BJ, Doane MA. Transversus abdominis plane catheters for analgesia following abdominal surgery in adults. Reg Anesth Pain Med. 2018;43(1):5–13. https://doi.org/10.1097/AAP.0000000000000681.
McDonnell JG, Curley G, Carney J, Benton A, Costello J, Maharaj CH, et al. The analgesic efficacy of transversus abdominis plane block after cesarean delivery: a randomized controlled trial. Anesth Analg. 2008;106(1):186–91 table of contents.
Canakci E, Gultekin A, Cebeci Z, Hanedan B, Kilinc A. The analgesic efficacy of transverse abdominis plane Block versus epidural Block after caesarean delivery: which one is effective? TAP Block? Epidural Block? Pain Res Manag. 2018;2018:3562701.
Roofthooft E, Joshi GP, Rawal N, Van de Velde M. Anaesthesia PWGotESoR, pain T, et al. PROSPECT guideline for elective caesarean section: updated systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2021;76(5):665–80. https://doi.org/10.1111/anae.15339.
Mishriky BM, George RB, Habib AS. Transversus abdominis plane block for analgesia after cesarean delivery: a systematic review and meta-analysis. Can J Anaesth. 2012;59(8):766–78. https://doi.org/10.1007/s12630-012-9729-1.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021;10(1):89. https://doi.org/10.1186/s13643-021-01626-4.
Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005;5(1):13. https://doi.org/10.1186/1471-2288-5-13.
Pereira J, Lawlor P, Vigano A, Dorgan M, Bruera E. Equianalgesic dose ratios for opioids: a critical review and proposals for long-term dosing. J Pain Symptom Manag. 2001;22(2):672–87. https://doi.org/10.1016/S0885-3924(01)00294-9.
Silvasti M, Rosenberg P, Seppälä T, Svartling N, Pitkänen M. Comparison of analgesic efficacy of oxycodone and morphine in postoperative intravenous patient-controlled analgesia. Acta Anaesthesiol Scand. 1998;42(5):576–80. https://doi.org/10.1111/j.1399-6576.1998.tb05169.x.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. Bmj. 2003;327(7414):557–60. https://doi.org/10.1136/bmj.327.7414.557.
Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ. 2011;343(oct18 2):d5928. https://doi.org/10.1136/bmj.d5928.
Kwikiriza A, Kiwanuka JK, Firth PG, Hoeft MA, Modest VE, Ttendo SS. The analgesic effects of intrathecal morphine in comparison with ultrasound-guided transversus abdominis plane block after caesarean section: a randomised controlled trial at a Ugandan regional referral hospital. Anaesthesia. 2019;74(2):167–73. https://doi.org/10.1111/anae.14467.
Kanazi GE, Aouad MT, Abdallah FW, Khatib MI, Adham AM, Harfoush DW, et al. The analgesic efficacy of subarachnoid morphine in comparison with ultrasound-guided transversus abdominis plane block after cesarean delivery: a randomized controlled trial. Anesth Analg. 2010;111(2):475–81. https://doi.org/10.1213/ANE.0b013e3181e30b9f.
McMorrow RCN, Ni Mhuircheartaigh RJ, Ahmed KA, Aslani A, Ng SC, Conrick-Martin I, et al. Comparison of transversus abdominis plane block vs spinal morphine for pain relief after caesarean section. Br J Anaesth. 2011;106(5):706–12. https://doi.org/10.1093/bja/aer061.
Dereu D, Savoldelli GL, Mercier Y, Combescure C, Mathivon S, Rehberg B. The impact of a transversus abdominis plane block including clonidine vs. intrathecal morphine on nausea and vomiting after caesarean section: a randomised controlled trial. Eur J Anaesthesiol. 2019;36(8):575–82. https://doi.org/10.1097/EJA.0000000000001013.
Loane H, Preston R, Douglas MJ, Massey S, Papsdorf M, Tyler J. A randomized controlled trial comparing intrathecal morphine with transversus abdominis plane block for post-cesarean delivery analgesia. Int J Obstet Anesth. 2012;21(2):112–8. https://doi.org/10.1016/j.ijoa.2012.02.005.
Jarraya A, Zghal J, Abidi S, Smaoui M, Kolsi K. Subarachnoid morphine versus TAP blocks for enhanced recovery after caesarean section delivery: a randomized controlled trial. Anaesthesia Crit Care Pain Med. 2016;35(6):391–3. https://doi.org/10.1016/j.accpm.2015.10.012.
Carvalho B. Respiratory depression after neuraxial opioids in the obstetric setting. Anesth Analg. 2008;107(3):956–61. https://doi.org/10.1213/ane.0b013e318168b443.
Ito S. Opioids in breast Milk: pharmacokinetic principles and clinical implications. J Clin Pharmacol. 2018;58(Suppl 10):S151–S63. https://doi.org/10.1002/jcph.1113.
Tsai HC, Yoshida T, Chuang TY, Yang SF, Chang CC, Yao HY, et al. Transversus abdominis plane Block: an updated review of anatomy and techniques. Biomed Res Int. 2017;2017:8284363.
Susuman AS, Chialepeh WN, Bado A, Lailulo Y. High infant mortality rate, high total fertility rate and very low female literacy in selected African countries. Scand J Public Health. 2016;44(1):2–5. https://doi.org/10.1177/1403494815604765.
Acknowledgements
Not applicable.
Funding
This research was supported by Science and Technology Department of Sichuan Province, Grant/Award Number: 2017SZ0147; 1·3·5 project for disciplines of excellence–Clinical Research Incubation Project, West China Hospital, Sichuan University, Grant/Award Number: 2018HXFH029.
Author information
Authors and Affiliations
Contributions
Tao-ran Yang made substantial contributions to conception and design of the study; Tao-ran Yang, Xue-mei He and Ru-rong Wang searched literature, extracted data from the collected literature and analysed the data; Tao-ran Yang wrote the manuscript; Xue-han Li and Ru-rong Wang revised the manuscript; all the authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
PRISMA checklist.pdf
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yang, Tr., He, Xm., Li, Xh. et al. Intrathecal morphine versus transversus abdominis plane block for caesarean delivery: a systematic review and meta-analysis. BMC Anesthesiol 21, 174 (2021). https://doi.org/10.1186/s12871-021-01392-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-021-01392-9