
Abstract
Background
Infection is a major complication following cerebral spinal fluid (CSF) diversion procedures for hydrocephalus. However, pediatric risk factors for surgical site infection (SSI) are currently not well defined. Because a SSI prevention bundle is increasingly introduced, the purpose of this study was to evaluate risk factors associated with SSIs following CSF diversion surgeries following a SSI bundle at a single quaternary care pediatric hospital.
Methods
We performed a retrospective cohort study of patients undergoing CSF diversion procedures from 2017 to 2019. SSIs were identified prospectively through continuous surveillance. We performed unadjusted logistic regression analyses and univariate analyses to determine an association between SSIs and patient demographics, comorbidities and perioperative factors to identify independent risk factors for SSI.
Results
We identified a total of 558 CSF diversion procedures with an overall SSI rate of 3.4%. The SSI rates for shunt, external ventricular drain (EVD) placement, and endoscopic third ventriculostomy (ETV) were 4.3, 6.9 and 0%, respectively. Among 323 shunt operations, receipt of clindamycin as perioperative prophylaxis and presence of cardiac disease were significantly associated with SSI (O.R. 4.99, 95% C.I. 1.27–19.70, p = 0.02 for the former, and O.R. 7.19, 95% C.I. 1.35–38.35, p = 0.02 for the latter). No risk factors for SSI were identified among 72 EVD procedures.
Conclusion
We identified receipt of clindamycin as perioperative prophylaxis and the presence of cardiac disease as risk factors for SSI in shunt procedures. Cefazolin is recommended as a standard antibiotic for perioperative prophylaxis. Knowing that unsubstantiated beta-lactam allergy label is a significant medical problem, efforts should be made to clarify beta-lactam allergy status to maximize the number of patients who can receive cefazolin for prophylaxis before shunt placement. Further research is needed to elucidate the mechanism by which cardiac disease may increase SSI risk after shunt procedures.
Similar content being viewed by others

Introduction
Hydrocephalus results from a disturbance of the normal pulsatile flow of cerebrospinal fluid (CSF), resulting in its abnormal accumulation within the cerebral ventricles. This can be alleviated in the short term by insertion of a reservoir or external ventricular drain (EVD). Long term, definitive treatment is most commonly accomplished by placement of a ventriculoperitoneal shunt (VPS) or by endoscopic third ventriculostomy (ETV) with or without choroid plexus cauterization (CPC) [1]. Although the rate of surgical site infections (SSIs) after neurosurgery is generally low, the clinical and financial consequences of SSIs after CSF diversion procedures are substantial [2]. Infections following neurosurgery can lead to significant complications such as seizures, neurological deficits, and malfunction of the shunt device [3, 4]. Therefore, the prevention of infection is a priority for managing these patients, and research over the years has identified modifiable risk factors and interventions [5,6,7,8]. However, infections still persist, and greater effort needs to be directed towards understanding risk factors in order to identify new ways to lower SSI rates. To compare what has been reported with our recent experience, we conducted an observational, retrospective study to identify factors associated with SSIs after CSF diversion procedures in a pediatric cohort in a single institution.
Materials and methods
Study cohort and patient background
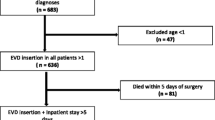
This retrospective cohort study was approved by the Institutional Review Board (IRB) at Boston Children’s Hospital (BCH). The need of the informed consent was waived. All the study methods were carried out in accordance with institutional guidelines and regulations. We identified patients who underwent CSF diversion surgery (shunts, EVD, ETV) at BCH from January 2017 to September 2019. We included cases with either congenital or acquired hydrocephalus, including communicating and noncommunicating hydrocephalus. We also included patients with a history of brain tumor who subsequently needed CSF diversion, but excluded patients who underwent craniotomy for tumor resection at the time of CSF diversion surgery. Our SSI prevention bundle consisted of 4 elements: 1) Preoperative bath using soap or an antiseptic agent; 2) Skin preparation with chlorhexidine gluconate (CHG)-alcohol (ChloraPrep™), povidone-iodine alone, povidone-iodine plus CHG-alcohol, povidone-iodine plus alcohol, or all three antiseptics in combination; 3) Using clippers for hair removal; and 4) Perioperative antibiotic prophylaxis. Cefazolin was the standard antibiotic for surgical prophylaxis unless patients had a previous history of bacterial infections that would direct other choices, or patients were previously known to have reactions to penicillin or cephalosporins, and the dose was administered within 60 min prior to skin incision. When SSIs were suspected, wounds and/or CSF were cultured at the medical team and/or surgeon’s discretion. SSIs associated with CSF diversion procedures were identified through ongoing prospective surveillance by the Infection Prevention and Control department using National Healthcare Safety Network (NHSN) definitions from the US Centers for Disease Control and Prevention (CDC) [9]. Prospective surveillance for 90 days following an operation is done by Infection Prevention and Control. For ETV, we included SSI diagnosed within 30 days after surgery. For shunt and EVD procedures, both of which involve implants, we included SSI diagnosed within 90 days after surgery. When a patient had a repeated operation on different dates within the time frame of 90-day observation, the SSI was attributed to the most recently performed procedure according to NHSN definitions. We extracted the information on the demographics and comorbidities of the study cohort from the electronic medical records and we obtained intraoperative information such as medications, surgical duration and American Society of Anesthesiology (ASA) physical status classifications from the Anesthesia Information Management System™ (AIMS; Cerner, MO, USA) to obtain. Comorbidities were based on the International Classification of Diseases (ICD)-9 / ICD-10 codes. Congenital cardiac diseases, great vessel malformations, and cardiomyopathies were categorized as cardiac diseases. There were a total of 10 surgeons.
Statistical analysis
We reported continuous variables as either means with standard deviation (SD) for normally distributed variables or medians and interquartile ranges (IQR) for variables without normal distribution. Normality of distribution was determined by Shapiro-Wilk test. Binary and categorical variables were reported using frequencies and percentages. We performed an unadjusted logistic regression analysis with SSI as the dependent variable. The effect was quantified by the odds ratio (OR) per 1-unit change in the predictor variable. If the outcome was zero or if logistic regression analysis for each categorical variable was not fit, we performed univariate analysis. We used Fisher’s exact test to compare proportions for categorical variables, and t-tests or Mann–Whitney U tests to compare means or medians for continuous variables. All hypothesis testing had a two-sided significance level of 0.05. All statistical analyses were conducted using Stata/MP 15.0 (StataCorp, College Station, TX, USA).
Results
Among 558 CSF diversion procedures in 306 unique patients, 19 infections occurred, yielding an SSI rate of 3.4%. Characteristics of the study cohort are shown in Table 1. The SSI rates for shunt, EVD, and ETV were 4.3, 6.9, and 0%, respectively. The median number of days from surgery to the onset of SSI was 13.5 days (IQR: 5.5, 30), with a maximum of 89 days. The median number of days from surgery to the onset of SSI was 18.5 and 9 days for shunt and EVD, respectively.
Table 2 shows all available variables and their association with SSIs in shunt procedures. In unadjusted logistic regression analysis, factors that were significantly associated with infection in shunt surgery were the administration of clindamycin as perioperative prophylaxis (O.R. 4.99, 95% C.I. 1.27–19.70, p = 0.02) and the presence of congenital heart disease (O.R. 7.19, 95% C.I. 1.35–38.35, p = 0.02). Cardiac diseases present among patients with SSI included single ventricle disease with palliative repair and valvulopathy with underlying connective tissue diseases. None of the perioperative factors, including the duration of procedure, surgeon, or type of skin preparation agent were associated with SSIs.
Table 3 displays all available variables evaluated for potential association with SSI following EVD procedures. No variables in this analysis were significantly associated with SSIs. There was no SSI that occurred among patients undergoing ETV.
Table 4 presents the CSF culture results for patients with SSIs. Staphylococcus epidermidis (14.3%) and Cutibacterium acnes (formerly Propionibacterium acnes) (14.3%) were detected most frequently. From the 19 positive CSF cultures, 14 unique bacterial and fungal species were identified.
Discussion
In this study, we investigated risk factors for pediatric SSIs after CSF diversion surgery at a single quaternary care pediatric center. We found that receipt of clindamycin for perioperative prophylaxis and comorbid cardiac disease were significantly associated with SSI in shunt surgery.
In our study, the incidence of SSI in combined CSF diversion surgery was 3.4%, while SSI rates for shunt surgery, EVD, and ETV were 4.3, 6.9, and 0%, respectively. EVD is a device placed to manage intracranial pressure when normal flow of CSF inside the brain is hindered. Because it is externalized, it is not surprising that EVD was associated with the highest infection rate among these procedure types. ETV is an important procedure for hydrocephalus that serves as an alternative to shunt device implantation. The success rate of ETV and its use in various ages and background diseases vary across reports [10]. ETV can be done with or without CPC. In our institution, CPC is generally done together with ETV. In general, the SSI rate of ETV is lower than that of a shunt device implantation procedure, but the post-ETV SSI rate depends on background and age [11]. In our institution, ETV was often performed for hydrocephalus due to congenital diseases in infancy, but it was also performed in cases of repeated shunting and brain tumor complications.
Research on modifiable perioperative risk factors and interventions to reduce the risk of shunt infection has been done for many years. Traditional risk factors include the duration of surgery [12], the experience of the surgeon [13], hair shaving [14], prophylactic systemic antibiotics [8, 15], antibiotic-impregnated sutures [16] and skin preparation [5, 6]. In our cohort, surgeon, duration of surgery, and skin preparation agent were not associated with SSIs. In addition, our institution routinely utilizes antibiotic-impregnated shunt tubing (Bactiseal tubing) [17, 18]. Receipt of clindamycin for prophylaxis was significantly associated with SSI. Cefazolin is the standard, first line prophylactic antibiotic choice for shunt operations, but other antibiotics are used when patients are thought to have penicillin or cephalosporin allergy. The spectrum of activity of clindamycin includes staphylococci, streptococci, pneumococci, and some anaerobic bacteria. However, it does not have activity against aerobic Gram negative bacteria. It is well known that unsubstantiated penicillin allergy labels are common in surgical patients. Up to 98% of patients labeled as allergic to penicillin can actually safely receive the antibiotic when tested [19]. Similarly, gastrointestinal upset is often listed as a reason for allergy to cephalosporins. In women with chorioamnionitis undergoing cesarean delivery, the use of cefazolin was associated with a lower incidence of postpartum infection than the use of clindamycin [20]. Although our study is from a single institution, this finding highlights the importance of obtaining a detailed history of antibiotic allergies and considering de-labeling strategies in order to maximize the number of patients who can successfully receive beta-lactam antibiotics for perioperative prophylaxis.
The association of cardiac diseases with shunt infection was previously described in a study of children who underwent shunt surgery within the first year of life [21]. Our study consisting of older children also demonstrated that comorbid cardiac disease was associated with an increased risk of shunt SSI. Cardiac diseases present among our patients with SSI included single ventricle disease with palliative repair [22] and valvulopathy with underlying connective tissue diseases. Although not directly related to infection, cardiac anomalies were associated with shunt failure in the prospective study of children from six Hydrocephalus Clinical Research Network Centers [23]. The authors suggested that this finding may be related to repeated hospitalizations and surgeries or immunodeficiency, but they did not formally analyze these exposures. For example, thymectomy is often performed to have better visualization in neonatal and infant cardiac surgeries [24], but it may have some immunological impact [25]. Immunological profiles for patients with a cardiac disease who present for CSF diversion procedures are not known, and could be a topic of future investigation.
The association between age and SSIs varies across studies. While some studies have identified younger age, particularly infancy, as a risk factor for SSI [26,27,28,29], other studies have demonstrated that age is not a risk factor for shunt failure or infection [30, 31]. Post- intraventricular hemorrhage (IVH) hydrocephalus secondary to prematurity occurs in infants, but older children may have different etiology of hydrocephalus including tumor-related hydrocephalus. In our cohort, age was not a risk factor. Most of the patients in our cohort were beyond infancy, and our results may not generalize to premature infants for that reason.
The risk of shunt failure or infection generally increases with each subsequent shunt replacement, resulting in a rising cumulative risk of SSIs [29, 32, 33]. However, in the present study, the number of shunt revisions was not a risk factor for SSIs. Previously, other investigators found that the presence of a gastrostomy tube was associated with infection risk in the larger study [32], but this did not substantially contribute to infections in this study. Some studies showed that lower gestational age (GA) at the time of procedures and prematurity were significant risk factors for infection after shunt surgery [7, 28]. In our study cohort, there was no incidence of SSIs in patients with a history of preterm birth, although a number of patients did not have detailed perinatal information available. Although it is difficult to determine the association between GA at birth and SSIs, GA was not a risk factor for SSI in our study. Further investigation is needed to clarify why our result differs from the previous reports.
Among the perioperative factors other than those mentioned above, there have been no reports that have examined the type and dose of anesthetics and the amount of oxygen administered in shunt surgery. Intraoperative factors such as oxygen dosage, and temperature control are known to play a role in SSI following adult general surgery [34,35,36]. The effect of volatile anesthetics on immune function have been reported previously [37,38,39,40,41,42,43,44]. In our previous work using a preclinical model, a long exposure (6-h) of volatile anesthetics was associated with increased infection, while a short exposure (2-h) was not [45]. In a study at our institution, we previously showed that higher volatile anesthetic dose was an independent risk factor for SSI in pediatric gastrointestinal surgery [46]. Anesthetic drugs and oxygen dosage also had no impact on the incidence of SSIs. The operative duration was less than 80 min for the groups with and without SSIs. Our result was in line with the finding in our preclinical study. In the present study, the median number of days to the date of SSI onset after surgery was 13.5 days, but more than 75% of the patients with SSI had a postoperative period of more than 30 days. In previous reports, the risk of infection was shown to be highest in the first 8 weeks after a shunt procedure, and the risk decreased substantially after 6 months [47]. Because of relatively late onset of SSI postoperatively and the short surgical duration, it is perhaps not surprising that the impact of intraoperative drugs and oxygen dose on immune function was less after CSF diversion surgery.
The most common bacteria detected in our cohort were Staphylococcus epidermidis and Cutibacterium acnes, generally consistent with previous reports [26, 27, 48, 49]. Staphylococcus aureus was detected in a smaller proportion of cases. While the effectiveness of antimicrobial-impregnated and -coated shunts (AIS) has been described [15, 49], there are concerns including the emergence of methicillin-resistant Staphylococcus aureus (MRSA) and resistant gram negative rods (GNR) with repeated use [48, 49]. Although we routinely use antimicrobial impregnated shunting, MRSA was not detected in our cohort.
Our study has several limitations. First, it was limited as a single-center study and was retrospective. Second, the low SSI rate and small sample size may impair statistical power to find associations.
In conclusion, we have shown that receipt of clindamycin as prophylaxis was significantly associated with SSI in children undergoing shunt surgery. Because unsubstantiated allergy labeling for penicillin and other antibiotics are common in surgical patients, efforts should be made to identify which patients can successfully receive a beta-lactam antibiotic for perioperative prophylaxis. Further research is needed to better define the mechanism by which cardiac disease is associated with SSI among patients undergoing neurosurgical shunt procedures.
Availability of data and materials
All the data and materials are available upon request.
References
Kahle KT, Kulkarni AV, Limbrick DD Jr, Warf BC. Hydrocephalus in children. Lancet. 2016;387(10020):788–99. https://doi.org/10.1016/S0140-6736(15)60694-8.
Simon TD, Riva-Cambrin J, Srivastava R, Bratton SL, Dean JM, Kestle JR. Hospital care for children with hydrocephalus in the United States: utilization, charges, comorbidities, and deaths. J Neurosurg Pediatr. 2008;1(2):131–7. https://doi.org/10.3171/PED/2008/1/2/131.
Mapstone T, Rekate H, Nulsen F, Dixon M, Glaser N, Jaffe M. Relationship of CSF shunting and IQ in children with myelomeningocele: a retrospective analysis. Childs Brain. 1984;11(2):112–8. https://doi.org/10.1159/000120166.
Vanaclocha V, Sáiz-Sapena N, Leiva J. Shunt malfunction in relation to shunt infection. Acta Neurochir. 1996;138(7):829–34. https://doi.org/10.1007/BF01411261.
Hommelstad J, Madsø A, Eide PK. Significant reduction of shunt infection rate in children below 1 year of age after implementation of a perioperative protocol. Acta Neurochir. 2013;155(3):523–31. https://doi.org/10.1007/s00701-012-1574-z.
Kestle JR, Riva-Cambrin J, Wellons JC 3rd, Kulkarni AV, Whitehead WE, Walker ML, et al. A standardized protocol to reduce cerebrospinal fluid shunt infection: the hydrocephalus clinical Research network quality improvement initiative. J Neurosurg Pediatr. 2011;8(1):22–9. https://doi.org/10.3171/2011.4.PEDS10551.
Spader HS, Hertzler DA, Kestle JR, Riva-Cambrin J. Risk factors for infection and the effect of an institutional shunt protocol on the incidence of ventricular access device infections in preterm infants. J Neurosurg Pediatr. 2015;15(2):156–60. https://doi.org/10.3171/2014.9.PEDS14215.
Klimo P Jr, Van Poppel M, Thompson CJ, Baird LC, Duhaime AC, Flannery AM. Pediatric hydrocephalus: systematic literature review and evidence-based guidelines. Part 6: Preoperative antibiotics for shunt surgery in children with hydrocephalus: a systematic review and meta-analysis. J Neurosurg Pediatr. 2014;14(Suppl 1):44–52.
Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, 1999. Am J Infect Control. 1999;27(2):97–134. https://doi.org/10.1016/S0196-6553(99)70088-X.
Zaben M, Manivannan S, Sharouf F, Hammad A, Patel C, Bhatti I, et al. The efficacy of endoscopic third ventriculostomy in children 1 year of age or younger: a systematic review and meta-analysis. Eur J Paediatr Neurol. 2020;26:7–14. https://doi.org/10.1016/j.ejpn.2020.02.011.
Labidi M, Lavoie P, Lapointe G, Obaid S, Weil AG, Bojanowski MW, et al. Predicting success of endoscopic third ventriculostomy: validation of the ETV success score in a mixed population of adult and pediatric patients. J Neurosurg. 2015;123(6):1447–55. https://doi.org/10.3171/2014.12.JNS141240.
Kontny U, Höfling B, Gutjahr P, Voth D, Schwarz M, Schmitt H. CSF shunt infections in children. Infection. 1993;21(2):89–92. https://doi.org/10.1007/BF01710738.
Cochrane D, Kestle J. The influence of surgical operative experience on the duration of first ventriculoperitoneal shunt function and infection. Pediatr Neurosurg. 2003;38(6):295–301. https://doi.org/10.1159/000070413.
Ratanalert S, Musikawat P, Oearsakul T, Saeheng S, Chowchuvech V. Non-shaved ventriculoperitoneal shunt in Thailand. J Clin Neurosci. 2005;12(2):147–9. https://doi.org/10.1016/j.jocn.2004.03.024.
Klimo P Jr, Thompson CJ, Baird LC, Flannery AM. Pediatric hydrocephalus: systematic literature review and evidence-based guidelines. Part 7: Antibiotic-impregnated shunt systems versus conventional shunts in children: a systematic review and meta-analysis. J Neurosurg Pediatr. 2014;14(Suppl 1):53–9.
Sciubba D, Lin L, Woodworth G, McGirt M, Carson B, Jallo G. Factors contributing to the medical costs of cerebrospinal fluid shunt infection treatment in pediatric patients with standard shunt components compared with those in patients with antibiotic impregnated components. Neurosurg Focus. 2007;22(4):E9. https://doi.org/10.3171/foc.2007.22.4.11.
Mallucci CL, Jenkinson MD, Conroy EJ, Hartley JC, Brown M, Dalton J, et al. Antibiotic or silver versus standard ventriculoperitoneal shunts (BASICS): a multicentre, single-blinded, randomised trial and economic evaluation. Lancet. 2019;394(10208):1530–9. https://doi.org/10.1016/S0140-6736(19)31603-4.
Parker SL, McGirt MJ, Murphy JA, Megerian JT, Stout M, Engelhart L. Comparative effectiveness of antibiotic-impregnated shunt catheters in the treatment of adult and pediatric hydrocephalus: analysis of 12,589 consecutive cases from 287 US hospital systems. J Neurosurg. 2015;122(2):443–8. https://doi.org/10.3171/2014.10.JNS13395.
Savic LC, Khan DA, Kopac P, Clarke RC, Cooke PJ, Dewachter P, et al. Management of a surgical patient with a label of penicillin allergy: narrative review and consensus recommendations. Br J Anaesth. 2019;123(1):e82–94. https://doi.org/10.1016/j.bja.2019.01.026.
Venkatesh KK, Hughes BL, Grotegut CA, Strauss RA, Stamilio DM, Heine RP, et al. Preoperative cefazolin rather than clindamycin or metronidazole is associated with lower postpartum infection among women with chorioamnionitis delivering by cesarean delivery. Am J Obstet Gynecol MFM. 2020;2(1):100074. https://doi.org/10.1016/j.ajogmf.2019.100074.
Kebriaei MA, Shoja MM, Salinas SM, Falkenstrom KL, Sribnick EA, Tubbs RS, et al. Shunt infection in the first year of life. J Neurosurg Pediatr. 2013;12(1):44–8. https://doi.org/10.3171/2013.4.PEDS12616.
Yuki K, Casta A, Uezono S. Anesthetic management of noncardiac surgery for patients with single ventricle physiology. J Anesth. 2011;25(2):247–56. https://doi.org/10.1007/s00540-010-1081-4.
Riva-Cambrin J, Kestle JR, Holubkov R, Butler J, Kulkarni AV, Drake J, et al. Risk factors for shunt malfunction in pediatric hydrocephalus: a multicenter prospective cohort study. J Neurosurg Pediatr. 2016;17(4):382–90. https://doi.org/10.3171/2015.6.PEDS14670.
Whiting D, Yuki K, DiNardo JA. Cardiopulmonary bypass in the pediatric population. Best Pract Res Clin Anaesthesiol. 2015;29(2):241–56. https://doi.org/10.1016/j.bpa.2015.03.006.
Kurobe H, Tominaga T, Sugano M, Hayabuchi Y, Egawa Y, Takahama Y, et al. Complete but not partial thymectomy in early infancy reduces T-cell-mediated immune response: three-year tracing study after pediatric cardiac surgery. J Thorac Cardiovasc Surg. 2013;145(3):656–62 662 e651–652; discussion 662.
Davis SE, Levy ML, McComb JG, Masri-Lavine L. Does age or other factors influence the incidence of ventriculoperitoneal shunt infections? Pediatr Neurosurg. 1999;30(5):253–7. https://doi.org/10.1159/000028806.
Pople IK, Bayston R, Hayward RD. Infection of cerebrospinal fluid shunts in infants: a study of etiological factors. J Neurosurg. 1992;77(1):29–36. https://doi.org/10.3171/jns.1992.77.1.0029.
Bruinsma N, Stobberingh EE, Herpers MJ, Vles JS, Weber BJ, Gavilanes DA. Subcutaneous ventricular catheter reservoir and ventriculoperitoneal drain-related infections in preterm infants and young children. Clin Microbiol Infect. 2000;6(4):202–6. https://doi.org/10.1046/j.1469-0691.2000.00052.x.
Simon TD, Hall M, Riva-Cambrin J, Albert JE, Jeffries HE, Lafleur B, et al. Infection rates following initial cerebrospinal fluid shunt placement across pediatric hospitals in the United States. Clinical article. J Neurosurg Pediatr. 2009;4(2):156–65. https://doi.org/10.3171/2009.3.PEDS08215.
Simon T, Whitlock K, Riva-Cambrin J, Kestle J, Rosenfeld M, Dean J. Association of intraventricular hemorrhage secondary to prematurity with cerebrospinal fluid shunt surgery in the first year following initial shunt placement. J Neurosurg Pediatr. 2012;9(1):54–63. https://doi.org/10.3171/2011.10.PEDS11307.
Piatt J, Carlson C. A search for determinants of cerebro spinal fluid shunt survival: retrospective analysis of a 14-year institutional experience. Pediatr Neurosurg. 1993;19(5):233–42. https://doi.org/10.1159/000120738.
Simon TD, Butler J, Whitlock KB, Browd SR, Holubkov R, Kestle JRW, et al. Risk factors for first cerebrospinal fluid shunt infection: findings from a multi-center prospective cohort study. J Pediatr. 2014;164(6):1462–1468.e1462.
Tuli S, Drake J, Lawless J, Wigg M, Lamberti-Pasculli M. Risk factors for repeated cerebrospinal shunt failures in pediatric patients with hydrocephalus. J Neurosurg. 2000;92(1):31–8. https://doi.org/10.3171/jns.2000.92.1.0031.
Melling AC, Ali B, Scott EM, Leaper DJ. Effects of preoperative warming on the incidence of wound infection after clean surgery: a randomised controlled trial. Lancet. 2001;358(9285):876–80.
Greif R, Akca O, Horn EP, Kurz A, Sessler DI, Outcomes Research G. Supplemental perioperative oxygen to reduce the incidence of surgical-wound infection. N Engl J Med. 2000;342(3):161–7. https://doi.org/10.1056/NEJM200001203420303.
Koo BW, Sim JB, Shin HJ, Kim DW, Kang SB, Do SH, et al. Surgical site infection after colorectal surgery according to the main anesthetic agent: a retrospective comparison between volatile anesthetics and propofol. Korean J Anesthesiol. 2016;69(4):332–40. https://doi.org/10.4097/kjae.2016.69.4.332.
Yuki K, Eckenhoff RG. Mechanisms of the immunological effects of volatile anesthetics: a review. Anesth Analg. 2016;123(2):326–35. https://doi.org/10.1213/ANE.0000000000001403.
Yuki K, Murakami N. Sepsis pathophysiology and anesthetic consideration. Cardiovasc Hematol Disord Drug Targets. 2015;15(1):57–69. https://doi.org/10.2174/1871529X15666150108114810.
Yuki K, Bu W, Shimaoka M, Eckenhoff R. Volatile anesthetics, not intravenous anesthetic propofol bind to and attenuate the activation of platelet receptor integrin alphaIIbbeta3. PLoS One. 2013;8(4):e60415. https://doi.org/10.1371/journal.pone.0060415.
Yuki K, Bu W, Xi J, Sen M, Shimaoka M, Eckenhoff RG. Isoflurane binds and stabilizes a closed conformation of the leukocyte function-associated antigen-1. FASEB J. 2012;26(11):4408–17. https://doi.org/10.1096/fj.12-212746.
Tazawa K, Koutsogiannaki S, Chamberlain M, Yuki K. The effect of different anesthetics on tumor cytotoxicity by natural killer cells. Toxicol Lett. 2017;266:23–31. https://doi.org/10.1016/j.toxlet.2016.12.007.
Carbo C, Yuki K, Demers M, Wagner DD, Shimaoka M. Isoflurane inhibits neutrophil recruitment in the cutaneous Arthus reaction model. J Anesth. 2013;27(2):261–8. https://doi.org/10.1007/s00540-012-1508-1.
Yuki K, Bu W, Xi J, Shimaoka M, Eckenhoff R. Propofol shares the binding site with isoflurane and sevoflurane on leukocyte function-associated antigen-1. Anesth Analg. 2013;117(4):803–11. https://doi.org/10.1213/ANE.0b013e3182a00ae0.
Yuki K, Soriano SG, Shimaoka M. Sedative drug modulates T-cell and lymphocyte function-associated antigen-1 function. Anesth Analg. 2011;112(4):830–8. https://doi.org/10.1213/ANE.0b013e31820dcabb.
Koutsogiannaki S, Schaefers MM, Okuno T, Ohba M, Yokomizo T, Priebe GP, et al. From the cover: prolonged exposure to volatile anesthetic Isoflurane worsens the outcome of Polymicrobial abdominal Sepsis. Toxicol Sci. 2017;156(2):402–11.
Shibamura-Fujiogi M, Ormsby J, Breibart M, Zalieckas J, Sandora TJ, Priebe GP, et al. The role of anesthetic Management in Surgical Site Infections after Pediatric Intestinal Surgery. J Surg Res. 2021;259:546–54. https://doi.org/10.1016/j.jss.2020.10.015.
Mancao M, Miller C, Cochrane B, Hoff C, Sauter K, Weber E. Cerebrospinal fluid shunt infections in infants and children in Mobile, Alabama. Acta Paediatr. 1998;87(6):667–70.
Simon TD, Kronman MP, Whitlock KB, Browd SR, Holubkov R, Kestle JRW, et al. Patient and treatment characteristics by infecting organism in cerebrospinal fluid shunt infection. J Pediatr Infect Dis Soc. 2019;8(3):235–43. https://doi.org/10.1093/jpids/piy035.
Konstantelias AA, Vardakas KZ, Polyzos KA, Tansarli GS, Falagas ME. Antimicrobial-impregnated and -coated shunt catheters for prevention of infections in patients with hydrocephalus: a systematic review and meta-analysis. J Neurosurg. 2015;122(5):1096–112. https://doi.org/10.3171/2014.12.JNS14908.
Acknowledgements
We thank Dr. Lifei Hou and Dr. Sophia Koutsogiannaki (both Boston Children’s Hospital) for discussion.
Funding
This study was in part supported by R01 GM127600 (K.Y.).
Author information
Authors and Affiliations
Contributions
MSF: Designed the study, analyzed the data, and wrote the manuscript; JO: Designed the study and collected the data.; MB: Collected the data.; BW: Wrote the manuscript.; GPP: Analyzed the data and wrote the manuscript;SGS: Analyzed the data and wrote the manuscript.; TJS: Analyzed the data and wrote the manuscript; KY: Designed the study, analyzed the data and wrote the manuscript. The authors read and approved the final manuscript.
Authors’ information
MSF: Research fellow; JO: Infectious disease nurse.; MB: Clinical research database specialist.; BW: Professor in neurosurgery.; GPP: Associate Professor in Anesthesia; SGS: Professor in Anesthesia.; TJS: Associate Professor in Pediatrics; KY: Associate Professor in Anesthesia.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Our study was approved by our institutional review board. Informed consent was waived.
Consent for publication
The institutional review provided us the consent to publish.
Competing interests
We do not have any conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shibamura-Fujiogi, M., Ormsby, J., Breibart, M. et al. Risk factors for pediatric surgical site infection following neurosurgical procedures for hydrocephalus: a retrospective single-center cohort study. BMC Anesthesiol 21, 124 (2021). https://doi.org/10.1186/s12871-021-01342-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-021-01342-5