
Abstract
Background
Common Variable Immunodeficiency (CVID) is a primary immunodeficiency syndrome resulting in recurrent infections, autoimmunity, and granulomatous manifestations.
Methods and materials
This retrospective study was conducted on an Iranian national registry of immunodeficient patients from 2010 to 2021. The frequency of first presentations of CVID and its association with sex, age of onset, and family history of CVID was evaluated.
Results
A total of 383 patients entered the study, 164 of whom were female, and the rest were male. The mean age of the patients was 25.3 ± 14.5 years. The most frequent first presentations of CVID were pneumonia (36.8%) and diarrhea (19.1%). Patient sex, age of onset, and family history did not make significant differences in first presentations of this disease.
Conclusion
pneumonia is the most common first presentation of CVID. Family history of CVID, the age of symptom onset, and sex made no differences in the first presentations of CVID.
Highlights
Pneumonia is the most common first presentation of CVID.
Female patients developed CVID at a younger age than male patients.
Sex is not a differentiating factor in first presentations of CVID.
Family history does not change the first presentations of CVID.
Adulthood-onset and childhood-onset CVID were not different regarding the first presentations.
Similar content being viewed by others

Introduction
Common Variable Immune Deficiency (CVID) is a spectrum of signs and symptoms indicating Primary Immune Deficiency (PID). CVID patients mostly experience defective antibody production, antibody class switch recombination, or antibody affinity maturation [1]. Patients afflicted with this condition may suffer from a wide range of symptoms that will end in about half of them being deceased in a 12.5-year period [2]. The highest proportion of patients with PID (40.2%) in the United States are diagnosed with CVID [3]. In Western Europe, CVID has caused 10,510 years of life lost due to death and disability for each 100,000 of the general population [4].
The presentations of CVID can be divided into two major classes: infectious and non-infectious. Recurrent infections in CVID vary from pneumonia to upper respiratory tract infections and gastrointestinal involvement as well as osteomyelitis and septic arthritis with bacterial pathogens being the leading etiologies of the infectious complications [5, 6]. Non-infectious manifestations of CVID can be in form of autoimmunities such as autoimmune hemolytic anemia, autoimmune thrombocytopenia, autoimmune thyroiditis, and inflammatory bowel disease [7]. Granulomatous disease and malignancies are also seen with a higher prevalence in CVID patients compared to the general population [8].
No previous study has assessed the first presentations of this disease and the role of first symptoms in the evaluation of the prognosis; consequently, in this study, we aimed to collect the first presentations of CVID in a large cohort of the Iranian National Registry of Primary Immune Deficiencies.
Methods and materials
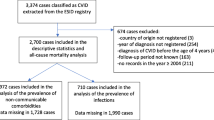
This retrospective study is a part of a large cohort study on Iranian immunodeficiency patients’ national registry from early 2010 to late 2021 [9]. All the patients with a confirmed diagnosis of CVID were included in this study. For any patient labeled as a case of CVID, the following data were collected: date of birth, age, sex, age of onset (month), age of diagnosis (month), having a positive family history of immunodeficiency, delayed diagnosis, and the first presentation. CVID diagnosis was made by the use of European Society of Immunodeficiency criteria as follows: significantly low levels of IgG as well as either IgM or IgA or both with no isohemagglutinins and/or poor response to inoculated vaccines in patients older than two years and in whom other causes of hypogammaglobulinemia have been ruled out [10].
The data were entered into IBM SPSS version 26.0. In this descriptive study, values are presented as numbers (percentage) for qualitative variables and as mean ± standard deviation (SD) for quantitative variables. Comparison of the clinical data and presentations were made using an independent two-sample T-test for quantitative variables and a chi-square test for qualitative variables. P-values less than 0.05 were considered statistically significant.
This study was approved by the Shiraz University of Medical Sciences Committee for Ethics in Biomedical Research by the code IR.SUMS.MED.REC.1400.24398 and written consent forms were obtained from the patients or their legal guardians prior to the interview.
Results
In our study, 383 patients with CVID were surveyed. The patients aged 1–69 years with a mean age of 25.3 ± 14.5 years. Among the studied patients, 164 (42.8%) were female and 219 (57.2%) were male. The median age at onset was 2.0 years (IQR 0.5–8.7) and a mean of 6.9 ± 10.8 years. The median age at diagnosis was 10.0 years (IQR 3.1–21.0) with a mean of 14.4 ± 13.9 years. The median time of delay in diagnosis was 4.0 years (IQR 1.0-9.6) and a mean of 7.6 ± 9.7 years. The mean follow-up period was 9.7 ± 8.6 years in our study. Forty-seven patients (12.3%) had a positive family history of CVID and 193 patients (50.4%) had parental consanguinity.
To evaluate the patients for their diagnosis of CVID immunologic tests were checked the results of which are summarized in Table 1. In our study, the patients had a total White Blood Cell (WBC) count of 10310.2 ± 14210.00 /mm3. The mean IgG level was measured to be 308.6 ± 339.38 mg/dL which is diminished for the adult population. The mean IgM and IgA levels were 44.2 ± 65.24 and 30.8 ± 55.03 mg/dL.
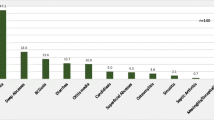
In our study, 356 patients reported their first presentations. The list of first reported presentations of CVID is summarized in Table 2. In total, 484 presentations were reported as the first presentations by our patients. Pneumonia was the most frequent first reported presentation of CVID (36.3%). Diarrhea (18.8%), otitis (14.4%), sinusitis (12.1%), other upper respiratory tract infections (7.2%), skin lesions (5.4%) and fever (3.6) were the other frequent first reported presentations of CVID by the patients.
Male and female patients were compared regarding their first presentation of CVID, the results of which are summarized in Table 3. The mean age at onset was significantly higher in male patients compared to females (8.4 versus 5.9 years respectively, P-value = 0.045). the mean of age, age at diagnosis, and time of delay in diagnosis were similar in both male and female patients (P-values > 0.05). Also, the family history of CVID in male and female patients was similar (P-value = 0.290).
Figure 1 shows the differences in the frequency of the first reported presentations in studied male and female CVID patients. Pneumonia was the most common first reported presentation in both male and female patients. In the female patients, diarrhea and otitis were the other common first reported presentations respectively, whereas, in the male patients, sinusitis and diarrhea were in the second and third rank, respectively. Differences between male and female patients were not statistically significant (P-values > 0.05).

Differences in the frequency of the first reported presentations in 256 studied male and female patients with Common variable immunodeficiency. Differences between male and female patients were not statistically significant (P-values > 0.05)
The patients were also compared regarding their initial symptoms based on the age at which the first symptoms developed. The information regarding the age at the time of symptom onset was available for 337 patients, of who 294 (87.2%) experienced childhood-onset CVID and 43 patients (11.1%) experienced adulthood-onset CVID. The patients were divided into two groups: adulthood-onset (first symptoms after 18 years old) and childhood-onset (first symptoms presented before 18 years old). The symptoms were found to have no association with the age of onset. Table 4 summarizes the findings of this analysis.
Finally, the patients were compared regarding their first presentations based on the family history of CVID. The information regarding the family history of CVID was available for 249 patients, 202(81.12%) of who had a negative family history of CVID and 47 (18.88%) who had a positive family history of CVID. No association was found between family history of CVID and the first presentations of CVID. Table 5 summarizes the findings of the comparison.
In this study, 58 patients underwent endoscopy/colonoscopy during the course of their disease. The most frequent finding was lymphocytic nodular hyperplasia and/or aggregations of lymphocytes (37.9%) in the gastrointestinal tract wall, followed by villous atrophy (26.2%). Moreover, fifty-eight patients had a lung computed tomography (CT) scan in whom the most frequently found abnormality was bronchiectasis (53.4%) followed by peribronchial thickening (29.3%). Pulmonary function test was performed for 59 patients which were normal in 47.5% of the cases. Furthermore, 20.3% of the cases had an obstructive pattern in their pulmonary function test. The findings of these investigations are summarized in Table 6.
In this study, 199 patients had whole exome sequencing, 20.2% of whom had no definitive mutations for CVID. The most frequently seen pathogenic mutation was in LRBA (16.8%), followed by DNMT3B (8.4%). Two of the patients had double mutations. Table 7 summarizes the mutations in this cohort of patients.
Discussion
In this article, we evaluated the first presentations of CVID in all of the newly diagnosed patients in Iran in a ten-year period. We found that respiratory infections, diarrhea, and otitis were the most common first presentations of CVID in our studied population.
In our study, we found that female patients were diagnosed earlier than male patients; however, this difference was not statistically significant. This finding might root in the difference in health-seeking behaviors of male and female patients. In a study by Khajeh et al., they found that male patients were more likely to practice self-medication instead of referring to their doctor. They were also more inattentive to their healthcare needs [11].
According to Ochs, CVID signs and symptoms can be categorized into three groups; first, symptoms associated with infections and immune deficiency, second, symptoms correlated to autoimmunity and granuloma formation, and third, manifestations of the frequent malignancies that patients with CVID are predisposed to such as lymphoma and leukemia [12]. In our article, all of the proposed manifestations were taken into consideration when the patients were approached.
In a systematic review conducted by Zainaldain et al., they found that pneumonia was the most frequently seen infection in patients with CVID with an overall prevalence of over two-thirds. Upper respiratory tract infections and gastrointestinal tract involvement with infectious pathogens were the next common infective complications of CVID [5]. In our article, pneumonia was the most common first presentation of CVID involving about 36.3% of the patients, followed by diarrhea (18.8%), otitis (14.4%), and sinusitis (12.1%). The findings of our study are in line with previous studies regarding the order of frequent first presentations. However, the prevalence of such findings is vastly different which might root in the different methodologies used in various studies. Moreover, in our study, the studied population is rather generalizable since it is conducted on a large population of a national registry.
In a study by Janssen et al., they systematically reviewed the pooled prevalence of various CVID presentations. They found that pneumonia was present in about 75% of the patients, while we found that pneumonia was responsible for about one-third of the first presentations [6]. This difference might indicate that CVID can predispose patients to the development of pneumonia in later stages. Such mechanisms might be through the immune deficiency, and other lung involvements such as chronic pulmonary disease, bronchiectasis, and interstitial lung disease among others. They also found that the “infection-only” type of CVID was less prevalent in adults and the adults showed more interstitial lung disease and structural abnormalities compared to children which are in line with the explanation.
In a study by Baloh et al., the authors assessed patients with CVID over 30 years. They found that children were less likely to develop malignancies and more likely to develop autoimmune hematologic diseases. However, in our study, no association was found between the age of symptom onset and any symptoms. This difference might root in the fact that longer follow-up in the study of Baloh made it possible to detect the long-term consequences of CVID, however, in our study such long follow-up was not possible [13].
In a study by Westh et al. on the Danish population, they found that the median age at onset was 29 years, however, the mean age at onset was 8.4 years for males and 5.9 years for females in our study [14]. This difference might root in the variety of healthcare systems in the two countries of Denmark and Iran. in Iran, strict guidelines are less abided by and the coverage of insurance companies is not dependent on the physician’s function, therefore, more expensive tests are performed sooner compared to developed countries such as Denmark. This fact might eliminate the recall bias in the interview with the patients. In the study performed in Denmark men were diagnosed earlier in contrast to our study. Consequently, the age at diagnosis was lower in Iran and the delay in diagnosis was shorter in Iran compared to Denmark. Another explanation of these differences might be the multifactorial nature of CVID in which genetics and environment both play important roles in the pathogenesis of the disease.
In a study by Gathmann et al., they assessed CVID patients in European countries and found that male patients had a younger age of onset which was not the case in our study [15]. They postulated that the earlier onset of the symptoms in male patients might be due to an undiagnosed X-linked primary immunodeficiency. However, in our study, such immunodeficiency syndromes were ruled out.
In a study by Hosseini-Chavoshi et al. they found that more than one-third of marriages in Iran were consanguineous, while in our study about half of the patients had consanguineous parents which shows the importance of inheritability in this disease [16].
We also found that no association was found between the family history of CVID and the first presentations of CVID. However, no previous study was found in this regard.
Conclusion
In conclusion, we found that pneumonia, diarrhea, otitis, and sinusitis were the most frequent first presentations of CVID. Female patients showed the symptoms earlier than the male patients and there was no statistically significant difference between male and female patients regarding the first presentation of CVID. Family history of CVID and age of onset made no difference in the first presentations of CVID.
Data availability
The data belongs to the Iranian national registry of primary immunodeficiency and the data used for this study can be available from corresponding author upon reasonable request.
Abbreviations
- CVID:
-
Common Variable Immunodeficiency
- PID:
-
Primary Immunodeficiency
- IBD:
-
Inflammatory Bowel Disease
- WBC:
-
White Blood Cell
- SD:
-
Standard Deviation
- CT:
-
Computed Tomography
References
Szczawinska-Poplonyk A, Schwartzmann E, Bukowska-Olech E, Biernat M, Gattner S, Korobacz T, Nowicki F, Wiczuk-Wiczewska M. The pediatric common variable immunodeficiency - from genetics to therapy: a review. Eur J Pediatr. 2022 Apr;181(4):1371–83. https://doi.org/10.1007/s00431-021-04287-6. Epub 2021 Dec 23. PMID: 34939152; PMCID: PMC8964589.
Bagheri Y, Vosughi A, Azizi G, Yazdani R, Kiaee F, Hafezi N, Alimorad S, Khoshmirsafa M, Seif F, Hassanpour G, Abolhassani H, Aghamohammadi A. Comparison of clinical and immunological features and mortality in common variable immunodeficiency and agammaglobulinemia patients. Immunol Lett. 2019 Jun;210:55–62. doi: 10.1016/j.imlet.2019.05.001. Epub 2019 May 3. PMID: 31059734.
Modell V, Orange JS, Quinn J, Modell F. Global report on primary immunodeficiencies: 2018 update from the Jeffrey Modell Centers Network on disease classification, regional trends, treatment modalities, and physician reported outcomes. Immunol Res. 2018 Jun;66(3):367–380. doi: https://doi.org/10.1007/s12026-018-8996-5. PMID: 29744770.
Odnoletkova I, Kindle G, Quinti I, Grimbacher B, Knerr V, Gathmann B, Ehl S, Mahlaoui N, Van Wilder P, Bogaerts K, de Vries E. ; Plasma Protein Therapeutics Association (PPTA) Taskforce. The burden of common variable immunodeficiency disorders: a retrospective analysis of the European Society for Immunodeficiency (ESID) registry data. Orphanet J Rare Dis. 2018 Nov 12;13(1):201. doi: https://doi.org/10.1186/s13023-018-0941-0. PMID: 30419968; PMCID: PMC6233554.
Zainaldain H, Rizvi FS, Rafiemanesh H, Alizadeh M, Jamee M, Mohammadi S, Kiaee F, Mohammadi H, Babaie F, Yazdani R, Abolhassani H, Aghamohammadi A, Azizi G. Infectious complications reporting in common variable immunodeficiency: a systematic review and Meta-analysis. Oman Med J 2020 Jul 30;35(4):e157. doi: https://doi.org/10.5001/omj.2020.64. PMID: 32802416; PMCID: PMC7417520.
Janssen LMA, van der Flier M, de Vries E. Lessons Learned From the Clinical Presentation of Common Variable Immunodeficiency Disorders: A Systematic Review and Meta-Analysis. Front Immunol. 2021 Mar 23;12:620709. doi: https://doi.org/10.3389/fimmu.2021.620709. PMID: 33833753; PMCID: PMC8021796.
Feuille EJ, Anooshiravani N, Sullivan KE, Fuleihan RL, Cunningham-Rundles C. Autoimmune Cytopenias and Associated Conditions in CVID: a Report from the USIDNET Registry. J Clin Immunol. 2018 Jan;38(1):28–34. https://doi.org/10.1007/s10875-017-0456-9. Epub 2017 Oct 28. PMID: 29080979; PMCID: PMC5743637.
Seidel MG, Kindle G, Gathmann B, Quinti I, Buckland M, van Montfrans J, Scheible R, Rusch S, Gasteiger LM, Grimbacher B, Mahlaoui N, Ehl S, ESID Registry Working Party and collaborators. The european Society for Immunodeficiencies (ESID) Registry Working Definitions for the clinical diagnosis of inborn errors of immunity. J Allergy Clin Immunol Pract. 2019 Jul-Aug;7(6):1763–70. Epub 2019 Feb 15. PMID: 30776527.
Abolhassani H, Kiaee F, Tavakol M, Chavoshzadeh Z, Mahdaviani SA, Momen T, Yazdani R, Azizi G, Habibi S, Gharagozlou M, Movahedi M, Hamidieh AA, Behniafard N, Nabavi M, Bemanian MH, Arshi S, Molatefi R, Sherkat R, Shirkani A, Amin R, Aleyasin S, Faridhosseini R, Jabbari-Azad F, Mohammadzadeh I, Ghaffari J, Shafiei A, Kalantari A, Mansouri M, Mesdaghi M, Babaie D, Ahanchian H, Khoshkhui M, Soheili H, Eslamian MH, Cheraghi T, Dabbaghzadeh A, Tavassoli M, Kalmarzi RN, Mortazavi SH, Kashef S, Esmaeilzadeh H, Tafaroji J, Khalili A, Zandieh F, Sadeghi-Shabestari M, Darougar S, Behmanesh F, Akbari H, Zandkarimi M, Abolnezhadian F, Fayezi A, Moghtaderi M, Ahmadiafshar A, Shakerian B, Sajedi V, Taghvaei B, Safari M, Heidarzadeh M, Ghalebaghi B, Fathi SM, Darabi B, Bazregari S, Bazargan N, Fallahpour M, Khayatzadeh A, Javahertrash N, Bashardoust B, Zamani M, Mohsenzadeh A, Ebrahimi S, Sharafian S, Vosughimotlagh A, Tafakoridelbari M, Rahimi M, Ashournia P, Razaghian A, Rezaei A, Mamishi S, Parvaneh N, Rezaei N, Hammarström L, Aghamohammadi A. Fourth update on the Iranian National Registry of primary immunodeficiencies: integration of molecular diagnosis. J Clin Immunol. 2018 Oct;38(7):816–32. https://doi.org/10.1007/s10875-018-0556-1. Epub 2018 Oct 9. PMID: 30302726.
Conley ME, Notarangelo LD, Etzioni A. Diagnostic criteria for primary immunodeficiencies. Representing PAGID (Pan-American Group for Immunodeficiency) and ESID (European Society for Immunodeficiencies). Clin Immunol. 1999 Dec;93(3):190-7. doi: https://doi.org/10.1006/clim.1999.4799. PMID: 10600329.
Khajeh A, Vardanjani HM, Salehi A, Rahmani N, Delavari S. Healthcare-seeking behavior and its relating factors in South of Iran. J Educ Health Promot 2019 Sep 30;8:183. doi: https://doi.org/10.4103/jehp.jehp_93_19. PMID: 31867368; PMCID: PMC6796318.
Ochs HD. Common variable immunodeficiency (CVID): new genetic insight and unanswered questions. Clin Exp Immunol. 2014;Suppl 15–6. https://doi.org/10.1111/cei.12491. PMID: 25546742; PMCID: PMC4285471. Dec;178 Suppl 1.
Baloh C, Reddy A, Henson M, Prince K, Buckley R, Lugar P. 30-Year Review of Pediatric- and adult-onset CVID: clinical Correlates and Prognostic indicators. J Clin Immunol. 2019 Oct;39(7):678–87. https://doi.org/10.1007/s10875-019-00674-9. Epub 2019 Aug 3. PMID: 31377970; PMCID: PMC6754754.
Westh L, Mogensen TH, Dalgaard LS, Bernth Jensen JM, Katzenstein T, Hansen AE, Larsen OD, Terpling S, Nielsen TL, Larsen CS. Identification and Characterization of a Nationwide Danish Adult Common Variable Immunodeficiency Cohort. Scand J Immunol. 2017 Jun;85(6):450–461. doi: https://doi.org/10.1111/sji.12551. PMID: 28370285.
Gathmann B, Mahlaoui N, CEREDIH, Gérard L, Oksenhendler E, Warnatz K, Schulze I, Kindle G, Kuijpers TW, Dutch WID, van Beem RT, Guzman D, Workman S, Soler-Palacín P, De Gracia J, Witte T, Schmidt RE, Litzman J, Hlavackova E, Thon V, Borte M, Borte S, Kumararatne D, Feighery C, Longhurst H, Helbert M, Szaflarska A, Sediva A, Belohradsky BH, Jones A, Baumann U, Meyts I, Kutukculer N, Wågström P, Galal NM, Roesler J, Farmaki E, Zinovieva N, Ciznar P, Papadopoulou-Alataki E, Bienemann K, Velbri S, Panahloo Z, Grimbacher B, European Society for Immunodeficiencies Registry Working Party. Clinical picture and treatment of 2212 patients with common variable immunodeficiency. J Allergy Clin Immunol. 2014 Jul;134(1):116–26. https://doi.org/10.1016/j.jaci.2013.12.1077. Epub 2014 Feb 28. PMID: 24582312.
Hosseini-Chavoshi M, Abbasi-Shavazi MJ, Bittles AH. Consanguineous marriage, reproductive behaviour and postnatal mortality in contemporary Iran. Hum Hered. 2014;77(1–4):16–25. https://doi.org/10.1159/000358403. Epub 2014 Jul 29. PMID: 25060266.
Acknowledgements
The authors would like to thank the participants for their valuable time and effort. Moreover, the authors would like to thank the Deputy of Research and Technology of Shiraz University of Medical Sciences.
Funding
The authors received no funding for this research.
Author information
Authors and Affiliations
Contributions
H.E, S.D, R.Y, and H.A were responsible for designing the study. A.J and A.H.H gathered the data, and N.M with the help of A.A and A.H.H analyzed the data. the draft was written by A.J. and A.H.H all of the authors then read and revised the manuscript. the final version of the manuscript has been accepted by all of the authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All experimental protocols were approved by Committee for Ethics in Biomedical Research of Shiraz University of Medical Sciences by the code IR.SUMS.MED.REC.1400.24398. All methods were carried out in accordance with relevant guidelines and regulations. Moreover, written informed consent forms were obtained from the participants and/ or their legal guardians prior to their interview.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Esmaeilzadeh, H., Jokar-Derisi, A., Hassani, A.H. et al. Assessment of the first presentations of common variable immunodeficiency in a large cohort of patients. BMC Immunol 24, 9 (2023). https://doi.org/10.1186/s12865-023-00545-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12865-023-00545-4