
Abstract
Background
The paper presents an overview of air quality in the 27 member countries of the European Union (EU) and the United Kingdom (previous EU-28), from 2000 to 2017. We reviewed the progress made towards meeting the air quality standards established by the EU Ambient Air Quality Directives (European Council Directive 2008/50/EC) and the World Health Organization (WHO) Air Quality Guidelines by estimating the trends (Mann-Kendal test) in national emissions of main air pollutants, urban population exposure to air pollution, and in mortality related to exposure to ambient fine particles (PM2.5) and tropospheric ozone (O3).
Results
Despite significant reductions of emissions (e.g., sulfur oxides: ~ 80%, nitrogen oxides: ~ 46%, non-methane volatile organic compounds: ~ 44%, particulate matters with a diameter lower than 2.5 µm and 10 µm: ~ 30%), the EU-28 urban population was exposed to PM2.5 and O3 levels widely exceeding the WHO limit values for the protection of human health. Between 2000 and 2017, the annual PM2.5-related number of deaths decreased (- 4.85 per 106 inhabitants) in line with a reduction of PM2.5 levels observed at urban air quality monitoring stations. The rising O3 levels became a major public health issue in the EU-28 cities where the annual O3-related number of premature deaths increased (+ 0.55 deaths per 106 inhabitants).
Conclusions
To achieve the objectives of the Ambient Air Quality Directives and mitigate air pollution impacts, actions need to be urgently taken at all governance levels. In this context, greening and re‐naturing cities and the implementation of fresh air corridors can help meet air quality standards, but also answer to social needs, as recently highlighted by the COVID-19 lockdowns.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
Outdoor air pollution is a major global public health issue [48], leading to 4.2 million premature deaths worldwide [74] and half a million in the European Union (EU) in 2016 [24]. The EU identifies seven main air pollutants [45]: ammonia (NH3), nitrogen oxides (NOx), carbon monoxide (CO), particulate matter with an aerodynamic diameter lower than 2.5 µm and 10 µm (PM2.5 and PM10), sulfur oxides (SOx), tropospheric ozone (O3), and non‐methane volatile organic compounds (NMVOCs). In cities, where 74% of the EU population lives [33], PM2.5 and ground-level O3 have potentially the most significant effects on human health associated with respiratory and cardiovascular diseases and mortality, compared to other air pollutants [9, 55, 75]. In 2016, 374,000 and 14,600 non-accidental premature deaths were attributed to air pollution (PM2.5 and O3, respectively) in the EU-28Footnote 1 countries [24]. Air pollution also damages plant ecosystems [35, 49, 63], and surface O3 is considered as the most detrimental air pollutant in terms of effects on vegetation and biodiversity [1, 52, 63].
The legislated ambient air quality standards and the emission control policies (e.g., [10, 18, 77]) control emissions of harmful substances into the atmosphere, and regulate the concentrations of air pollutants such as PM2.5, PM10, NO2 and O3, by setting limit and target values for the protection of human health Table 1 and requirements to ensure that Member States adequately monitor air quality in a harmonised manner. Therefore, the number of air quality monitoring stations grew rapidly in Europe, by an order of magnitude in 1996, with databases gathering air quality data such as the AirBase system of the European Environment Agency. The number of urban and suburban monitoring stations in Europe ranged from 1300 in 1990 to 3600 in 2000 and about 5000 stations in 2020. Due to the spatial representativeness of monitoring stations and the duration of time series, the above database offers an unprecedented way for trends analysis, and peer-reviewed articles. The Clean Air Programme for Europe (CAPE), published by the European Commission in 2013, aims to improve air quality in Europe by 2030 and to reduce the number of premature deaths by half compared with 2005 [16].
For the first time, through an extensive literature review and trends analysis, this study aims to (i) quantify the annual trends in national emissions of main air pollutants in the EU-28 countries over the time period 2000–2017, (ii) analyze the trends in real-world air pollutants concentrations over the last two decades; (iii) assess the effectiveness of emissions control policies for reducing the exposure of EU-28 population to ambient air pollution, and (iv) evaluate the impact of control policies on the number of premature deaths attributed to exposure to ambient PM2.5 and O3 levels over time.
Materials and methods
Data collection
The official national emissions of main air pollutants (SOx, NH3, PM2.5, PM10) and main O3 precursors (NOx, NMVOCs, CO), submitted by the Parties to the LRTAP Convention, were obtained through the Centre on Emission Inventories and Projections (CEIP) under the European Monitoring and Evaluation (EMEP) Program.Footnote 2 The EU-28 urban population exposure was estimated by the European Environmental Agency (EEA) from data reported in Airbase, and the number of premature deaths attributed to exposure to ambient PM2.5 and O3 (per 106 inhabitants) were obtained by the Organization for Economic Co-operation and DevelopmentFootnote 3 (OECD). The above datasets were obtained over the time period 2000–2017.
Estimation of urban population exposure
For each city included in the Urban Audit,Footnote 4 the EU-28 urban population exposure to air pollutants above the EU limit values and WHO AQG was estimated by combining the concentration maps, from measured concentrations at urban and suburban background monitoring stations with more than 75% of validated hourly data per year, with the population density, and considering that the entire population is potentially exposed to the averaged concentrations, i.e., excluding human mobility [22,23,24,25,26,27,28,29,30,31,32]. The estimation of population exposure was based on data from about 1300 stations in 2000 to 3100 stations in 2017 in EU-28 countries.
Estimation of the national number of premature deaths
The number of non-accidental premature deaths attributable to ambient PM2.5 and O3 were estimated for each EU member country and year by the method described in detail in Global Burden of Diseases [36] and widely used for the health risk assessment of air pollution [2, 3, 12, 37, 42,43,44, 61].
WHO set daily maximum 8-h concentrations for O3 and 24-h average concentration for PM2.5 as metrics to represent the mean daily exposure of population [76]. The daily population exposure to O3 and PM2.5 is estimated by combining concentrations maps from satellite and modeled data, and calibrated by ground measurements, with epidemiological data including relative risk values and baseline incidence rates [36]. For a health endpoint, the number of cases NCc attributed to the exposure to the air pollutant c is calculated as NCc \(=\) BI \(\times\) AP where BI is the baseline incidence rates and AP the attributable proportion, i.e., the fraction of a health endpoint that can be related to the exposure to c in a population Pc where RR is the relative risk value, i.e., the probability of developing a disease associated to an increase of 10 μg m−3 of the air pollutant c concentration [73].
The demographic data were taken from Eurostat [34], and the mortality data and BI were obtained by WHO [72]. The RR values were obtained from exposure–response functions, based on epidemiological studies, following recommendations from the Health Risks of Air Pollution in Europe project, and published by WHO [75]. For the non-accidental mortality (all ages), RR = 1.0123 and RR = 1.0029 are reported for PM2.5 and O3, respectively, i.e., for instance, a 10 μg m−3 increase in the 24-h average PM2.5 concentration is associated with a 1.2% increase in the risk for mortality attributed to non-accidental causes. However, the use of RR values and BI data from local (or national) epidemiological studies is recommended to obtain robust results.
Statistical estimation of annual trends
A 10-year time-series is considered long enough to assess short-term changes [66]. The non-parametric Mann–Kendall test and the non-parametric Sen’s slope estimator were used to detect changes within time-series and estimate the magnitude of trends [38, 65]. Both tests were applied for annual national emissions of main air pollutants and the number of premature deaths attributed to exposure to ambient PM2.5 and O3 levels in EU-28 countries over the time period 2000–2017. In this study, we used MAKESENS program version 1.0 [56]. Results were considered significant at p < 0.05.
Literature review
To report robust short-term air pollutants changes over the last 2 decades, approximately 50 peer-reviewed articles and technical report spanning over the time period 2000–2017 were retrieved from literature databases (Science Direct, Web of Science, and Google scholar). We selected the studies with: (i) in-situ observations from air quality monitoring networks (excluding modeled data); (ii) annual mean concentrations; (iii) at least 10-year time-series of data; (iv) more than 75% of data coverage annually; and (v) significant trend, i.e., with a p value < 0.05.
Results and discussion
Trends in national emissions
Significant reductions were observed for the emission of all primary pollutants, i.e., − 4.7% year−1 for SOx, − 2.7% year−1 for NOx, − 2.6% year−1 for NMVOCs, − 0.6% year−1 for NH3, − 2.9% year−1 for CO and− 1.8% year−1 and− 1.7% year−1 for PM2.5 and PM10, respectively, over the time period 2000–2017 in the EU-28 countries (Fig. 1). The SOx emissions decreased in all EU-28 countries, from − 2.9% year−1 (Germany) to − 6.0% year−1 (Slovenia). For NOx, the highest decrease was observed in the United Kingdom (− 3.4% year−1), while the lowest reduction was found in Lithuania (− 0.6% year−1) and Poland (− 0.7% year−1). For NMVOCs, the decrease ranged from − 0.6% year−1 (Poland) to − 4.0% year−1 (France). In general, small reductions were exhibited in the agricultural sector, contributing to 92% of NH3 emissions [22], but an increase could be determined in Austria, Estonia, Germany, Latvia and Lithuania, ranging from 0.1 to 1.0% per year. The domestic heating represents 48% of CO emissions [22]. Also, the CO emissions usually decreased, except in Malta (+ 0.6% year−1). A decrease of PM2.5 emissions was observed in all EU-28 countries, except Bulgaria (+ 0.5% year−1), Hungary (+ 0.9% year−1) and Romania (+ 0.3% year−1), associating with a slighter reduction in PM10 emissions (− 0.2% year−1 in Bulgaria, − 0.1% year−1 in Hungary). An increase of PM10 emissions was noted in Lithuania (+ 0.8% year−1) and Romania (+ 0.1% year−1). The highest decrease for PM2.5 (− 4.2% year−1) and PM10 (4.0% year−1) emissions occurred in Malta (Fig. 1).

Annual trends of national emissions (% year−1) in the 28 European Union countries (EU-28) for sulfur oxides (SOx), nitrogen oxides (NOx), non-methane volatile organic compounds (NMVOCs), ammonia (NH3), carbon monoxide (CO), particulate matter with an aerodynamic diameter lower than 2.5 µm and 10 µm (PM2.5 and PM10) over the time period 2000–2017 (see Additional file 1: Table S1 for raw data). All trends are significant at p < 0.05 (Mann–Kendall)
The emissions of all primary air pollutants contributing to ambient levels of PM, O3, and NO2 decreased between 2000 and 2017 in the EU-28 (observed reductions SOx: − 80%; NOx: − 46%; NMVOCs: − 44%; NH3: − 10%; CO: − 49%; PM2.5: − 31%; PM10: − 29%), in line with stringent EC Directives, e.g. Air Quality Framework Directive [21], Large Combustion Plant Directive [19], and National Emission Ceilings Directives [17, 20], setting emission reduction commitments by 2030 compared to 2005 (expected reductions SO2: − 79%, NOx: − 63%, NMVOCs: − 40%, NH3: − 19%; PM2.5: − 49%). The emission reductions were mainly achieved as a result of the progress in e.g. the use of flue-gas abatement techniques, energy production and distribution, storage and distribution of solvents [28, 71], and vehicle technologies related to legislative “Euro” standards [59].
In EU-28 countries, the “on-road transport” sector is the largest contributor to total NOx emissions (road transport: 40–55%), and represents 8–15% of VOCs emissions [22]. Diesel-powered motor vehicles account for about 91% of the fleet (from 81% in Czech Republic to 99% in Portugal) in all EU countries except for Greece (37%), and gasoline-powered motor vehicles account for about 7% of the fleet [41]. The Euro-2 to Euro-6 standards for light-duty vehicles were enforced from 1997 to 2015. For diesel cars, the average NOx + VOCs limit ranged from 0.70 g/km (Euro-2) to 0.17 g/km (Euro-6), from 1.00 g/km to 0.50 g/km for CO and from 0.08 g/km to 0.0045 g/km for PM. For gasoline cars, the average NOx + VOCs limit ranged from 0.500 g/km (Euro-2) and 0.128 g/km (Euro-6) and from 2.2 g/km to 1.0 g/km for CO. In 2017, the successive Euro standards have lowered the PM (94%), CO (50%) and NOx + VOCs (76%) emission intensity in the EU compared to early 2000s. An investigation by Breuer et al. [7] in Germany showed that 91% of road transport NOx emissions are produced by diesel-powered motor vehicles. At national level, emissions of NOx from on-road transport decreased in all EU countries (from − 0.81% year−1 in Lithuania to − 4.29% year−1 in Finland) except in Poland (+ 1.51% year−1) and Romania (+ 1.17% year−1) between 2000 and 2017 (Additional file 1: Table S1). Investigations on NOx emissions by diesel cars showed that, on average, their real-world NOx emissions are seven times the limit of 0.08 g/km mandated by the Euro 6 standard [41]. Therefore, the reported reduction of NOx emissions (− 46%) can be overestimated compared to the real-world NOx emissions.
Trends in urban population exposure
Despite the reduction of PM10 emissions over the time period 2000–2017, the minimum and maximum percentage of the EU-28 urban population exposed to PM10 concentrations above the EU daily limit value ranged from 18 to 44% in 2000–2010 to 13–30% in 2010–2017 (Fig. 2), with the highest extent of exposure observed in 2003 (44%). Between 2000 and 2017, the EU daily limit value for PM10 was widely exceeded in Europe, mostly in Eastern Europe [38], e.g., Bulgaria, Cyprus, Czech Republic, Hungary, Poland, Slovakia, Greece, and Italy. In 2017, the EU daily limit value was exceeded in Bulgaria, Croatia, Czech Republic, Poland and Italy [22, 31]. Before 2006, more than 80% of the EU-28 population was exposed to PM10 levels exceeding the WHO AQG, reaching 42–52% in 2014–2017 (Additional file 1: Table S2). From 2000 to 2017, the annual averaged PM10 concentrations decreased by 0.65 μg m−3 year−1 on average at urban stations in the EU-28 [22]. In 2010–2017, 6–14% of the EU-28 population was exposed to PM2.5 levels above the EU annual target value, while the range was 16–52% in 2000–2010 (Fig. 2). The target value was exceeded mostly in Bulgaria, Czech Republic, Poland, and Slovakia between 2000 and 2013. The population exposure to PM2.5 levels above the WHO AQG ranged from more than 90% before 2006 to 74–80% in 2014–2017 Additional file 1: Table S2. Between 2000 and 2017, the annual averaged concentrations of PM2.5 decreased by on average 0.42 μg m−3 per year at urban background stations in the EU-28 [22].

Minimum and maximum percentage of EU-28 population (in %) exposed to air pollutants concentrations (particulate matter PM2.5 and PM10, nitrogen dioxides NO2 and tropospheric ozone O3) exceeding the European Union limit or target values between 2000 and 2017 (see Additional file 1: Table S2; data source: [22,23,24,25,26,27,28,29,30,31,32]
The percentage of the EU-28 population exposed to NO2 concentrations above the EU annual limit value and the WHO AQG decreased from 14 to 31% before 2006, with the maximum recorded in 2003, to less than 10% since 2012 (Fig. 2). The annual limit value was mostly exceeded in Italy, Greece, and in the United Kingdom in 2000–2005, and in Germany in 2010–2016 [22,23,24,25,26,27,28,29,30,31]. The NO2 annual mean concentrations decreased by on average 0.39 μg m−3 year−1 over the time period 2002–2011 by joining 708 urban stations in the EU-28 [38]. The percentage of the EU-28 urban population exposed to SO2 levels above the EU daily limit value ranged from 1 to 2% in 2000–2005 to lower than 0.5% since 2007 (data not shown). The percentage of the EU-28 urban population exposed to SO2 levels exceeding the WHO AQG decreased from more than 70% before 2006 to less than 40% since 2013 [22,23,24,25,26,27,28,29,30,31]. Less than 2% of the EU-28 urban population was exposed to maximum CO daily 8-h mean concentrations above the EU and the WHO AQG (data not shown). Only a few traffic stations in Bulgaria, Poland and Romania have reported exceedances of the SO2 and CO EU limit values over the time period 2000–2017 [22, 38].
The EU-28 urban population exposed to O3 levels above the EU target value for human health protection ranged from 7 to 62% since 2000 (Fig. 2), with the highest extent of exposure observed in 2003. As for NO2 and PM10, the maximum O3 concentrations were observed in 2003, due to extremely warm summer in Europe, with a heatwave occurred in August, and stagnant weather conditions leading to accumulation of air pollutants [70]. The EU target value was mostly exceeded in Southern Europe, where higher background O3 levels (annual mean > 30 ppb) are observed [65], such as Croatia, Cyprus, France, Greece, Italy, Slovenia, Spain, Malta, Portugal, but also in Austria, Hungary, Luxembourg, and Poland recently. More than 95% of the total EU-28 urban population was exposed to O3 levels exceeding the WHO AQG since 2000 (Additional file 1: Table S2). In the EU, the annual mean of daily O3 concentrations increased by on average 0.05 ppb year−1 at 260 urban stations over the time period 2000–2014 Table 2. The annual O3 mean concentrations increased by on average 0.34 ppb year−1 at more than 80% of urban stations between 2005 and 2014, except in the United Kingdom where a decrease (− 0.18 ppb year−1) was observed at 65% of urban stations [59]. In Germany, an increase of 0.18 ppb year−1 was reported at 79 urban stations over the time period 2005–2018 [59]. A significant increase in the annual O3 mean (on average, + 0.29 ppb year−1) was found at urban stations in Southern Europe between 2000 and 2010 [46, 65]. In France, an increase of + 0.14 ppb year−1 at 76% of urban stations was reported between 1999 and 2012 [64]. Despite an increasing fleet size, the reduction in NOx and VOCs emissions since the early 1990s, due to the vehicle emission regulations, allowed a reduction in O3 peaks and high percentiles [11, 26, 62]. At EU-28 urban stations, a reduction in O3 annual mean of the maximum daily 8-h mean values (− 0.75 ppb year−1) was found over the time period 2000–2014 [26]. In Southern Europe, significant reductions in 98th percentile (− 0.51 ppb year−1) and hourly maximum (− 1.81 ppb year−1) values were found at urban stations between 2000 and 2010 [65]. Simpson et al. [68] found an increase of O3 concentrations of 0.1–0.4 ppb year−1 up to the 95th O3 percentile over the time period 1990–2009. The surface O3 levels are rising in cities in Europe from 2000 (e.g., [8, 47, 59, 64, 67, 78], mainly due to a reduced titration of O3 by NO [40, 59].
Trends in national mortality from exposure to ambient PM2.5 and O 3 levels
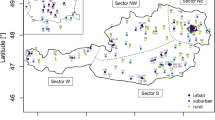
At present compared to other air pollutants, PM2.5 poses the most serious health risk in the EU-28 cities, associated with premature deaths and increased morbidity, followed by ground-level O3 [9, 55]. In the EU-28, the number of deaths due to ambient PM2.5 levels decreased by on average 4.85 per 1,000,000 inhabitants annually between 2000 and 2017 (Fig. 3). The highest annual decreases were observed in the United Kingdom and Estonia (− 11.74 and − 10.46 deaths per 106 inhabitants, respectively) while a slighter reduction was found in Portugal (− 0.50 deaths per 106 inhabitants). In Greece and Lithuania, an increase of annual mortality due to ambient PM2.5 levels was observed (+ 1.22 and + 1.72 deaths per 106 inhabitants, respectively). In line with rising O3 levels in cities [59, 62], the annual O3-related number of premature deaths increased in the EU-28 (on average + 0.55 deaths per 106 inhabitants). The highest annual decrease of mortality was observed in Greece (+ 2.41 deaths per 106 inhabitants), Hungary (+ 2.05 deaths per 106 inhabitants) and Czech Republic (+ 1.40 deaths per 106 inhabitants), while a non-significant increase was found in Spain (+ 0.03 deaths per 106 inhabitants). Between 2000 and 2017, the annual number of deaths attributed to O3 declined mostly in Northern Europe (e.g., Belgium: − 0.24, Ireland: − 0.30, Lithuania: − 0.23 deaths per 106 inhabitants per year) where lower background O3 levels (annual mean < 20 ppb) were observed [4, 59]. In this study, only the outdoor exposure to air pollution was considered while people spend about 80–90% of time in indoor environments [54]. As the spatio-temporal variability of air pollutants levels and human mobility were ignored, the individual exposure estimates are slightly biased.

Annual trends of mortality (number of deaths per 1,000,000 inhabitants per year) due to ambient particulate matter with an aerodynamic diameter lower than 2.5 µm (PM2.5) and tropospheric ozone (O3) over the time period 2000–2017 in the 28 European Union countries (EU-28). Points below the thick line show a decrease in O3- and PM2.5-related mortality, while points above the thick line show an increase (see Additional file 1: Table S3 for raw data)
Conclusions
Between 2000 and 2017, the EU-28 emissions fell for SOx by about 80%, NOx: 46%, NMVOCs: 44%, NH3: 10%, CO: 49%, PM2.5: 31%, and PM10: 29%. This confirms successful control strategies of air pollutants emissions. However, the current levels of air pollutants in cities continue to exceed the EU standards and WHO AQG for the protection of human health in Europe, especially for the secondary air pollutant O3 [12, 23, 38, 61]. In 2015–2017, the percentages of EU-28 urban population exposed to concentrations exceeding the WHO limit values were 74–81% for PM2.5, 42–52% for PM10, 95–98% for O3, 21–31% for SO2 and 7–8% for NO2 [22]. In agreement with a reduction of ambient PM2.5 levels in cities, the annual PM2.5-related number of deaths decreased (− 4.85 per 106 inhabitants) between 2000 and 2017. The control strategies of O3 precursor emissions were effective in rural areas [53, 65]. However, the rising O3 levels have become a major public health issue in the EU-28 cities [47, 59, 62], where the annual O3-related number of premature deaths increased (+ 0.55 deaths per 106 inhabitants) over the time period 2000–2017.
Barmpadimos et al. [5] have reported a positive correlation between PM10 and air temperature in summer (e.g., higher emissions from agriculture), and negative in winter (e.g., lower emissions by tertiary sector for heating). In Europe, the average annual air temperature increased by 0.22–0.40 °C per decade since 1965 [24]. The highest air temperature increase was observed over Eastern and Northern Europe in winter, and over Southern Europe in summer (EEA, 2018b). Climate change is projected to reduce the benefits of PM and O3 precursor emissions controls leading to higher PM and O3 levels.
There is an urgent need to take decisive actions at all governance levels to achieve the objectives of the Ambient Air Quality Directives as reported by the EC COM [15]. These actions span from improving air quality monitoring network, control of emission sources, improved mobility plans and raising awareness to citizens on the problem of air pollution, among others. In this context, urban and peri-urban reforestation and an implementation of fresh air corridors can help improve air quality and meet air quality standards in cities [6, 13, 51], but also answer to social needs, e.g., recreation, cultural, aesthetic [57, 58]. The cold air corridors are needed to reduce the climatic extreme events in large cities, which can lead to air pollution peaks.
Although outside the period of analysis, it is relevant to note that the recent COVID-19 pandemic could represent an opportunity for adopting measures that contribute to improve air quality in European cities in the future. Compared to the same period in 2017–2019, the lockdown measures in 2020 led to a decrease of NO (~ 63%) and NO2 (~ 52%) concentrations in Southern European cities due to the reduction of road and non-road transport [60, 69]. However, these measures did not significantly reduce the PM2.5 and PM10 levels (~ 8%) attributed to an increase of PM emissions from the activities at home (e.g., domestic heating, biomass burning), and during the lockdown, the ground-level O3 levels increased by ~ 17% due to a lower titration of O3 by NO [60]. While it is true that “Air pollution rebounds in Europe’s cities as lockdowns ease” (Financial Times, 24 June 2020) and that COVID discourages the use of public transport, there are some positive changes that, if sustained over time, might result in improvements of air quality in the cities in the future. Partial or total telework has been implemented in many companies and public offices, a change that will last to certain extent after the COVID pandemic reducing private car mobility. Cities like Barcelona and Paris have widened sidewalks to ensure social distancing on pedestrians, created more bicycle lanes and separated traffic and bus lanes for each direction.Footnote 5
The COVID-19 lockdowns showed us the value of green urban spaces for our physical and mental wellbeing. Greening and re‐naturing cities are keywords of the EU Biodiversity Strategy for 2030 EC COM [14]. European Commission calls on European cities of at least 20,000 inhabitants to develop “ambitious Urban Greening Plans” by including the promotion of green infrastructure, nature-based solutions, and by planting at least 3 billion additional trees in the EU by 2030. Then, the COVID pandemic can be taken as an opportunity for the cities to foster changes in organization of the urban public space and re-think mobility [39], which hopefully may have relevant and lasting impacts on the quality of urban air. However, to efficiently reduce air pollution in cities, municipalities and city planners urgently need to base the selection of tree species upon quantitative and concrete assessments of the role of urban trees in affecting air quality either positively or negatively [62]. For improving air quality and thermal comfort in cities, tree planting programs need to: (a) plant and sustain healthy trees by selecting a diversity species well adapted to local conditions, (b) avoid species sensitive to air pollution, (c) use low VOCs and pollen emitting trees, (d) supply ample water to vegetation; (e) use long-lived and low maintenance species; and (f) implement cold air corridor in large cities to minimize the health risk of air pollutants [50, 62].
Availability of data and materials
Not applicable.
Notes
Including the United Kingdom, which withdrew from the European Union on 31st January 2020.
Abbreviations
- AP:
-
Attributable proportion
- AQG:
-
Air Quality Guidelines
- BI:
-
Baseline incidence
- CAPE:
-
The Clean Air Programme for Europe
- CLRTAP:
-
Convention on Long-range Transboundary Air Pollution
- CO:
-
Carbon monoxide
- EEA:
-
European Environmental Agency
- EMEP:
-
European Monitoring and Evaluation Program
- EU:
-
European Union
- GDB:
-
Global Burden of Diseases
- ICCT:
-
International Council on Clean Transportation
- NC c :
-
Number of cases attributed to the exposure to the air pollutant c
- NH3 :
-
Ammonia
- NMVOCs:
-
Non‐methane volatile organic compounds
- NOx :
-
Nitrogen oxides
- O3 :
-
Tropospheric ozone
- OECD:
-
Organization for Economic Co-operation and Development
- PM10 :
-
Particulate matter with an aerodynamic diameter lower than 10 µm
- PM2.5 :
-
Particulate matter with an aerodynamic diameter lower than 2.5 µm
- RR:
-
Relative risk
- SOx :
-
Sulfur oxides
- WHO:
-
World Health Organization
References
Agathokleous E, Feng Z, Oksanen E, Sicard P, Wang Q, Saitanis CJ et al (2020) Ozone affects plant, insect, and soil microbial communities: a threat to terrestrial ecosystems and biodiversity. Sci Adv 6:eabc1176
Amoatey P, Sicard P, De Marco A, Khaniabadi YO (2019a) Human health risk assessment of long-term exposures to PM2.5 in Rome, Italy. ClinEpidemiol Glob Health 7:222–227
Amoatey P, Takdastan A, Sicard P, Hopke PK, Baawain M, Omidvarborna H, De Marco A, Allahyari S, Khanaibadi YO (2019) Short and long-term impacts of ambient ozone on health in Ahvaz, Iran. Hum Ecol Risk Assess 9:1–16
Araminienė V, Sicard P, Anav A, Agathokleous E, Stakėnas V, De Marco A et al (2019) Trends and inter-relationships of ground-level ozone metrics and forest health in Lithuania. Sci Total Environ 658:1265–1277
Barmpadimos I, Hueglin C, Keller J, Henne S, Prévôt ASH (2011) Influence of meteorology on PM10 trends and variability in Switzerland from 1991 to 2008. Atmos Chem Phys 11:1813–1835
Baró F, Chaparro L, Gómez-Baggethun E, Langemeyer J, Nowak DJ, Terradas J (2014) Contribution of ecosystem services to air quality and climate change mitigation policies: the case of urban forests in Barcelona, Spain. Ambio 43:466–479
Breuer JL, Samsun RC, Peters R, Stolten D (2020) The impact of diesel vehicles on NOx and PM10 emissions from road transport in urban morphological zones: A case study in North Rhine-Westphalia, Germany. Sci Total Environ 727:138583
Chang KL, Petropavlovskikh I, Cooper OR, Schultz MG, Wang T (2017) Regional trend analysis of surface ozone observations from monitoring networks in eastern North America, Europe and East Asia. Elementa Sci Anthropocene 5:50
Cohen AJ, Brauer M, Burnett R, Anderson HR, Frostad J, Estep K et al (2017) Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015. Lancet 389:1907–1918
Convention on Long-range Transboundary Air Pollution (2017) Mapping Critical Levels for Vegetation. In: Chapter III of manual on methodologies and criteria for modelling and mapping critical loads and levels and air pollution effects, risks and trends. UNECE.
de Foy B, Brune WH, Schauer JJ (2020) Changes in ozone photochemical regime in Fresno, California from 1994 to 2018 deduced from changes in the weekend effect. Environ Pollut 263:114380
De Marco A, Sicard P, Khaniabadi YO, Hopke PK, Amoatey P (2018) Mortality and morbidity for cardiopulmonary diseases related to PM2.5 exposure in the metropolis of Rome, Italy. Eur J Internal Med 57:49–57
Escobedo FJ, Kroeger T, Wagner JE (2011) Urban forests and pollution mitigation: analyzing ecosystem services and disservices. Environ Pollut 159:2078–2087
European Commission (2020) COM 380 final “EU Biodiversity Strategy for 2030: bringing nature back into our lives.” Brussels 20(5):2020
European Commission (2018) COM(2018) 330 final “A Europe that protects: Clean air for all.” Brussels 17(5):2018
European Commission (2013) COM(2013) 918 final “A Clean Air Programme for Europe.” Brussels 18(12):2013
European Council Directive 2016/2284/EC of the European Parliament and of the Council of 14 December 2016 on the reduction of national emissions of certain atmospheric pollutants, amending Directive 2003/35/EC and repealing Directive 2001/81/EC. Official Journal of the European Union L 344/1 17.12.2016.
European Council Directive 2008/50/EC of the European Parliament and of the Council of 21 May 2008 on ambient air quality and cleaner air for Europe. Off J 152:0044
European Council Directive 2001/80/EC of the European Parliament and of the Council of 23 October 2001 on the limitation of emissions of certain pollutants into the air from large combustion plants. Official Journal L 309, 27.11.2001 P. 0001–0021.
European Council Directive 2001/81/EC of the European Parliament and of the Council of 23 October 2001 on national emission ceilings for certain atmospheric pollutants. Official Journal L 309, 27.11.2001 P. 0022–0030.
European Council Directive 1996/62/EC of the European Parliament and of the Council of 27 September 1996 on ambient air quality assessment and management. Official Journal L 296, 21.11.1996 P. 0055–0063.
European Environment Agency (2019) Air quality in Europe - 2019 report. EEA Technical Report No 10/2019. https://doi.org/10.2800/822355.
European Environment Agency (2018a) Air Quality in Europe-2018 report. EEA Technical Report No 12/2018. https://doi.org/10.2800/777411.
European Environment Agency (2018b) Global and European temperature. https://www.eea.europa.eu/data-and-maps/indicators/global-and-european-temperature-9/assessment. Accessed 10 Dec 2020
European Environment Agency (2017) Air quality in Europe - 2017 report. EEA Technical Report No 13/2017. https://doi.org/10.2800/850018
European Environment Agency (2016) Air quality in Europe - 2016 report. EEA Technical Report No 28/2016. https://doi.org/10.2800/80982
European Environment Agency (2015) Air quality in Europe - 2015 report. EEA Technical Report No 5/2015. https://doi.org/10.2800/62459
European Environment Agency (2014) Air quality in Europe - 2014 report. EEA Technical Report No 5/2014. https://doi.org/10.2800/22775
European Environment Agency (2013) Air quality in Europe - 2013 report. EEA Technical Report No 9/2013. https://doi.org/10.2800/92843
European Environment Agency (2012) Air quality in Europe - 2012 report. EEA Technical Report No 4/2012. https://doi.org/10.2800/55823
European Environment Agency (2011) Air quality in Europe - 2011 report. EEA Technical Report No 12/2011. https://doi.org/10.2800/83213
European Environment Agency (2007) Air quality in Europe - 1990–2004. EEA Technical Report No 2/2007, ISSN 1725–9177.
European Union (2016) Urban Europe Statistics on cities, towns and suburbs. Eurostat Statistical Book. https://doi.org/10.2785/91120
Eurostat: https://ec.europa.eu/eurostat/statistics
Feng Z, De Marco A, Anav A, Gualtieri M, Sicard P, Tian H et al (2019) Economic losses due to ozone impacts on human health, forest productivity and crop yield across China. Environ Int 131:104966
Global Burden of Disease (2018) Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 392:1923–1994
Goudarzi G, Daryanoosh SM, Godini H, Hopke PK, Sicard P, De Marco A et al (2017) Health risk assessment of exposure to the Middle-Eastern Dust storms in the Iranian megacity of Kermanshah. Public Health 148:109–116
Guerreiro CBB, Foltescu V, de Leeuw F (2014) Air quality status and trends in Europe. Atmos Environ 98:376–384
Honey-Rosés J, Anguelovski I, Chireh VK, Daher C, Konijnendijk van den Bosch C, Litt JS et al (2020) The impact of COVID-19 on public space: an early review of the emerging questions - design, perceptions and inequities. Cities Health 1:17
Huszar P, Belda M, Halenka T (2015) On the long-term impact of emissions from central European cities on regional air-quality. Atmos Chem Phys Discussions 15:32101–32155
International Council on Clean Transportation, ICCT (2016) NOx emissions from heavy-duty and light-duty diesel vehicles in the EU: Comparison of real-world performance and current type-approval requirements. ICCT Briefing
Khaniabadi YO, Sicard P, Takdastan A, Hopke PK, Taiwo AM, Khaniabadi FO, De Marco A, Daryanoosh M (2019) Mortality and morbidity due to ambient air pollution in Iran. ClinEpidemiol Glob Health 7:222–227
Khaniabadi YO, Daryanoosh M, Sicard P, Takdastan A, Hopke PK, Esmaeili S, De Marco A, Rashidi R (2018) Chronic obstructive pulmonary diseases related to outdoor PM10, O3, SO2 and NO2 in a heavily-polluted megacity of Iran. Environ Sci Pollut Res 25:17726–17734
Khaniabadi YO, Daryanoosh M, Sicard P, Takdastan A, Hopke PK, Esmaeili S et al (2018) Chronic obstructive pulmonary diseases related to outdoor PM10, O3, SO2 and NO2 in a heavily-polluted megacity of Iran. Environ Sci Pollut Res 25:17726–17734
Koolen CD, Rothenberg G (2019) Air Pollution in Europe. Chemsuschem 10:164–172
Kulkarni PS, Bortoli D, Domingues A, Silva AM (2015) Surface Ozone Variability and Trend over Urban and Suburban Sites in Portugal. Aerosol Air Quality Res 1:15
Lefohn AS, Malley CS, Smith L, Wells B, Hazucha M, Simon H et al (2018) Tropospheric ozone assessment report: global ozone metrics for climate change, human health, and crop/ecosystem research. Elementa Sci Anthropocene 6:28
Lelieveld J, Evans JS, Fnais M, Giannadaki D, Pozzer A (2015) The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature 525:367–371
Mills G, Hayes F, Simpson D, Emberson L, Norris D, Harmens H et al (2011) Evidence of widespread effects of ozone on crops and (semi-)natural vegetation in Europe (1990–2006) in relation to AOT40 and flux-based risk maps. Glob Change Biol 17:592–613
Nowak DJ, Hirabayashi S, Doyle M, McGovern M, Pasher J (2018) Air pollution removal by urban forests in Canada and its effect on air quality and human health. Urban For Urban Greening 29:40–48
Nowak DJ, Crane DE, Stevens JC (2006) Air pollution removal by urban trees and shrubs in the United States. Urban For Urban Greening 4:115–123
Paoletti E (2007) Ozone impacts on forests. CAB Rev 2(68):13
Paoletti E, De Marco A, Beddows DCS, Harrison RM, Manning WJ (2014) Ozone levels in European and USA cities are increasing more than at rural sites, while peak values are decreasing. Environ Pollut 192:295–299
Park YM, Kwan MP (2017) Individual exposure estimates may be erroneous when spatiotemporal variability of air pollution and human mobility are ignored. Health Place 43:85–94
Pascal M, Corso M, Chanel O, Declercq C, Badaloni C, Cesaroni G et al (2013) Assessing the public health impacts of urban air pollution in 25 European cities: results of the Aphekom project. Sci Total Environ 449:390–400
Salmi T, Määttä A, Ruoho-Airola T, Anttila P, Amnell T (2002) Detecting trends of annual values of atmospheric pollutants by the Mann–Kendall test and Sen’s slope estimates. The Excel template application makesens. Publications on air quality 31. Finnish Meteorological Institute, Helsinki
Samson R, Moretti M, Amorim JU, Branquinho C, Fares S, Morelli F et al (2019) Towards an integrative approach to evaluate the environmental ecosystem services provided by urban forests. J For Res 30:1981–1996
Selmi W, Weber C, Rivière E, Blond N, Mehdi L, Nowak DJ (2016) Air pollution removal by trees in public green spaces in Strasbourg city, France. Urban For Urban Greening 17:192–201
Sicard P, Paoletti E, Agathokleous E, Araminienė V, Proietti C, Coulibaly F et al (2020) Ozone weekend effect in cities: Deep insights for urban air pollution control. Environ Res 191:110193
Sicard P, De Marco A, Agathokleous E, Feng Z, Xu X, Paoletti E et al (2020) Amplified ozone pollution in cities during the COVID-19 lockdown. Sci Total Environ 735:139542
Sicard P, Khaniabadi YO, Perez S, Gualtieri M, De Marco A (2019) Effect of O3, PM10 and PM2.5 on cardiovascular and respiratory diseases in cities of France, Iran and Italy. Environ Sci Pollut Res 26:32645–32665
Sicard P, Agathokleous E, Araminiene V, Carrari E, Hoshika Y, De Marco A et al (2018) Should we see urban trees as effective solutions to reduce increasing ozone levels in cities? Environ Pollut 243:163–176
Sicard P, Augustaitis A, Belyazid S, Calfapietra C, De Marco A, Fenn M et al (2016) Global topics and novel approaches in the study of air pollution, climate change and forest ecosystems. Environ Pollut 213:977–987
Sicard P, Serra R, Rossello P (2016) Spatio-temporal trends of surface ozone concentrations and metrics in France. Environ Res 149:122–144
Sicard P, De Marco A, Troussier F, Renou C, Vas N, Paoletti E (2013) Decrease in surface ozone concentrations at Mediterranean remote sites and increase in the cities. Atmos Environ 79:705–715
Sicard P, Coddeville P, Galloo JC (2009) Near-surface ozone levels and trends at rural stations in France over the 1995–2003 period. Environ Monit Assess 156:141–157
Simon H, Reff A, Wells B, Xing J, Frank N (2015) Ozone trends across the United States over a period of decreasing NOx and VOC emissions. Environ Sci Technol 49:186–195
Simpson D, Arneth A, Mills G, Solberg S, Uddling J (2014) Ozone - the persistent menace: interactions with the N cycle and climate change”. CurrOpin Environ Sustain 10:9–19
Tobías A, Carnerero C, Reche C, Massagué J, Via M, Minguillón MC et al (2020) Changes in air quality during the lockdown in Barcelona (Spain) one month into the SARS-CoV-2 epidemic. Sci Total Environ 726:138540
Vautard R, Beekmann M, Desplat J, Hodzic A, Morel S (2007) Air quality in Europe during the summer of 2003 as a prototype of air quality in a warmer climate. CR Geosci 339:747–763
Vestreng V, Ntziachristos L, Semb A, Reis S, Isaksen ISA, Tarrasón L (2008) Evolution of NOx emissions in Europe with focus on road transport control measures. Atmos Chem Phys Discuss 8:10697–10747
World Health Organization (2019) Global Health Estimates: Life expectancy and leading causes of death and disability”. https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates
World Health Organization (2018) AirQ+: software tool for health risk assessment of air pollution”. http://www.euro.who.int/en/health–topics/environment–and–health/air–quality/activities/airq–software–tool–for–health–risk–assessment–of–air–pollution. Accessed 13 Sept 2020
World Health Organization (2016) Global Health Observatory data. https://www.who.int/gho/phe/outdoor_air_pollution/burden/en/. Accessed 13 Sept 2020
World Health Organization (2013) Review of Evidence on Health Aspects of Air Pollution - REVIHAAP Project. World Health Organization, Regional Office for Europe, Copenhagen, Technical Report
World Health Organization (2008) Health risks of ozone from long-range transboundary air pollution. WHO/Euro product ISBN 978 92 890 42895.
World Health Organization (2006) Air quality guidelines global update 2005: particulate matter, ozone, nitrogen dioxide and sulfur dioxide. WHO Regional Office for Europe, Copenhagen
Yan Y, Lin J, Pozzer A, Kong S, Lelieveld J (2019) Trend reversal from high-to-low and from rural-to-urban ozone concentrations over Europe. Atmos Environ 213:25–36
Acknowledgements
This work was made in the framework of the Research Group 8.04.00 “Air Pollution and Climate Change” and Working Party 8.04.05 “Ground-level ozone” under the International Union of Forest Research Organizations.
Funding
This work was carried out with the contribution of the LIFE financial instrument of the European Union in the framework of the AIRFRESH project “Air pollution removal by urban forests for a better human well-being” (LIFE19 ENV/FR/000086). V.C. thanks Project IMAGINA (PROMETEU 2019, Generalitat Valenciana).
Author information
Authors and Affiliations
Contributions
PS, VC, and EA conceived the project. PS, VC, and EA analyzed the data. All authors participated in writing and revising the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Annual trends of national emissions (% year-1) in the 28 European Union countries (EU-28) for sulfur oxides (SOx), nitrogen oxides (NOx), on-road transport NOx (NOx_road), non-methane volatile organic compounds (NMVOCs), ammonia (NH3), carbon monoxide (CO), particulate matter with an aerodynamic diameter lower than 2.5 μm and 10 μm (PM2.5 and PM10) over the time period 2000–2017. All trends are significant at p < 0.05 (Mann-Kendal). The increasing trends are in bold. Table S2. Minimum and maximum percentage of EU-28 population (in %) exposed to air pollutants concentrations (tropospheric ozone O3, nitrogen dioxides NO2, particulate matter PM2.5 and PM10) exceeding the European Union (EU) and World Health Organization Air Quality Guidelines (WHO AQG) limit or target values between 2000 and 2017. Table S3. Annual trends of mortality (number of deaths per 1,000,000 inhabitants per year) due to ambient particulate matter with an aerodynamic diameter lower than 2.5 μm (PM2.5) and tropospheric ozone (O3) over the time period 2000–2017 in the 28 European Union countries (EU-28) with associated significance level p (Mann-Kendal *** p < 0.001; ** p < 0.01; * p < 0.05; + p < 0.1 and p < 0.1).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sicard, P., Agathokleous, E., De Marco, A. et al. Urban population exposure to air pollution in Europe over the last decades. Environ Sci Eur 33, 28 (2021). https://doi.org/10.1186/s12302-020-00450-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12302-020-00450-2