
Abstract
Background
Tamsulosin, an alpha-blocker in medical expulsive therapy, selectively relaxes ureteral smooth muscle, while Tadalafil, a PDE5-Is, is recommended for treating lower urinary tract symptoms.
Methods
This study compares the effectiveness of Tadalafil and Tamsulosin as medical expulsive therapy for distal ureteric stones at the Urology Department, Beni-Suef University Hospital, Egypt, using baseline demographics, preoperative data, intraoperative data, and outcome analysis.
Results
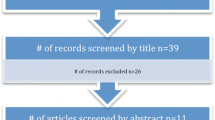
A randomized comparative study that is prospective and was from March 2019 to March 2021. Although 280 instances were eligible, 30 were eliminated & 250 were randomized, and only 164 patients completed the study. 83 patients were in the study Tadalafil group (Group A), 54 males (65.1%) & 29 (34.9%) and 81 patients were assigned to the Tamsulosin group (Group B), 47 males (58%) &34 females made up the Tadalafil group (Group A). The study was completed by 34 females (42%). Additionally, there was a significant difference in the meantime for stone expulsion between groups A (8.8 ± 3.1 days) and B (10.8 ± 3.4 days, (p = 0.001). With fewer episodes of colic, Group A needed less analgesia than Group B.
Conclusions
Tadalafil is a safer and more effective treatment for 5–9 mm lower ureteric end stones, offering a higher stone expulsion rate, earlier passage, lower analgesic requirements, and fewer colic episodes.
Similar content being viewed by others


1 Background
One of the urologic conditions that is most frequently diagnosed, having a high incidence and significant clinical and financial burden on the healthcare system, is nephrolithiasis [1].
The incidence rate of urinary stones is on a constant rise; hence, it is the interest of urologists all over the world. Stones lodged in the ureter, especially the distal ureter, are the most common types of cause of loin pain and urine flow obstruction [2].
Many factors can affect the passage of ureteric stones, such as size, stone location, number, ureteric spasm, peristalsis, ureteric anatomy, mucosal edema or inflammation [3].
Due to the high incidence of spontaneous distal ureteric stone passage, medical expulsive therapy (MET) is the most important noninvasive treatment for small-sized distal ureteric calculi [4] involving various treatments like α-adrenergic blockers, calcium channel blockers, NSAIDs, and corticosteroids. These treatments help increase stone passing rates by blocking receptors [5].
Monotherapy with tadalafil or tamsulosin similarly improved lower urinary tract symptoms had already been demonstrated. Managing LUTS with monotherapy in the form of Tadalafil or Tamsulosin has become an established line of treatment [6].
With the demonstration of in vitro effects of phosphodiesterase‑5 inhibitor (PDE5i) sildenafil, vardenafil, and tadalafil on isolated human ureteral smooth muscle, interest in the use of PDE5i as MET has increased [7].
Hence, drugs classically used to expel stones relied on ureteral smooth muscle relaxation by blocking alpha-1 receptors. One of the often prescribed alpha-1 blockers is Tamsulosin [8].
PDE5 inhibitors, a modern medication, are used to expel lower ureteric stones by stopping the breakdown of cAMP and cGMP, causing smooth muscle relaxation and making stone passage easier. Tadalafil, a selective PDE5is, was approved for erectile dysfunction (ED)-related LUTS [9].
Over the last few years, there has been a growing interest in the employment of PDE5 as MET upon the showing of in-vitro actions of Tadalafil on isolated human ureteral smooth muscle [7, 8, 10].
Several studies have shown an additional benefit when using Tadalafil in combination with Alfa blockers [11,12,13].
Tadalafil, as a sole treatment for distal ureteric stones, offers benefits like safety, effectiveness, and potential improvement in coexisting ED, but it remains controversial and requires more scientific support. [14,15,16]
Therefore, we aimed to add to the body of evidence in support of Tadalafil as an optimal single-drug MET option.
1.1 Objective
To compare the effectiveness of Tadalafil and Tamsulosin as medical expulsive therapy for distal ureteric stones.
2 Methods
Study design A prospective randomized controlled double blinded trial.
Study Setting The study, conducted from March 2019 to March 2021, involved participants from the Urology Department at Beni-Suef University Hospital in Egypt.
2.1 Inclusion criteria
Patients with unilateral single symptomatic lower ureteric stones, patients who was between the ages of 16 and 60 years, and stones measuring 5 to 9 mm in size were included.
2.2 Exclusion criteria
Patients with bilateral or multiple ureteric stones, a ureteric stone in solitary kidney, active urinary tract infection, moderate to marked hydronephrosis as documented by ultrasound, and chronic, or acute renal failure were excluded from the study.
2.3 Intervention
Pre-intervention steps
-
Urological assessment of the patient's urological history, medical, sexual, and drug history was reviewed, along with a clinical examination of the abdomen and prostate.
-
Laboratory assessment: routine lab (urinalysis and culture, blood picture and kidney function tests).
-
Radiological assessment was a Non-contrast computed tomography scan (NCCT), ultrasound (US) imaging of the urinary tract and plain X-ray of the kidneys, ureters and bladder (KUB) radiograph.
2.4 Technique
Patients were divided into 2 groups randomly via a sealed envelope system, achieving nearly equal-sized treatment groups. The study was double-blinded (both researchers and patients didn’t know the active ingredient). The tablets were prepared by specialized pharmacists who knew each type of the tablet. The tablets were similar in shape and color.
Group A Patients who took 5 mg of tadalafil orally every day.
Group B Patients who took 0.4 mg of tamsulosin hydrochloride orally every day.
Each group's patient got the anticipated care, which consists of:
(1) Proper hydration, consuming 3 L or more of water daily; (2) 50 mg of oral diclofenac taken on demand (3) Parenteral ketorolac 30 mg ampoules on demand; (4) 4 mg ampoules of ondansetron hydrochloride, a parenteral antiemetic administered on demand; (5) Limiting salt in the diet.
A ureteroscopy was performed, and treatment terminated when uncontrollable discomfort, fever, a shift in the degree of hydronephrosis from mild to moderate or severe as documented on follow-up by ultrasonography, and the inability to expel the stone after four weeks occurred.
Assessments of the stone expulsion rate, time of expulsion, pain episodes, and total analgesic usage were part of the follow-up.
Follow-up radiologically on the cases: Use ultrasonography to monitor any changes in the degree of hydronephrosis, KUB to check for radiopaque stones, and CT KUB to ensure that the stone has completely cleared.
2.5 Ethical consideration
The Review Board, an ethical committee, granted its approval (approval number: FMBSUREC/30042019/ Saleh). After being fully briefed about the purpose of the study, participants were told about the goal and benefits of the analysis. Participants in the study voluntarily provided their consent. Furthermore, written consent was granted beforehand. For the participants, the confidentiality of the gathered data was guaranteed.
2.6 Study outcomes
In this study, we sought to assess the efficacy of tamsulosin, which is currently controversial in passing stones with tadalafil, among patients with distal ureteral stones since the reported results of the studies cannot definitively answer whether the rate and time of stone expulsion and analgesic requirement time are the same among patients treated with tamsulosin and tadalafil or not.
2.7 Statistical analysis
2.7.1 Statistical method
The study used G power version 3.1 for Microsoft 10 Windows to calculate sample size based on time to expulsion, resulting in 152 patients, with 76 in each arm and 83 to overcome dropout or follow-up.
The study used SPSS version 17 to analyze data, presenting means, standard deviations, ranges, frequencies, and percentages. Statistical significance was determined using unpaired Student t-test and chi-square test (Fig. 1).

Flow diagram of the study:
3 Results
The study included 83 Tadalafil and 81 Tamsulosin patients, with a mean age of 36.3 ± 7.8 years in Group A and 38.6 ± 8.2 years in Group B. The male-to-female ratio was 1.9 in Group A and 1.4 in Group B. Comorbidities were comparable in both groups (Table 1).
As regards the Table 1 there is a positive statistical association between comorbidities in the use of both medications, with no significant statistical difference between 2 groups related to demographic data, age, or sex.
Group A had no significant difference in hospital visits but required less Diclofenac Sodium administration, a higher stone expulsion rate, and a shorter mean time for stone expulsion compared to Group B (Table 2 and Fig. 2).

Survival analysis for comparison between the study groups regarding the time to stone expulsion
The study found no significant difference in drug-related adverse effects between groups, except for headache, and 87% of male patients experienced penile tumescence without priapism in Group A. Ejaculatory dysfunction was significantly higher in Group B (Table 3).
As regards Table 3, Headache is the predominant side effect in group A, then gastritis, but in group B, headache, Postural hypotension & backache are equal in incidence.
The median time to stone expulsion in the tadalafil group was 8 days (95% CI was 7.37–8.63) and 10 days (95% CI was 8.825–11.17) in the tamsulosin group. A statistically significant difference was evident between both groups regarding the time to expulsion and regarding the expulsion rate (85.5% vs. 76.1%, respectively).
4 Discussion
Ureteric stones constitute only one-fifth of urinary tract calculi. They are the most responsible for 25% of symptoms related to urolithiasis. However, the literature has shown distal ureteric calculi to be the most liable to spontaneous passage, reaching 98% for stones under 5 mm and up to 51% for stones ranging from 5 to 10 mm. [14]
Distal ureteric calculi are most likely to spontaneously pass, influenced by factors like burden, density, location, and spasm [15]. Medical therapy has been proven over the years to be a useful adjunct to observation [16]. In Abdel Rahim et al., patients were classified into 3 (Taladafil, Tamsulin and Placebo) groups of participants, while in Hasan et al. [17] patients were divided into Taladafil and Placebo groups. In Kumar et al. [11] patients were divided into Taladafil, Tamsulin and silodosin groups Table 4. In Abdel Rahim et al. [18] there is no statistically significant difference between the three groups.
In our study and Goyal et al. [5] patients were classified into 2 groups (Taladafil, and Tamsulin), in our study, no significant statistical difference between the 2 groups related to demographic data, age, or sex. In our study, Stone size was varied from 5 to 9 mm with mean ± SD stone size in mm in the group of Taladafil (7.4 ± 1.3) and in the group of Tamsulin (7.2 ± 1.3) (P value = 0.261). In our study, Seitz et al. [8] and Hada et al. [19] research: Medical therapy has been proven to be a useful adjunct to observation. Conservative approaches are preferred due to less associated morbidity [15]. Tamsulosin is widely used to relax smooth muscles and facilitate stone passage [8].
PDE5 is, relax smooth muscles and increase ureteric stone passage [5]. Kumar et al. [11] study found that Tadalafil combined with Tamsulosin caused higher stone expulsion rates, lower time to expulsion, and lower analgesic requirement and hospitalization for colic compared to Tamsulosin alone. Rahman et al. [13] found a significant difference in stone expulsion rate between Sildosin plus Tadalafil (90%) and Tamsulosin (57.5%), with a shorter mean time to stone expulsion and fewer pain episodes. Gnyawali et al. [12] study found that the expulsion rate of Tamsulosin was 50% compared to 64% when combined with Tadalafil. A study on single-drug MET revealed that Tadalafil and Tamsulosin had lower stone expulsion rates (66.7%) and time to stone expulsion (83.3%) compared to Sildosin [16]. A study by Bahadur et al. [15] found higher expulsion rates for Tadalafil as monotherapy compared to Tamsulosin but lower times for expulsion and similar side effects. Our study found that Tadalafil showed the superior time to expulsion compared to both drugs in resolving stones. In contrast to Goyal's study, Tamsulosin was found to be more effective than Tadalafil in terms of stone expulsion rate and time required, also in both studies, there was significantly higher retrograde ejaculation [14].
MET aids in ureteric stone passage, reduces stone expulsion time, reduces renal colic risk, and reduces analgesic use. Our finding is similar to Bahadur et al.'s study [15]. In our study Kumar's trial found no significant drug-related side effects, except headache and tumescence in the Tadalafil group, but all side effects were well tolerated and comparable between research groups [11].
The study, despite its limited number of patients and lack of a placebo group, is one of the few investigating Tadalafil as a sole treatment for managing lower ureteric stones.
5 Conclusions
Tadalafil, a safe, effective medication, has a higher stone expulsion rate than Tamsulosin for distal ureteric calculi, reducing analgesic requirements and colic episodes.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Shokeir AA, Tharwat MA, Abolazm AE, Harraz A (2016) Sildenafil citrate as a medical expulsive therapy for distal ureteric stones: a randomized double-blind placebo-controlled study. Arab J Urol 14:1–6
Tasian GE, Kabarriti AE, Kalmus A, Furth SL (2017) Kidney stone recurrence among children and adolescents. J Urol 197(1):246–252
Wein A, Kavoussi L, Partin A, Peters C (eds) (2016) Campbell-Walsh urology, 11th edn. Elsevier, Philadelphia, pp 3743–3743
Pietropaolo A, Proietti S, Geraghty R, Skolarikos A, Papatsoris A, Liatsikos E, Somani BK (2017) Trends of ‘urolithiasis: interventions, simulation, and laser technology’ over the last 16 years (2000–2015) as published in the literature (PubMed): a systematic review from European section of Uro-technology (ESUT. World J Urol 35:1651–1658
Goyal SK, Singh V, Pandey H, Chhabra MK, Aggarwal SP, Bhat A (2018) Comparative efficacy of tamsulosin versus tadalafil as medical expulsive therapy for distal ureteric stones. Urol Ann 10:82–86
Oelke M, Giuliano F, Mirone V, Xu L, Cox D, Viktrup L (2012) (2012): Monotherapy with tadalafil or tamsulosin similarly improved lower urinary tract symptoms suggestive of benign prostatic hyperplasia in an international, randomized, parallel, placebo-controlled clinical trial. Eur Urol 61(5):917–925
Gratzke C, Ückert S, Kedia G, Reich O, Schlenker B, Seitz M, Becker AJ, Stief CG (2007) In vitro effects of PDE5 inhibitors sildenafil, vardenafil and tadalafil on isolated human ureteral smooth muscle: a basic research approach. Urol Res 35:49–54
Seitz C, Liatsikos E, Porpiglia F, Tiselius HG, Zwergel U (2009) Medical therapy to facilitate the passage of stones: what is the evidence? Eur Urol 56(3):455–471
Shabsigh R, Seftel AD, Rosen RC, Porst H, Ahuja S, Deeley MC, Garcia CS, Giuliano F (2006) Review of time of onset and duration of clinical efficacy of phosphodiesterase type 5 inhibitors in treatment of erectile dysfunction. Urology 68(4):689–696. https://doi.org/10.1016/j.urology.2006.05.009
Al-Aown A, Kyriazis I, Kallidonis P, Sakellaropoulos G, Vrettos T, Perimenis P, Filos K, Liatsikos E (2011) Vardenafil effect on ureteric smooth muscle. In vitro study in porcine model. J Endourol. https://doi.org/10.1089/end.2010.0244
Kumar S, Jayant K, Agrawal S, Singh SK (2014) Comparative efficacy of tamsulosin versus tamsulosin with tadalafil in combination with prednisolone for the medical expulsive therapy of lower ureteric stones: a randomized trial. Korean J Urol 55(3):196–200
Gnyawali D, Pradhan MM, Sigdel PR, Parajuli P, Chudal S, Poudyal S, Chapagain S, Luitel BR, Chalise PR, Sharma U, Gyawali PR (2020) Efficacy of tamsulosin plus tadalafil versus tamsulosin as medical expulsive therapy for lower ureteric stones: a randomized controlled trial. Hindawi Adv Urol. https://doi.org/10.1155/2020/4347598
Rahman MJ, Faridi MS, Mibang N, Singh RS (2018) Comparing tamsulosin, silodosin versus silodosin plus tadalafil as medical expulsive therapy for lower ureteric stones: a randomized trial. Arab J Urol. https://doi.org/10.1016/j.aju.2017.11.012
Goyal SK, Singh V, Pandey H, Chhabra MK, Aggarwal SP, Bhat A (2018) Comparative efficacy of tamsulosin versus tadalafil as medical expulsive therapy for distal ureteric stones. Urol Ann 10:82–86
Kc HB, Shrestha A, Acharya GB, Basnet RB, Shah AK, Shrestha PM (2016) Tamsulosin versus tadalafil as a medical expulsive therapy for distal ureteral stones: a prospective randomized study. Investig Clin Urol 57(5):351–356. https://doi.org/10.4111/icu.2016.57.5.351
Kumar S, Jayant K, Agrawal MM, Singh SK, Agrawal S, Parmar KM (2015) Role of tamsulosin, tadalafil, and silodosin as the medical expulsive therapy in lower ureteric stone: a randomized trial (a pilot study). Urology 85(1):P59-63. https://doi.org/10.1016/j.urology.2014.09.022
Hasan H, Jaffal W, Al-Hossona H (2011) The role of tadalafil in lower ureteric stone expulsion. IRAQI Postgrad Med J 10(1):24–32
Abdel Rahim AM, Abdel-Raheum MA, Sayed M, Hussein AA (2020) Tadalafil versus Tamsulosin as a medical expulsive therapy for solitary unilateral lower ureteric stone less than 1 cm: a prospective randomized study. MJMR 31(3):413–420
Hada A, Yadav SS, Tomar V, Priyadarshi S, Agarwal N, Gulani A (2018) Assessment of factors affecting the spontaneous passage of lower ureteric calculus on the basis of lower ureteric calculus diameter, density, and plasma C- reactive protein level. Urol Ann 10(3):302–307. https://doi.org/10.4103/UA.UA_89_17
Acknowledgements
Not applicable
Funding
None.
Author information
Authors and Affiliations
Contributions
All authors have read and approved the manuscript; AM. Ragheb, conception, work design; AG. Mohamed, interpretation of data; A. Abd Elatif, drafted the manuscript; AS. Mostafa, drafted the manuscript; A A. Elmarakbi, conception, work design; RM. Ibrahim. Revised the work; AM. Elbatanouny, Data analysis.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Review Board, an ethical committee, approval obtained from the hospital ethics committee at the Faculty of Medicine, Beni-Suef University, granted its approval (approval number: FMBSUREC/30042019/Saleh) After being fully briefed about the purpose of the study, participants were told about the goal and benefits of the analysis. Participants in the study voluntarily provided their consent. Furthermore, written consent was granted beforehand. For the participants, the confidentiality of the gathered data was guaranteed. Informed consent was taken from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Ragheb, A.M., Mohamed, A.G., Mostafa, A.S. et al. Tadalafil versus tamsulosin for distal ureteric stone expulsion; a prospective randomized comparative study. Afr J Urol 30, 20 (2024). https://doi.org/10.1186/s12301-024-00425-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12301-024-00425-2