
Abstract
Background
Bilateral ectopic pelvic kidneys are rarely observed, and cake form of fusion is a relatively distinct anomaly. With the presence of aberrant vasculature and risk of injuring surrounding viscera, conventional treatment of symptomatic calculi with percutaneous and retrograde approaches, become challenging for the urologist. 3D Laparoscopic approach is safe, reduces patient morbidity and avoids open surgery.
Case presentation
We herein report a case of 44-year-old female with symptomatic calculi in a pelvic cake kidney, which was adequately managed by 3D laparoscopic transperitoneal pyelolithotomy. Preoperatively, CT imaging and fluoroscopy were performed. The surgery lasted for 156 min, and complete stone clearance was achieved. Postoperative course was uneventful, and patient was discharged in 72 h.
Conclusions
3D Laparoscopic pyelolithotomy is an acceptable and efficient treatment modality for symptomatic calculi in ectopic fused pelvic kidneys with a malrotated orientation.
Similar content being viewed by others


1 Background
Overall incidence of ectopic kidneys approximates 1 in 900 with an incidence of a pelvic location of less than 1 in 200 [1, 2]. There is no significant gender difference, and left side is favored slightly over the right side [3]. Bilateral ectopic kidneys are rarely observed and accounted for only 10% of all patients with renal ectopia [4]. These may be simple ectopia (ectopic on its own side) or crossed ectopia (across the midline fused or unfused to contralateral kidney) with the most common location in pelvis opposite sacrum below the bifurcation of aorta. The cake, or lump, kidney is a relatively rare form of fusion with the total kidney being irregular and lobulated [5]. It may be associated with malformations of other systems including skeletal, genitourinary, cardiovascular and gastrointestinal tract [6]. Most ectopic kidneys are asymptomatic. Absence of kidneys in normal location with the presence of reniform structure in ectopic location, guides the diagnosis of renal ectopia when the imagining usually performed for other causes. Urinary stasis as a result of abnormal location of the renal pelvis, high insertion of ureter or external compression increases the probability of stone formation.
Management of symptomatic calculi in ectopic fused kidneys is a challenging task for the urologist.
Patients harboring this diagnosis may require multiple endourologic procedures for complete stone clearance.
Ureteroscopy and percutaneous nephrolithotomy (PCNL), shock wave lithotripsy (SWL) can be considered as a reasonable management option, however larger stone burdens with complex anatomy may require more invasive methods, which include pyelolithotomy using open, laparoscopic or robotic approaches [7].
For ectopic kidney with a small stone burden, flexible ureteroscopy and shock wave lithotripsy can be used as effective modalities [8]. However, larger stone sizes necessitate much invasive interventions such as open, percutaneous, laparoscopic or robotic approaches. Choosing the right approach depends on the location of kidneys, presence of hydronephrosis, stone burden and stone density.
Percutaneous access through a standard flank approach may not be suitable in pelvic ectopic kidneys and frequently requires modification of the technique including laparoscopic assistance to avoid inadvertent injury to the surrounding viscera [9].
Laparoscopic pyelolithotomy for ectopic renal calculi was described much later than laparoscopic-guided endourologic procedures. The first laparoscopic pyelolithotomy was described by Chang and Dretller in 1996 [10]. The pelvis of ectopic kidneys is often dilated, as many of them have pelviureteric junction obstruction. Laparoscopic pyeloplasty combined with pyelolithotomy has been described by Ramakumar et al. for such patients [11]. However, in our patient, the IVP demonstrated prompt excretion ruling out ureteropelvic junction obstruction.
The precise location and type of fusion anomaly, stone burden, presence of hydronephrosis, variation of pelvicalyceal anatomy, bony structure and surrounding viscera are important factors in deciding the treatment approach.
2 Case report presentation
A-44-year-old female presented with lower quadrant pain for the past 2 years, which was dull aching, mild to moderate in intensity, radiating to the left flank, and was relieved on taking medications. The physical examination was normal with no significant other findings. Upon investigating, operative laboratory investigations were within normal limits. Ultrasonography (USG) showed B/L empty renal fossa with lower poles of both kidney fused at right iliac fossa with 17 mm calculi in mid calyx of left kidney with mild hydronephrosis. Intravenous pyelography (IVP) confirmed the location of stone in ectopic kidney with B/L excretion present in both. The CT urography revealed 23 mm left renal pelvic calculus (800HU) with mild HDN. Both kidney fused with cake kidney configuration in pelvic location. Left kidney having an anteriorly directed intrarenal pelvis with a large stone and normal excretion (Fig. 1a–d).

a–d CT urography showing cake kidney configuration in pelvic location. Left kidney having an anteriorly directed intrarenal pelvis with a large stone and normal excretion
The procedure was performed under general anesthesia. A preliminary cystoscopy was done, orthotopic left ureteric orifice (Fig. 2) identified, retrograde pyelography (Fig. 3) done and an open-ended ureteric catheter was guided into the renal pelvis to later help in identification of the pelvis. The other end of the ureteric catheter was kept in the sterile surgical field for further control and fixed to the self-retaining urethral catheter.

Left ureteric orifice

Retrograde pyelogram showing pelvic calculus
The patient was placed in a 30° Trendelenburg position with a gentle lateral elevation on the left side to ensure that the bowel falls away from the side to be operated.
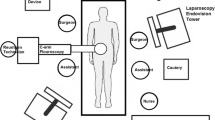
Pneumoperitoneum was initiated using a Veress needle. The procedure was performed with four ports: three 12-mm laparoscopic trocars were placed: one for the camera below the level of the umbilicus in midline, midway between the umbilicus and the symphysis pubis and two near the lateral border of rectus at the level of umbilicus. Another 5-mm trocar was inserted at the anterior axillary line, lateral and proximal to the last one, which helped in bowel retraction (Fig. 4).

Port placement
The bowel loops were slided out of the pelvis, and the colon was reflected medially along the line of Toldt. The ureteric catheter was gently moved from outside by the assistant, and this aided in the identification of the ureter. The ureter was found to have dense periureteric adhesions. Intraoperative fluoroscopy with C-arm was used to identify the location of the stone in pelvis. The perirenal fat was dissected to expose the wall of the renal pelvis, which was then incised using Harmonic Ace (Fig. 5). L-shaped incision was given over the pelvis ensuring adequate space for removal of the 2.5 cm renal calculi (Fig. 6). Dissection of any of the renal vessels was not required. A 5 Fr × 21 cm double ”J” (DJ) stent was placed through one of the 12 mm ports, and the pyelotomy incision was primarily closed with continuous Vicryl 4–0 suture in a tension free, watertight pattern.

Renal pelvis

Stone extraction
A 14F drain was placed in the peritoneal cavity close to the kidney through the left 5-mm laparoscopic port. Hemostasis was confirmed, stone was bagged and removed, the laparoscopic ports were removed and skin closure was done (Fig. 7). The postoperative course was uneventful. Complete clearance was documented with plain x-ray KUB with DJ stent in situ (Fig. 8). Urethral catheter was removed on 3rd postoperative day followed by drain removal. Patient was satisfactorily discharged. The left DJS was removed after 4 weeks under local anesthesia. Patient lives symptom free till date.

Postoperative scar

Comparing preoperative and postoperative x-ray showing stone clearance with DJ stent in situ
3 Results
Complete stone clearance was achieved. Surgery lasted 156 mins. Estimated blood loss was < 50 ml. No notable complications were encountered. The per urethral catheter was removed after 24 h, and intraperitoneal drain was removed after 48 h. The patient was discharged 72 h after surgery. The double J stent was removed 4 weeks after surgery under local anesthesia. Follow-up ultrasonography at 3 months revealed a no hydronephrosis or calculi.
4 Discussion
Abnormally located kidneys with differently rotated pelvis require different approaches for stone extraction.
Factors such stone size, density and location and upper urinary tract abnormalities, influence the choice of therapeutic approach (retrograde, percutaneous and/or laparoscopic/robotic). Laparoscopic pyelolithotomy is a safe and minimally invasive treatment option for large kidney stones with unfavorable anatomy for the endoscopic approach [12].
3D Laparoscopic pyelolithomy can allow direct exposure and make stone extraction possible in one setting. We prefer going in with an intraperitoneal access, as we are more familiar, and can manage a better working space with no significant difference in the postoperative ileus rates. Performing retrograde pyelogram at the start of procedure with placement of an open-access ureteric catheter helps in identification of the ureter and pelvis, saving significant amount of time. Intraoperative fluoroscopic guidance with C-arm for confirming the position of the calculus and marking the pyelotomy incision is advocated.
A steep learning curve, with poor depth perception, and spatial orientation remain the main drawbacks of two-dimensional (2D) laparoscopy. Three-dimensional (3D) laparoscopic systems have been developed with stereoscopic vision, in which depth perception is achieved by combining different unique images received by each eye.
Initially, surgeons were uncomfortable with the 3D system due to heavy active shutter glasses, poor quality image and strain related to the view mode. Advancement in 3D technology has made 3D vision more comfortable and acceptable. Comparative assessment of new-generation 3D versus conventional 2D laparoscopy remains limited in clinical urology, and only a few studies address this in the field of general surgery [13].
The use of 3D HD laparoscopic system improves vision quality with accurate depth perception, enabling faster and safer intracorporeal suturing, thereby reducing total operative time with less blood loss, and better overall surgeon performance compared with conventional systems. 3D system offers to fill the gap between 2D laparoscopy and robot assistance.
5 Conclusions
3D Laparoscopic pyelolithotomy is an acceptable and efficient treatment modality for large symptomatic calculi in ectopic fused pelvic kidneys with a malrotated orientation and unfavorable anatomy for the endoscopic approach.
Availability of data and materials
The data that supports the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- 3D: 3:
-
3-Dimensional
- HD:
-
High definition
- PCNL:
-
Percutaneous nephrolithotomy
- SWL:
-
Shock wave lithotripsy
- IVP:
-
Intravenous pyelography
- DJ:
-
Double J Stent
References
Stein RJ, Desai MM (2007) Management of urolithiasis in the congenitally abnormal kidney (horseshoe and ectopic). Cur Opin Urol 17:125–131
Zafar FS, Lingeman JE (1996) Value of laparoscopy in the management of calculi complicating renal malformations. J Endourol 10:379–383
Abeshouse BS, Bhisitkul I (1959) Crossed renal ectopia with and without fusion. Urol Int 9:63–91
Malek RS, Kelalis PP, Burke EC (1971) Ectopic kidney in children and frequency of association of other malformations. Mayo Clin Proc 46:461–467
Glenn JF (1958) Fused pelvic kidney. J Urol 80:7–9
Ward JN, Nathanson B, Draper JW (1965) The pelvic kidney. J Urol 94:36e9
Salvado JA, Guzman S, Trucco CA, Parra CA (2009) Laparoscopic pyelolithotomy: optimizing surgical technique. J Endourol 23:575–578
Tunc L, Tokgoz H, Tan MO, Kupeli B, Karaglan U, Bozkirli I (2004) Stones in anomalous kidneys: results of treatment by shock wave lithotripsy in 150 patients. Int J Urol 11:831–836
Matlaga BR, Kim SC, Watkins SL, Kuo RL, Munch LC, Lingeman JE (2006) Percutaneous nephrolithotomy for ectopic kidneys: over, around, or through. Urology 67:513–517
Chang TD, Dretller SP (1996) Laparoscopic pyelolithotomy in an ectopic kidney. J Urol 156:1753
Ramakumar S, Lancini V, Chan DY, Parsons JK, Kavoussi LR, Jarret TW (2002) Laparoscopic pyeloplasty with concomitant pyelolithotomy. J Urol 167:1378–1380
Polanco Pujol L, Bueno Chomon G, Caño Velasco J, Rodríguez Fernández E, Diez-Cordero JM, Hernández Cavieres J, Blaha I, Hernández FC (2021) Laparoscopic pyelolithotomy in pelvic ectopic kidney: case report and literature review. Actas Urol Esp 45(6):419–426
Patankar SB, Padasalagai GR (2017) Three-dimensional versus two-dimensional laparoscopy in urology: a randomized study. Indian J Urol 33:226–229
Acknowledgements
Not applicable.
Funding
None to be declared.
Author information
Authors and Affiliations
Contributions
Conceptualization and study design, manuscript preparation and manuscript review were done by AK. Conceptualization and study design, generation and collection of data, data analysis and manuscript preparation manuscript review were provided by KK.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Yes, ethical approval obtained from the institutional ethics committee (IEC), VMMC and Safdarjung Hospital New Delhi. IEC/VMMC/SJH/Thesis/2020–03/CC-06) along with the written consent to participate directly from the patient.
Consent for publication
Yes. Obtained directly from patient of legal age.
Competing interests
None to be declared.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Kapoor, K.K., Kumar, A. 3D-Laparoscopic transperitoneal pyelolithotomy in a rare case of pelvic cake kidney: case report and review of literature. Afr J Urol 29, 39 (2023). https://doi.org/10.1186/s12301-023-00368-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12301-023-00368-0