
Abstract
Background
Pseudoaneurysm (PA) of pudendal artery’s distal branches is an extremely rare clinical scenario. We report a case of life-threatening urethrorrhagia due to PA of the internal pudendal artery (IPA).
Case presentation
A 35-year-old man presented with massive urethral bleeding after traumatic urethral catheterization. Failed attempts of conservative management necessitate an emergency intervention with angiography which shows an active extravasation from the left IPA, which was embolized with gel foam, and complete hemostasis was achieved.
Conclusion
PA of the pudendal artery’s distal branches is serious, and majority of cases need an emergency intervention. CT angiography is the best diagnostic imaging, and angioembolization of the bleeding site is considered the first-line treatment. Other treatment options such as US-guided compression, endoscopic coagulation, and open surgery are alternative treatments.
Similar content being viewed by others


1 Background
Continuous or intermittent active urethral bleeding independent of urination is defined as urethrorrhagia, which is an uncommon urological condition [1]. Pseudoaneurysm (PA) of the pudendal artery’s distal branches is a very rare but devastating disorder. It can result following traumatic catheterization with urethral false passage formation [2,3,4,5], iatrogenic urethral injury following internal optical urethrotomy [6], straddle injury [7], and traumatic pelvic fracture [1]. Bleeding in such condition may be massive (> 1000 ml), associated with rapid hemoglobin (Hb) level drop, and the patient becomes hypovolemic requiring an emergency intervention [7].
We present a rare case of massive urethrorrhagia due to internal pudendal artery (IPA) PA caused by iatrogenic traumatic urethral catheterization that was managed successfully by an angioembolization with gel foam.
2 Case Presentation
A 35-year-old male complaining of hypertension, anemia, and end-stage renal disease presented to the ER with complaints of shortness of breath for three days and generalized body swelling. Patient was initially unstable, so he was admitted to the ICU. However, during urethral catheter insertion there were traumatic urethral injury and profuse urethral bleeding. Urology on call-doctor was called, and urethral catheter was fixed properly and with perineal compression bleeding stopped.
On the 3rd day before discharge and after urethral catheter removal, bright-red severe urethral bleeding restarted again. A urology doctor was consulted, he inserted a 3-way 20F Foley’s catheter with good urethral lubrication, traction on thigh, and manual perineal compression was performed for the patient with close monitoring and observation. Urine in bag became clear; however, continuous massive urethral bleeding came out around the catheter that stopped only with penile compression and bandage that was placed for 24 h. After removal of the penile bandage, there was massive re-bleeding again from the urethral meatus around the catheter. Urgent CT angiography of the pelvis was done and showed an active extravasation of contrast in the corpus spongiosum/periurethral area which is due to PA in posterior aspect of the penile urethra (Fig. 1). The patient’s Hb levels dropped steadily from 7 to 5.1 over the past 48 h, and he received three packed RBCs in the ICU. The patient became hypotensive and tachycardic. Following an emergency multidisciplinary meeting, discussing with the patient treatment options available, an agreement and informed consent from the patient were obtained to do a pelvic angiography that was conducted under ultrasound and fluoroscopic guidance to gain access to the right femoral artery. Angiogram of the left internal iliac artery revealed active extravasation of the left IPA, which was embolized with gel foam, and complete hemostasis was achieved (Fig. 2).

CT angiography (axial and sagittal cuts) of the pelvis showing an active contrast extravasation in the corpus spongiosum/periurethral area, which is due to pseudoaneurysm in the posterior aspect of penile urethra (red arrow)

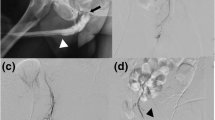
Angiography confirmed a left internal artery pseudoaneurysm, which was successively treated by embolization: An active extravasation of contrast (red arrow) postembolization angiography revealed cessation of flow to the pseudoaneurysm (blue arrow)
The patient tolerated the treatment well and had no complications during or after the embolization. The urethral bleeding stopped at the end of the day after the source of bleeding was embolized, and the Hb level remained stable in the days after the treatment. After a four-month follow-up in the OPD, the patient was voiding normally and had normal erectile function and sexual activity. The manuscript report adheres to CARE guidelines for reporting of case reports.
3 Discussion
External trauma is the commonest cause of urethral injuries that primarily affects men. Clinically the patient is presented by urethrorrhagia, penis ecchymosis, and scrotal/perineal hematoma. The majority of urethral bleeding is small and resolves spontaneously or with conservative treatment including external perineal compression, gentle urethral catheter insertion, antibiotics, close monitoring, stop anticoagulation, and antiplatelet therapy [1].
Massive urethrorrhagia due to PA formation is an extremely rare but devastating event and can lead to hypovolemic shock if one of the pudendal artery’s distal branches is involved, requiring emergency intervention [1,2,3,4,5,6,7]. Different etiological mechanisms have been described for the formation of pseudoaneurysms including traumatic pelvic fracture [1], straddle injury [7], and iatrogenic urethral injury during difficult urethral catheterization [2,3,4,5] or after endoscopic treatment of urethral stricture [6]. The most common involved arteries are the internal pudendal artery [1, 4,5,6,7], the bulbar artery [2], and the obturator artery [3]. Pseudoaneurysm diagnosis is usually made by radiological imaging such as Doppler ultrasound, angio-computed tomography, or angiography [1,2,3,4,5,6,7].
Literature data about this critical condition are sparse, and thus, protocol of management has been based on surgeons’ experience. If conservative therapy is failed and bleeding persists, there are different therapeutic options either by angiography, open, or endoscopic therapy.
Angioembolization is the first-line therapy for arterial bleeding as usual. Previous reports have shown that it is safe, feasible, and effective in controlling severe urethral bleeding due to rupture pseudoaneurysms [1,2,3,4,5]. On the other hand, Attri et al. reported a successful unique management technique of US-guided compression repair for bulbourethral artery pseudoaneurysm following optical internal urethrotomy. They recommended before going for invasive procedure, and this simple technique can be tried specially in small pseudoaneurysm [6]. Furthermore, urethroscopy and direct transurethral coagulation of the bleeding artery in the bulbar urethra have been reported by Yuki and colleagues. In their case, the penile artery was terminal and narrow and they prefer endoscopic management directly as super-selective embolization for targeted artery would be difficult [8]. It is worth to mention that bilateral internal iliac artery ligation for management of massive recurrent urethral bleeding following urethral dilatation has been reported successfully [9]; however, in the era of minimally invasive therapeutic options such as angiography and endoscopy open surgery can be last option if all previous methods failed.
4 Conclusion
Massive life-threatening urethrorrhagia due to PA of the pudendal artery’s distal branches is very rare but devastating condition and needs emergency intervention. CT angiography is the best diagnostic imaging, and angioembolization of the bleeding site is considered the first-line treatment. Other treatment options such as US-guided compression, endoscopic coagulation, and open surgery are alternative treatments.
Availability of data and materials
All articles used in the current review are available from the corresponding author on reasonable request.
Abbreviations
- PA:
-
Pseudoaneurysm
- IPA:
-
Internal pudendal artery
References
Francesco P, Milena C, Antonio B, Francesco G, Fabiol C, Antonio C et al (2020) A singular case of massive urethrorrhagia solved by transarterial embolization. Egypt J Radiol Nucl Med 51:168
Bettez M, Aubé M, El Sherbiny M, Cabrera T, Jednak R (2017) A bulbar artery pseudoaneurysm following traumatic urethral catheterization. Can Urol Assoc J 11(1–2):E47–E49
Huang TY, Huang CN, Lee YC (2013) Life-threatening urethral bleeding induced by a pseudoaneurysm of the obturator artery. Urology 82(6):e43–e44
Luo B, Tang K, Yang W, Lu Z (2022) Massive Urethral bleeding following urethral catheterization induced by a pseudoaneurysm. Urology. https://doi.org/10.1016/j.urology.2022.05.004
Liu S, Deng J, Zeng B, Jia Y (2019) Embolization with microcoils for urethral hemorrhage: a case report. Medicine 98:27
Attri V, Parmar K, Dewana S, Sharma G, Chandna A (2018) Massive bleed following optical internal urethrotomy: an unforeseen doom discussing the unique management technique. J Endourol Case Rep 4(1):179–182
José CS, Nicolás BP, Pablo AA, Vicente SZ, Juan Carlos BP, David CS (2016) Urethrorrhagia secondary to traumatic penile pseudoaneurysm. Urol Case Rep 22(7):10–13
Yuki H, Fuse M, Masuda A, Betsunoh H, Abe H, Yashi M et al (2013) Urethral arterial bleeding from an iatrogenic pseudoaneurysm due to catheterization. Med Surg Urol 2:3
Shah LK, Rao MS, Bapna BC, Vaidyanathan SS, Kapoor VK, Joshi VK et al (1982) Bilateral internal iliac artery ligation for massive recurrent haemorrhage following urethral dilatation: a case report. J Postgrad Med 28:176
Acknowledgements
None.
Funding
No funding was received for this article.
Author information
Authors and Affiliations
Contributions
DT: contributed to evaluation and treatment of index patient, study design, and drafting the manuscript. AH: contributed to literature search, scoping review and data acquisition. SB: contribute to evaluation and treatment of index patient, study design, and critical review of the draft manuscript. MO: contributed to study design, literature search, and drafting the manuscript. IA: contributed to literature search, scoping review and data acquisition. AAR: contributed to evaluation and treatment of index patient, study design, scoping review, drafting the manuscript, literature search, and drafting the manuscript and data acquisition. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
A Written informed consent for publication was sought from the patient.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Taha, DE., Hariri, A., Bahdilh, S. et al. Urethral pseudoaneurysm life-threatening bleeding: a case report and literature review of etiological and treatment options. Afr J Urol 28, 52 (2022). https://doi.org/10.1186/s12301-022-00321-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12301-022-00321-7