
Abstract
Background
While genitourinary tuberculosis is a common form of extra-pulmonary tuberculosis, cold abscess of the epididymis is rare with our literature search finding no reports from the West African subregion. Where the index of suspicion is low, diagnosis is missed and unnecessary surgery may be performed on suspicion of a tumour. The aim of this case report is to highlight the diagnostic challenges of this condition in resource-limited settings in order to create awareness within the health community, increase the chance of appropriate diagnosis, thereby facilitating early commencement of treatment so as to avoid needless testicular loss or complications, such as infertility.
Case presentation
A 33-year-old Black African College-educated public service employee resident in Abuja, Nigeria, presented with a one-week history of right scrotal pain and swelling. Genital examination revealed a firm, non-tender epididymal mass which was initially mistaken for a malignancy. There were no constitutional symptoms, and the contralateral testis was normal. The swelling involved only the epididymis. The testis was distinctly palpable but not oedematous. There was some hemi-scrotal oedema. Blood count and urine cultures were normal. Ultrasound scan showed a hypoechogenic, uniformly enlarged epididymis. Testicular tumour markers were negative. However, CT-abdomen showed enlarged para-caval and pelvic nodes which were thought to be due to secondary deposits from a testicular tumour. Scrotal swelling was later found to be due to an abscess of the epididymis at surgery. Histology showed caseous granulomas typical of Mycobacterium tuberculosis. Gene-Xpert, a cartridge-based nucleic acid amplification test, later confirmed that patient had tuberculosis, for which he is being treated.
Conclusion
The differential diagnosis of an epididymal cold abscess from testicular tumour or chronic epididymitis can be challenging. Therefore, a high index of suspicion as well as a complete tuberculosis screen is essential in an apparently healthy patient presenting with a chronic epididymal swelling.
Similar content being viewed by others


1 Background
Genitourinary tuberculosis is the 2nd most common presentation of extra-pulmonary tuberculosis [1, 2] constituting about 4–15% of cases of tuberculosis [3]. The aim of this case report is to highlight the diagnostic challenges of this condition in resource-limited settings in order to create awareness within the health community, increase the chance of appropriate diagnosis, thereby facilitating early commencement of treatment so as to avoid needless testicular loss or complications, such as infertility. To the best of our knowledge, this is the first case of epididymal abscess reported in Nigeria. Our literature search yielded no tangible report on cold abscess of the epididymis globally.
2 Case presentation
We present a 33-year-old public service employee who presented at the Surgical Outpatient Department with complaints of right scrotal swelling and pain of a week’s duration. Pain was dull, graded 4 on a scale of 10, insidious, non-radiating, aggravated by contact or touch and temporarily relieved by analgesics.
There was no associated urethral discharge, or lower urinary tract symptom. There was no prior history of trauma, strenuous physical activity or fever. He denied weight loss, chronic cough or loss of appetite. He was neither hypertensive nor diabetic. He had had surgery for intussusception at age 4 and hydrocoelectomy at 12. He was not aware of what type of intussusception or hydrocele he had. He was given antibiotics in another hospital before presentation.
He was afebrile. Genitourinary examination revealed a right hemi-scrotal swelling, normally situated right testis and an enlarged, firm, non-tender epididymis. There was a moderate-sized hydrocoele in the right side. The Urologist’s assessment was epididymitis.
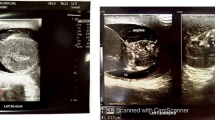
Full blood count (FBC) was normal and Urine Culture showed no significant bacterial growth. Sperm count was 38 million per ml. Scrotal ultrasound scan (USS) showed an enlarged, right testis measuring 5.38 × 3.25 × 3.58 cm (32.83 ml) and a surrounding hydrocoele, and the ipsilateral epididymis appeared inflamed, enlarged and hypoechogenic with a thickened scrotal skin. The left testis measured 4.31 × 3.19 × 3.23 cm or 22.23 ml.
He subsequently presented to two other Urologists, who, on the suspicion of cancer, requested for alpha fetoprotein (AFP), beta human chorionic gonadotropin (HCG) and lactose dehydrogenase (LDH) all of which were within normal limits. A CT scan showed enlarged para-caval and pelvic lymph nodes with “secondary deposits” from a primary tumour in the right testis, as assessed by the radiologist.
On presentation in Kelina Hospital, the scrotal swelling had increased in size. He brought the Radiologist’s report of the abdominal CT scan suggesting a malignant testicular tumor. An agreement was reached between the medical team, the patient and his family for surgical intervention. Transinguinal scrotal exploration revealed an inflamed and heamorrhagic scrotal wall and 500 ml of straw-coloured fluid was evacuated from the tunica vaginalis.
The tunica vaginalis was opened and the epididymis was found to be tensely swollen. The vas deferens was hardened along its entire course. The testis was oedematous but the entire surface was smooth; no nodule was palpated on the testis.
It was decided that since the vas was palpably obstructed, a biopsy of the head of the epididymis would not cause any additional harm to the patient. An incision on the head of the epididymis yielded thick pus (Fig. 1). Pus was also found on the body of the epididymis.

Incision of swollen epididymis yielded thick pus
At this point, a decision was taken to remove the testis completely. Orchidectomy was done with the vas ligated and transected around the deep ring. Procedure was well tolerated and patient was discharged home 2 days later. Specimens were sent for Pathologist’s assessment.
The patient was lost to follow-up until 7 weeks later when he presented with contralateral testicular pain graded 4 on a scale of 10. There was mild swelling and a fever one week prior to presentation which had resolved with self-medication.
Examination findings were an enlarged, left testis and epididymis, positive Phren’s sign and a firm, non-tender left lobe of the prostate on digital rectal examination. A prostatic massage was done and samples were sent for Gram staining and culture which yielded negative results. A sample of the initial abscess also did not grow any bacteria. FBC and urine culture were also normal. Scrotal USS only showed a moderate left vaginal hydrocoele. He was empirically started on parenteral antibiotics (Imipenem) and anti-Koch’s regimen on the suspicion of tuberculous epididymo-orchitis. He was discharged on anti-Koch’s medication and Azithromycin.
The pathologist’s report later came back to us with section of the testis showing granulomatous lesions composed of central necrosis surrounded by epithelioid cells, occasional multinucleated giant cells with characteristic horse shoe-shaped arrangements of the nuclei (Langhans’ giant cells). The lesion was surrounded by peripheral rims of lymphocyte and fibrous tissue. The lesions were more in the epididymis but extending also into the testis; however, AFB stain done was not able to demonstrate the acid-fast bacillus in the tissue, Grocott methenamine silver stain for fungi was negative (Fig. 2).

Micrograph of the testis showing granulomatous inflammation with central necrosis
Patient stopped taking the antituberculous drugs and subsequently developed a discharging sinus on the side of the remaining testis. TB quantiferon gold test confirmed the diagnosis of tuberculosis, and he was re-commenced on the drugs for 5 months before this report. The sinus healed. He is still on his medications at the time of this report.
3 Discussion
This case report confirms other reports which show that diagnosis of a tuberculous epididymitis could be challenging [4]. First, its presentation mimics those of other causes of scrotal swelling [5, 6]. Saad et al. [7] who studied the characteristics of cold tuberculous abscesses reported that common presenting symptoms included pain, a walled swelling and a fistula. Fever was present in less than half of the patients in his series [7].
Commonly, a cold abscess presents as a walled mass which is rarely fluctuant, thus mimicking a tumuor [8] unlike fluctuant, warm abscesses of pyogenic infections. In our patient, the presenting complaint was pain and a non-tender swelling, similar to the presenting complaints of other inflammatory and neoplastic lesions. However, since he was on an antibiotic and non-steroidal analgesic at the time of presentation, it was assumed that the medications had masked the typical presentation of an epididymo-orchitis.
The index patient had no constitutional or pulmonary symptoms. The presence of pulmonary and constitutional symptoms makes the diagnosis of an extra-pulmonary tuberculosis relatively easier [9]. However, only about 35% of cases of genitourinary tuberculosis have been reported with concurrent pulmonary infection [10], with most cases occurring without an active pulmonary infection [11] and so the suspicion of Tuberculosis may not be high until complications set in. The preoperative chest x ray did not show any evidence of Tuberculosis. CT-abdomen did not reveal any renal pathology suggestive of tuberculosis.
Diagnosis of tuberculous epididymitis should be made by identification of the tubercle bacilli from the epididymis [12] on direct examination and culture of pus or histological samples from the edges of the abscess [7, 13]. Supporting diagnostic modalities include urine analysis and culture to isolate the bacilli. In the patient under consideration, no bacilli were isolated.
The ultrasound scan done on the patient showed a hypoechogenic picture which could have been either due to a tumor or an epididymitis. Colour Doppler USS on first presentation did not report any focal linear or spotty blood flow signals. Colour Doppler ultrasound, the first choice for imaging epididymal tuberculosis [14], may be useful in distinguishing between bacterial epididymitis, which appears as diffuse increased blood flow pattern, from tuberculous epididymitis which shows focal linear or spotty blood flow signals in the peripheral zone of the affected epididymis [15, 16].
Histological diagnosis is almost always the most consistent, showing the characteristic picture of granulomatous lesions with central necrosis [17]. However, this is usually done after surgical removal of the epididymis.
The histologic diagnosis is characteristically composed of granulomatous inflammatory lesions which are accumulation of modified macrophages and characteristic multinucleated giant cells (Langhans giant cells). Central caseous necrosis is pathognomonic of Tuberculosis granuloma. AFB is rarely detected using ZN stain but can be demonstrated using immunofluorescence dye Auramine, which is not available in our climes.
4 Conclusion
The differential diagnosis of an epididymal cold abscess from testicular tumour or chronic epididymitis can be challenging. Therefore, a high index of suspicion as well as a complete tuberculosis screen is essential in an apparently healthy patient presenting with a chronic epididymal swelling.
Availability of data and materials
Not applicable.
Abbreviations
- FBC:
-
Full blood count
- USS:
-
Ultrasound scan
- AFP:
-
Alpha fetoprotein
- ß hCG:
-
Beta human chorionic gonadotropin
- LDH:
-
Lactose dehydrogenase
- AFB:
-
Acid-fast bacillus
- ZN:
-
Ziehl–Neelsen Stain
References
Abbara A, Davidson RN (2011) Medscape, Etiology and management of genitourinary tuberculosis. Nat Rev Urol. https://doi.org/10.1038/nrurol.2011.172
Kapoor R, Ansari MS, Mandhani A, Gulia A (2008) Clinical presentation and diagnostic approach in cases of genitourinary tuberculosis. Indian J Urol. https://doi.org/10.4103/0970-1591.42626
Borges WM, Bechara GR, de Miranda MML, de Figueiredo GB, Venturini BA, Laghi CR (2019) Epididymis tuberculosis: case report and brief review of the literature. Urol Case Rep. https://doi.org/10.1016/j.eucr.2019.100969
Man J, Cao L, Dong Z, Tian J, Wang Z, Yang L (2020) Diagnosis and treatment of epididymal tuberculosis: a review of 47 cases. PeerJ. https://doi.org/10.7717/peerj.8291
Rajpal S, Dhingra VK, Malik M, Kumar R (2002) Tuberculous epididymo-orchitis treated with intermittent therapy: a case report. Indian J Allergy Asthma Immunol 16(1):51–54
Zajaczkowski T (2012) Genitourinary tuberculosis: historical and basic science review: past and present. Cent Eur J Urol. https://doi.org/10.5173/ceju.2012.04.art1
Ben Saad S, Kallel N, Gharsalli H, Kwas H, El Gharbi L, Ghedira H, Daghfous H, Tritar F (2018) Cold abscess in the immunocompetent subject. Tunis Med 96(5):302–306
Benjelloun H, Morad S, Zaghba N, Bakhatar A, Yassine N, Bahlaoui A (2015) Cold thoracic parietal abscesses in immunocompetent subjects. Pan Afr Med J. https://doi.org/10.11604/pamj.2015.20.161.5773
Sharma A, Nagalli S, Varughese AT, Ayvazian AM (2020) A review of the diagnostic use of fine-needle aspiration cytology for tuberculosis epididymo-orchitis: to do or not to do. Cureus. https://doi.org/10.7759/cureus.6532
Chirindel A, Martinez F, Gagliardi JA, Armm MF (2008) Testicular tuberculosis without epididymitis simulating neoplasm. Radiol Case Rep. https://doi.org/10.2484/rcr.v3i3.133
Lee IK, Yang WC, Liu JW (2007) Scrotal tuberculosis in adult patients: a 10-year clinical experience. Am J Trop Med Hyg 77(4):714–718
Madeb R, Marshall J, Nativ O, Ertuk E (2005) Epididymal tuberculosis: case report and review of literature. Urology 65(4):798. https://doi.org/10.1016/j.urology.2004.10.029
Cek M, Lenk S, Naber KG, Bishop MC, Johansen TE, Botto H, Grabe M, Lobel B, Redorta JP, Tenke P (2005) Members of the Urinary Tract Infection (UTI) Working Group of the European Association of Urology (EAU) Guidelines Office. EAU guidelines for the management of genitourinary tuberculosis. Eur Urol. https://doi.org/10.1016/j.eururo.2005.03.008
Viswaroop BS, Kekre N, Gopalakrishnan G (2005) Isolated tuberculous epididymitis: a review of forty cases. J Postgrad Med 51(2):109–111
Chudasama N, Sidhu R, Shah N (2016) Classical case of tuberculous epididymo-orchitis and how to rule out differentials on sonography. West Afr J Radiol. https://doi.org/10.4103/1115-3474.162153
Yang DM, Chang MS, Oh YH, Yoon MH, Kim HS, Chung JW (2000) Chronic tuberculous epididymitis: color Doppler US findings with histopathologic correlation. Abdom Imaging. https://doi.org/10.1007/s002610000092
Yadav S, Singh P, Hemal A, Kumar R (2017) Genital tuberculosis: current status of diagnosis and management. Transl Androl Urol. https://doi.org/10.21037/tau.2016.12.04
Acknowledgements
We acknowledge the role of Prof. Friday Odey who provided editorial assistance prior to submission.
Funding
Kelina Hospital.
Author information
Authors and Affiliations
Contributions
CUU conceptualized the work based on history and examination findings. PJ performed histo-pathological examination of the epididymis and testes. EIN was a major contributor in reviewing the relevant literature and writing the manuscript. KRT prepared figures, contributed in writing the manuscript and extensively reviewed all references. Both CUU and PJ reviewed the contents for accuracy. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval for the study was given by the National Hospital, Abuja Health Research Ethics Committee with Approval Number: NHA/EC/098/2020.
Consent for publication
Written informed consent for publication was sought from the patient.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Undie, C.U., Jibrin, P., Nnana, E.I. et al. The diagnostic challenge of a tuberculous cold abscess of the epididymis: a case report. Afr J Urol 28, 39 (2022). https://doi.org/10.1186/s12301-022-00309-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12301-022-00309-3