
Abstract
Background
Genital involvement in neurofibromas is rare and can involve both the clitoris and penis; in the latter, it usually accompanies a systemic pathology. Isolated penile neurofibroma is anecdotal. This report presents an unusual solitary penile neurofibroma in a child, discusses its surgical management and reviews the literature.
Case presentation
A 6-year child presented with history of swelling on the undersurface of his penis and obstructive voiding symptoms since 18 months of age. He underwent a partial excision at 5 years of age elsewhere which recurred. The swelling was a 3 × 2 cm, firm, midline, smooth surfaced, longitudinally oblong mass over the ventral penis extending from root to mid shaft with restricted mobility. There was no inguinal lymphadenopathy. Ultrasonography and cystoscopy characterized it to be a corpus spongiosal soft tissue mass encasing and indenting the contained penile urethra. The mass was completely excised along with involved urethra and corpus spongiosa and a penoscrotal urethrostomy created. Histopathological analysis revealed it to be a benign nerve sheath tumor/neurofibroma. He had no stigmata of neurofibromatosis and the ophthalmologic examination was unremarkable. At 2-year follow-up, he is well, has normal glanular sensation and erectile function and awaits urethral reconstruction.
Conclusion
Primary solitary penile neurofibroma in children is extremely rare. This report details the presentation and management of a ventral penile neurofibroma involving the adjacent urethra/corpora spongiosa.
Similar content being viewed by others


1 Background
Neurofibromatosis type1 (NF1/Von Recklinghausen disease) is an autosomal dominant neurocutaneous disorder with an incidence of 1 in 3000 live birth [1, 2] and may involve any region of the body. Genitourinary neurofibromas can originate from the pelvis, prostatic and/or vesicular nerve plexus, the urinary bladder being the commonly affected urogenital organ. Genital involvement is rare and can involve both the clitoris and penis [3]; in the latter, it usually accompanies a systemic pathology. They are of perineural and schwannian cell origin and arise from the autonomic cavernous plexus in the corporal bodies. This report presents an unusual solitary penile neurofibroma in a child and discusses its surgical management along with a review of literature.
2 Case presentation
A swelling was first noticed at 18 months of age on the undersurface of the penis and had increased in size progressively thereafter. It was excised at 5-years of age and the histopathology was suggestive of a soft tissue neoplasm. He presented to us after a year with a recurrent swelling. He voided with moderate straining but there was no history of retention of urine/hematuria/urinary tract infection.
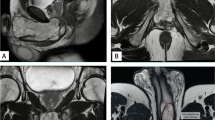
There was a 3 × 2 cm, firm, midline, smooth surfaced, longitudinally oblong mass over the ventral penis extending from root to mid shaft. (Fig. 1a, b) It had a restricted mobility and the inguinal lymph nodes were not palpably enlarged. The urinalysis, complete blood count, renal and liver function tests were normal. Ultrasound showed a mass in the corpus spongiosum encasing the proximal penile urethra (Fig. 1c, d). Cystoscopy (9 Fr scope) showed an extrinsic irregular mass chinking the urethral lumen beginning 3 cm from the meatus proximally for 2 cm (Fig. 2a, b). The bladder was mildly trabeculated and bilateral ureteric orifices were normal. The mass was excised along with the involved urethra and corpus spongiosa with a centimeter margin proximally and distally and a penoscrotal urethrostomy fashioned. Grossly, the 3.4 × 1.8 × 1.7 cm mass was smooth, had greyish white surface and a central bulbous enlargement. Microscopic examination revealed an unencapsulated, highly cellular spindle cell tumor. The cells were arranged in predominantly fascicular and focally storiform pattern, and they showed mild nuclear atypia and focal degeneration. The cytoplasm was positive for S-100 and the vessels positive for CD34, a diagnosis of a benign nerve sheath tumor—localized neurofibroma was made (Fig. 3). He had no stigmata of NF I and the ophthalmologic examination was unremarkable. There are no signs of recurrence of the tumor after 2 years (Fig. 4a, b), and the ultrasound shows postoperative changes around the urethrostomy with normal adjacent urethra (Fig. 4c, d). The glanular sensation and erectile functions are preserved and he awaits urethral reconstruction.

Clinical photographs (a, b) showing a ventral, oblong, proximal penile bulge (arrow). Longitudinal (c) and transverse (d) sonographic gray scale images with the probe ventral, shows a well-circumscribed mass (M) in the corpus spongiosum (S), which is isoechoic to the corpus cavernosum (C). The mass (M) is encasing the proximal penile urethra (arrow)

Cystoscopic views of the penile urethra indented by an extrinsic, irregular mass (arrows)

Photomicrograph showing A cellular spindle cell tumour with minimal nuclear and cellular pleomorphism and intermixed collagen (Hematoxylin and eosin, 200 X); B S 100p is diffusely and strongly positive (IHC X 200)

Postoperative clinical photographs (a, b) after resection of the mass. Note the gap (arrow) between the urethrostomies and the distal penile urethra (yellow asterisk). Longitudinal (c) and transverse (d) sonographic gray scale images with the probe dorsal, shows post-operative changes (arrows) in the proximal penile shaft with non-visualization of the mass, corpus spongiosum and proximal urethra. Distal penile shaft shows normal urethra (asterisk) within the corpus spongiosum (S). C indicates corpus cavernosum
3 Discussion
Diagnosis of NF1 is clinical with the presence of at least two of the seven criteria—Six or more café-au-lait spots, two or more cutaneous or subcutaneous neurofibroma/ a plexiform neurofibroma, axillary or groin freckling, two or more Lisch nodules, optic pathway glioma, bony dysplasia and first degree relative with NF1 [2]. Genitourinary tract involvement in NF 1 has a prevalence of 0.65% with urinary bladder being the most commonly affected organ due to an abundance of autonomic nerves. Common extra vesical sites include renal hilum, ureters, uterus and prostate [3].
External genital involvement in neurofibromatosis is comparatively infrequent, clitoromegaly being the most common [3]. Penile involvement is usually associated with concomitant genitourinary involvement. Isolated penile neurofibroma is extremely rare, and only 17 cases of primary solitary neurofibroma of penis have been documented in children under 16 years since 1950 (Table 1) [1, 4,5,6,7,8]. Features of NF 1 were present in 10, and the rest were histological surprises. Two (Case 4, 14) had significant neurological affliction. The histology was described as plexiform (13/17), solitary (3/17) or left unqualified (2/17). Complete excision of the neurofibroma was curative in ten. In dorsal penile neurofibroma arising close to the neurovascular bundle, a complete resection preserving the bundle is technically impractical and somato-sensory deficit must be weighed against cosmesis. Partial resection is associated with recurrence and possible malignant transformation in 5–15% cases. In seven who had partial excision, five were curative. One had a local recurrence 2 months after surgery and underwent partial penectomy for a definitive cure thereafter. The case with multiple cranial nerve palsies and quadriplegia died later due to neoplasia elsewhere (cerebral ependymoma). Although the short-term follow-up mentions improvement and no recurrence, long-term follow-up data are lacking.
In contrast, the lesion described here was located on the ventral aspect of the penis and indented the urethra. The management aimed at complete resection with a cuff of normal tissue and delayed urethral reconstruction.
4 Conclusions
Primary solitary penile neurofibroma in children is extremely rare. This report details the presentation and management of a ventral penile neurofibroma involving the adjacent urethra/corpora spongiosa. Total excision of neurofibroma is ideal; however, partial excision do give good results with rare instances of recurrence. Long term follow of these cases is warranted to detect any recurrence and malignant transformation.
Abbreviations
- NF1:
-
Neurofibromatosis type1
References
Banthia R, Yadav P, Agarwal R, Lal H (2020) Plexiform neurofibromatosis of penis: a rare presentation of type 1 neurofibromatosis. BMJ Case Rep 13:e236542
Gao B, DeCotiis K, Bobrowski A, Koyle M, O’Kelly F (2020) The association of neurofibromatosis type 1 and lower urinary tract dysfunction in the paediatric population: a critical review of literature. J Pediatr Urol 16(3):357–65
Pascual-Castroviejo I, Lopez-Pereira P, Savasta S, Lopez-Guitierrez JC, Lago CM, Cisternino M (2008) Neurofibromatosis type 1 with external genitalia involvement presentation of 4 patients. J Pediatr Surg 43:1998–2003
Kousseff BG, Hoover DL (1999) Penile neurofibromas. Am J Med Genet 87:1–5
Littlejohn JO, Belman AB, Selby D (2000) Plexiform neurofibroma of the penis in a child. Urology 56(4):669. https://doi.org/10.1016/S0090-4295(00)00730-5
Mazdak H, Gharaati MR (2007) Plexiform neurofibroma of penis. Urol J 4:52–54
Ballouhey Q, Longis B, Couvrat-Carcauzon V, Gardic S, Piguet C, Berenguer D et al (2013) Neurofibroma and epidermoid cyst: unexpected findings after first foreskin retraction. Urology 82(6):1419–1420. https://doi.org/10.1016/j.urology.2013.06.014
Collins NC, Ayodeji EE, Motunrayo FO, Abayomi SB, Olufemi OI, Olusesan AL (2018) Large penile plexiform neurofibroma in an 11 year old boy. Malawi Med J 30(1):49–51
Acknowledgements
We thank the patient and his family to be very supportive and having faith on us for the treatment.
Funding
No funding received.
Author information
Authors and Affiliations
Contributions
Case conception and design: SKM. Acquisition of data: MSA/BS/MNS, KD. Analysis and/or interpretation of data: SKM, KD. Drafting the article: MSA/SKM. Images design: BS/MNS/KD. Revising it critically for important intellectual content: ABP/KD. All authors contributed to the final approval of the version to be published. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures performed in this study were in accordance with the ethical standards of our institutional review board with the 1964 Helsinki declaration. Consent for this surgery was obtained from the patient and her father.
Consent for publication
Consent for publication of this report was obtained from the patient and his father.
Availability of data and materials
Not applicable.
Competing interests
None to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Ahmad, M.S., Mahalik, S.K., Sahoo, B. et al. Primary solitary neurofibroma of penis in a child: case report and review. Afr J Urol 28, 20 (2022). https://doi.org/10.1186/s12301-022-00286-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12301-022-00286-7