
Abstract
Background
Primary adenocarcinoma of renal pelvis or ureter is rarest (< 1%) among all urothelial tumors. Regrettably, no characteristic symptoms, radiological features and treatment for this tumor are reported. We report three cases of adenocarcinoma of renal pelvis and ureter.
Case presentation
Case 1 had grossly hydronephrotic non-functional right kidney and underwent percutaneous nephrostomy followed by laparoscopic simple nephrectomy. Incidentally, histopathological examination reported adenocarcinoma of renal pelvis. Whole-body positron emission tomography-CT (PET-CT) ruled out malignancy at other sites. Patient refused adjuvant chemotherapy. Case 2 presented with previous history of right pyelolithotomy, right ureteroscopic lithotripsy and right flank pain with intermittent discharge via previous percutaneous site. On biochemical and radiological investigations, right poorly functioning pyonephrotic kidney was confirmed. Patient underwent right open nephrectomy which incidentally reported adenocarcinoma of renal pelvis. Patient is disease-free at 18 months of follow-up. Case 3 had left ureteric wall thickening on CT scan when evaluated for hematuria. Ureteroscopic-guided biopsy showed villous adenoma. Laparoscopic left nephroureterectomy with bladder cuff excision specimen showed well-differentiated adenocarcinoma in ureter with extension into periureteric fat. Patient died 32 months after surgery.
Conclusion
Primary adenocarcinoma of renal pelvis or ureter is very rare and urologists should suspect it in patients with mucinous material in nephrostomy tube. We should have a low threshold for performing radical nephrectomy with complete ureterectomy in these unusual cases to improve the prognosis.
Similar content being viewed by others


1 Background
Primary adenocarcinoma of renal pelvis or ureter is rarest (< 1%) among all urothelial tumors. They are further sub-classified into tubulovillous (71.5%), mucinous (21.5%) and papillary (7%) [1]. Till date < 150 cases have been reported worldwide. Herein, we present our experience with three patients of adenocarcinoma of renal pelvis or ureter in the past six years.
2 Case presentation
2.1 Case 1
A 40-year-old male non-smoker presented with a four months history of right flank pain without fever and hematuria. He underwent right open pyelolithotomy 10 years back. Abdominal examination revealed right renal angle tenderness. Routine hematological investigations were normal. There was no red or pus cell on urine analysis. Serum creatinine was 0.7 mg/dL.
Abdominal sonography showed gross right hydronephrosis. Multiphasic contrast-enhanced abdominal tomography (CECT) revealed grossly hydronephrotic right kidney with papery thin parenchyma and few small calculi in lower and middle calyx. Right ureter was not dilated (Fig. 1a). DTPA renal scanning revealed 5% split function of the right kidney.

a Contrast-Enhanced computed tomography shows right grossly hydronephrotic kidney with thin cortex and non-excreting right kidney on delayed film. b Resected nephrectomy specimen showing gelatinous polypoidal material inside calyx. c Microscopic section displaying proliferation of atypical columnar epithelial cells with multiple acini and few papillary fronds
A percutaneous nephrostomy (PCN) was placed that drained a small quantity of gelatinous material which did not show malignant changes on cytopathological examination. The patient underwent laparoscopic simple nephrectomy without total ureterectomy with intraoperative spillage of mucinous content.
Gross pathological examination of the kidney showed gelatinous polypoidal material in calyces and pelvis (Fig. 1b). Microscopic examination shows the renal pelvis was composed of atypical columnar epithelial cells with multiple acini and few papillary fronds suggestive of adenocarcinoma (Fig. 1c). Whole-body positron emission tomography-CT (PET-CT) ruled out any other site for adenocarcinoma.
Adjuvant chemotherapy was offered to the patient considering the intraoperative spillage, but the patient refused. Patient was asymptomatic with normal CECT Chest and abdomen-pelvis for a recorded follow-up period of 12 months.
2.2 Case 2
A 60-year-old male underwent right open pyelolithotomy 2 years prior for renal calculi. After six months he was diagnosed with an obstructive right mid-ureteric calculus and underwent right PCN insertion followed by right ureteroscopic lithotripsy at peripheral center. After 3 months, he presented to us with right side flank pain and intermittent discharge from the previous nephrostomy site. He was afebrile with no history of hematuria. Hematological investigation showed elevated total leucocyte count of 18,500 cells/mm3 [Normal range: 4,000–11,000 cells/mm3] and serum creatinine 1.2 mg/dl. Urinalysis showed 60–70 pus-cells/hpf. CECT showed grossly hydronephrotic right kidney and a loculated perinephric hypodense collection with peripheral enhancement communicating the pelvicalyceal system (PCS). The right renal cortex was papery thin and no contrast excretion was seen on delayed scan (Fig. 2a). Considering a right renal abscess as the working diagnosis, a right PCN was inserted. Thick pus along with mucoid material was drained. Preoperative working diagnosis of a pyonephrotic non-functional kidney was made, and the patient underwent open right nephrectomy. Intraoperatively dense perinephric adhesions were present with spillage of mucoid material at some places. Gross pathological examination showed grossly dilated PCS filled with gelatinous material and multiple brownish papillary nodules seen on the surface of renal pelvis and calyces (Fig. 2b). Histopathological examination showed neoplastic glands lined by pseudostratified columnar epithelium with vacuolated cytoplasm suggestive of well-differentiated adenocarcinoma (Fig. 2c). Final pathological stage pT3aNx in light of opened PCN tract. PET-CT ruled out any other site of origin of disease. The patient was disease-free by the 18-month postoperative follow-up.

a Contrast Abdominal computed tomography reveals right side severe hydronephrosis with perinephric collection communicating with right pelvic calyceal system. b Dilated PCS along with filled gelatinous material and multiple brownish papillary nodules found on the surface of renal pelvis and calyces. c Glands and papillae lined by pseudostratified columnar epithelium and show characteristics of adenocarcinoma
2.3 Case 3
A 57-year-old male non-smoker presented with three episodes of painless hematuria along with intermittent pain in the left flank. He was afebrile with unremarkable past history. His routine hematological and urine investigations were normal.
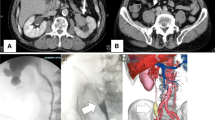
CT urography showed thickened enhancing mid-ureteric wall with luminal narrowing involving the short segment of left ureter. Non-excretion of contrast in the pelvicalyceal system was reported even on 15 min delayed scan (Fig. 3a). Rest all organs were normal. Urine cytology was negative.

a CT urography showing left hydronephrosis along with non-excretion of contrast secondary to luminal narrowing at mid ureter. b Ureteroscopy showed left irregular mass with intraluminal protrusion at mid ureter. c Microscopic section from ureter shows atypical acini present in muscularis and extending into periureteric tissue
Cystoscopic evaluation of bladder was unremarkable and ureteroscopic showed intraluminal protruding irregular mass in left mid ureter. Ureteroscopic-aided biopsy of left ureteric mass reported villous adenoma (Fig. 3b). DTPA renal scan revealed poorly functioning left kidney with GFR of 14 ml/min. The contralateral kidney was normal. The patient underwent laparoscopic left nephroureterectomy with bladder cuff excision. Intraoperatively, the ureter was clipped distal to mass and tissue sent for frozen section showed presence of tumor. Subsequently, entire ureter along with bladder cuff excision was done.
Histopathological examination reported 1 × 0.5 cm well-differentiated adenocarcinoma in ureteric segment which invades beyond muscularis into periureteric fat (Fig. 3c). In view of piecemeal resection of distal ureteric segment, chemotherapy was advised to patient but he denied. Patient succumbed to death 32 months after surgical intervention.
3 Discussion
Although rare, most renal pelvic or ureteric adenocarcinoma is reported from Asian countries [1]. The pathogenesis of adenocarcinoma considers chronic inflammation or obstruction leading to glandular metaplasia of the urothelium which subsequently undergoes malignant transformation. Pelvic stone causing chronic inflammation was seen in two cases in our series.
No characteristic symptoms of adenocarcinoma are mentioned in literature. In the present case series, all patients had flank pain and one patient had hematuria. Diagnosing adenocarcinoma preoperatively is difficult as no distinctive radiological features exist for this entity.
Abbas et al. [2] stated that no characteristic radiological feature exists for adenocarcinoma. In our series, all patients had hydronephrotic kidney with non-excretion of contrast. Considering its rare incidence, there exists no recommended standard surgical procedure for adenocarcinoma of renal pelvis or ureter. Most patients underwent nephrectomy without complete ureterectomy [1]. In our case series, two patients underwent simple nephrectomy and one underwent nephroureterectomy with bladder cuff excision. Postoperative histopathological examination confirms the final diagnosis as two cases in our series surprisingly showed adenocarcinoma of renal pelvis. Considering low incidence of this disease and lack of prospective trails, role of adjuvant chemotherapy or radiotherapy should be individualized [3].
The overall prognosis of adenocarcinoma of renal pelvis or ureter is poor as published literature reported death of 50% patients within two years of surgery [4]. In our case series, 1 out of 3 patients expired after 32 months of surgery.
4 Conclusions
Primary adenocarcinoma of renal pelvis or ureter is very rare. Mucinous material in nephrostomy tube should alert treating surgeon and he should have a low threshold for performing radical nephrectomy with complete ureterectomy in these unusual cases.
Availability of data and material
All patient data are stored in our database.
Abbreviations
- HSK:
-
Horseshoe kidney
- CECT:
-
Contrast-Enhanced Abdominal Tomography
- PCN:
-
Percutaneous nephrostomy
References
Li H, Xie F, Zhao C, Yi Z, Chen J, Zu X (2020) Primary mucinous adenocarcinoma of the renal pelvis misdiagnosed as calculous pyonephrosis: a case report and literature review. Transl Androl Urol 9(2):781
Abbas M, Kramer MW, Spieker T, Herrman TR, Merseburger AS, Müller KM, Kuczyk MA, Becker JU, Kreipe HH (2014) Primary mucinous adenocarcinoma of the renal pelvis with carcinoma in situ in the ureter. J Egypt Natl Canc Inst 26(1):51–54
Chaudhary P, Agarwal R, Srinivasan S, Singh D (2016) Primary adenocarcinoma of ureter: A rare histopathological variant. Urol Ann 8(3):357
Han DS, Yuk SM, Youn CS, Park G, Sul HJ, Jang H (2015) Primary mucinous cystadenocarcinoma of the renal pelvis misdiagnosed as ureteropelvic junction stenosis with renal pelvis stone: a case report and literature review. World J Surg Oncol 13(1):1–5
Acknowledgements
We would like to acknowledge the contribution of Dr. Shailesh Soni (Department of Pathology) in helping us with proper histopathological diagnosis and pictures.
Funding
The case study did not receive any funds from any source.
Author information
Authors and Affiliations
Contributions
S.A.: Writing manuscript; A.G.S.: Editing manuscript; R.B.S.: Editing manuscript; M.D.: Editing manuscript. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Our institution does not require ethics approval for reporting individual case reports.
Consent for publication
Written informed consent for publication was obtained from the patients (Case 1 and 2) and from the relative of patient (Case 3) for the anonymized information and the accompanying images to be published in this article.
Competing interests
The authors declare that there is no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Agrawal, S., Singh, A.G., Sabnis, R.B. et al. Primary adenocarcinoma of renal pelvis or ureter: an uncommon histopathological entity seen in three cases. Afr J Urol 27, 161 (2021). https://doi.org/10.1186/s12301-021-00262-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12301-021-00262-7