
Abstract
Background
Fournier’s gangrene and trauma to the external genitalia are the commonest causes of peno-scrotal wound defects in our environment. The management of these patients includes initial resuscitation and subsequent wound care with or without wound cover. The aim of this study is to document our experience in the management of peno-scrotal defects in a tertiary hospital of North-Western Nigeria.
Methods
This is a 20-year retrospective study of patients managed for peno-scrotal wound defects by the Urology Unit in the Department of Surgery of our hospital from January 2001 to December 2019. Data were collected from the patients’ case notes and entered into a proforma. Data were analysed using SPSS version 25.0.
Results
A total number of 54 patients with peno-scrotal wound defects were managed within the study period with the mean age of 46.27 ± 22.09 years and a range of six weeks to 107 years. The wound defects were sequelae of Fournier’s gangrene in 42 patients (77.8%) and traumatic in 12 patients (22.2%). Healing by secondary intention was achieved in 20 patients (37.0%). Direct closure was done in 17 patients (31.5%), skin graft in nine patients (16.7%), and advancement flap in eight patients (14.8%) depending on the location and size of the defects. Fourteen patients (26.0%) developed surgical site infection ± wound dehiscence and partial graft loss. The complication rate was higher in post-Fournier’s gangrene wound defects, but without statistical significance (p = 0.018).
Conclusion
Fournier’s gangrene and trauma to the external genitalia are the commonest causes of peno-scrotal wound defects in our environment. Smaller wound defects were healed by secondary intention, while larger defects required either direct closure or the use of advancement flap or skin grafting depending on the location and size of the wound. The study reported a higher post-repair complication in patients that had Fournier’s gangrene.
Similar content being viewed by others

1 Background
Peno-scrotal wound defects are common sequelae of Fournier’s gangrene, trauma to the external genitalia, as well as skin malignancies involving peno-scrotal area and extramammary Paget disease [1,2,3,4,5]. The management of the defects becomes important after tackling the emergent or sinister issues related to the fulminant infection, trauma, and malignancy [6]. The wound cover facilitates healing, urological, sexual, and psychological functions of the patient [3, 7], thereby improving the quality of life of the patients. Reconstruction of the scrotum may be challenging because of the differences in skin colour, texture, difficulty in tissue mobilization, propensity for infection, tissue tension, and the presence of intercurrent illnesses [3, 8, 9].
Option of management depends on the location of the defect, size, and state of the surrounding skin [3]. Most of the scrotal defects are amenable to direct closure or healing by secondary intention if small (2–5 cm), while larger defects require advancement or rotational flaps [5, 8]. Due to the inelastic nature of the penile skin, most of the penile defects away from the scrotum may be managed by skin graft and local flaps [3, 5, 10].
The aim of this study is to document our experience in the management of peno-scrotal wound defects within the last 20 years.
2 Methods
This is a 20-year retrospective study of consecutive patients managed for peno-scrotal wound defects by the Urology Unit in the Department of Surgery of our hospital from January 2001 to December 2019. Data were collected from the patients’ case notes as well as theatre register and entered into a proforma. Information retrieved included biodata, presentation, aetiology, intercurrent diseases, results of laboratory investigations, treatment offered, complications and their management, and overall outcome. The study excluded patients with incomplete records. Data were analysed using the SPSS version 25.0. The study was approved by Health Research and Ethics Committee of our institution.
3 Results
A total number of 54 patients with peno-scrotal wound defects were managed within the study period with mean age of 46.27 ± 22.09 years and a range of 6 weeks to 107 years. The wound defects were sequelae of Fournier’s gangrene in 42 patients (77.8%) and traumatic in 12 patients (22.2%).
The commonest form of presentation was scrotal or penile swelling with or without ulceration and discharge. This occurred in 43 patients (79.6%). Other forms of presentation were as shown in Table 1.
Wound defects that occurred as a result of Fournier’s gangrene were found in 42 patients (77.8%), road traffic accidents accounted for 10 patients (18.5%), gunshot accounted for a case (1.9%), and excision of malignant peno-scrotal ulcer also accounted for one case.
Urethral stricture was the commonest predisposing factor to Fournier’s gangrene as seen in 10 patients (18.5%). Other predisposing factors are presented in Fig. 1 below.

A bar chart showing predisposing factors in the patients with Fournier’s gangrene
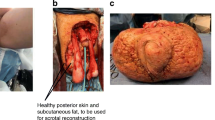
The wound defects were scrotal in 26 patients (48.1%), peno-scrotal in 20 patients (37.0%), and penile in 8 patients (14.8%). Peno-scrotal wound defect with extension to the lower anterior abdominal wall is indicated in Fig. 2.

Peno-scrotal wound defect with extension to the lower anterior abdominal wall is shown in Fig. 3
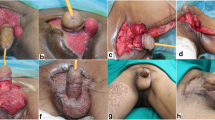
Small wound defects of sizes 2 cm were healed by secondary intention, and direct closure ± advancement flap was performed on 25 patients (46.3%) with defects greater than 2 cm. Other details of the treatment offered are shown in Table 2. Scrotal advancement flap and penile skin grafts are presented in Figs. 3 and 4.

Scrotal advancement flap (a) for anterior and (b) posterior scrotal defect

Penile skin graft
The complications encountered were surgical site infection (SSI) ± wound dehiscence in 9 patients (16.7%) and partial graft loss in 5 patients (9.3%) as shown in Fig. 5. Complete wound healing was achieved with wound dressing, and wound reclosure was performed on 4 patients (7.4%). The rate of complications in Fournier’s gangrene group was 20.4%, which was higher than the 9.3% in the trauma group. The rate of SSI + wound dehiscence and graft loss in Fournier’s gangrene group doubled the rate in the trauma group as shown in Fig. 6. The difference was not statistically significant (p = 0.18).

Complication: partial penile skin graft loss and superficial wound dehiscence secondary surgical site infection post-scrotal advancement flap

A bar chart showing distribution of complications in Fournier’s gangrene (FG) and trauma group
4 Discussion
Peno-scrotal wound defects are common sequelae of Fournier’s gangrene, trauma to the external genitalia, as well as skin malignancies involving peno-scrotal area and extramammary Paget disease [1,2,3,4,5]. The management of the defects becomes important after tackling the emergent or sinister issues related to the fulminant infection, trauma, and malignancy [6]. The wound cover facilitates healing, urological, sexual, and psychological functions of the patient [3, 7], thereby improving the quality of life of the patients.
The mean age of patients in this study was 46 years, which is comparable with the 45 years reported by Karki et al. [7], but lower than the 93 years reported by Kyung et al. [3]. This may be associated with lower life expectancy in developing countries.
The commonest presentation was the penile and or scrotal swelling—with or without ulceration—and wound discharge as reported by previous studies [11, 12].
The commonest cause of the peno-scrotal wound defects in our study was Fournier’s gangrene. This is similarly reported by previous studies [2, 5, 7,8,9]. The study recorded a case of malignant ulcer in the peno-scrotal region, but no case of extramammary Paget disease although it has been reported by some other studies [3, 7, 8].
Most of the patients (46%) in our study, especially those who have Fournier’s gangrene, presented with other underlying medical or urological conditions, which impacted negatively on wound healing and outcome of the treatment. This has also been reported by previous studies [1, 5, 8].
The authors achieved closure of all the scrotal defects with either advancement flaps—specifically in cases where the scrotal defects are not amenable to healing by secondary intention—or direct closure even in those with available scrotal skin less than 50%. This is contrary to what was reported by other authors that closure of the scrotum may be impossible when residual skin is less than 50% [8]. This became possible with the ability to create more space in the soft tissues of the groin and perineum [5, 8]. By rule, almost all the penile defects were covered with skin graft except a patient whose penile defect was covered by staged advancement flaps from the suprapubic and perineal regions with resultant moderate penile wound defect that healed by secondary intention while awaiting skin graft. The simpler the approach, the better the outcome as reported by various studies [3, 5, 7, 8]. The researcher did not use pedicled flaps such as Gracilis myocutaneous, pudendal artery, or circumflex artery perforator flaps in any of our patients as against what was reported by some studies [3, 6, 13].
The commonest complications recorded in our series were surgical site infection—with or without wound breakdown and partial graft loss as reported by previous studies [3, 8]. The higher complication rate in Fournier’s gangrene group is not unexpected due to the nature of the primary condition being an infective process as compared to the trauma group in which the wound gets infected secondarily. The gunshot wounds are primarily dirty; hence, they have similar complications rate to Fournier’s gangrene wounds. Notwithstanding, all the complications were equally managed successfully with antibiotics, wound dressing, and reclosure of the wound with good outcome.
5 Conclusion
Fournier’s gangrene and external genital trauma are the commonest causes of peno-scrotal defects in our environment. Smaller defects can easily heal following dressing by secondary intention or direct closure. Larger defects, more especially, in the penis require advancement flaps and or skin graft. The commonest complications were surgical site infection, wound breakdown, and partial graft loss. The complication rate was higher in post-Fournier’s gangrene wound defects. All the complications were managed with good outcome by wound dressing—with or without wound closure—depending on the size of the defect.
Availability of data and materials
The data and materials are available on request.
References
Chen SY, Fu JP, Chen TM, Chen SG (2011) Reconstruction of scrotal and perineal defects in Fournier’s gangrene. J Plast Reconstr Aesthetic Surg 64(10):1392–1393
Houben CH, Azubuike C, Ozoemena O, Saidu B (2013) Scrotal necrosis to total de-gloving injury of the male genitalia: an experience from Sub-Saharan Africa. Healthc Low Resour Settings 1:16–20
Kyung H, Kwon H, Song S-H, Oh S-H (2018) Reconstruction using local flaps for penoscrotal defects after ablation of skin lesions. J Wound Manag Res 14(1):37–43
Hunter CL, Skinner EC, Lee GK (2015) Reconstruction with pedicled anterolateral thigh flap after wide local excision of penoscrotal extramammary Paget’s disease: a case report and comprehensive literature review. Eplasty 15:155–169
Bryk DJ, Yamaguchi Y, Zhao LC (2015) Tissue transfer techniques in reconstructive urology: review article. Korean J Urol 56(7):478–486
Han HH, Lee JH, Kim SM, Jun YJ, Kim YJ (2016) Scrotal reconstruction using a superficial circumflex iliac artery perforator flap following fournier’s gangrene. Int Wound J 13(5):996–999
Karki D, Patel PK, Narayan RP (2016) Penoscrotal defect: a functional, esthetic, and psychological challenge. Plast Aesthet Res 3:64–67
Karian LS, Chung SY, Lee SE (2014) Reconstruction of defects afterFournier’s gangrene: a systematic review. Eplasty 15:155–170
Ahn DK, Kim SW, Park SY, Kim YH (2014) Reconstructive strategy and classification of penoscrotal defects. Urology 84:117–1222
Obi AO (2016) Isolated Fournier’s gangrene of the penis. Niger J Clin Pract 19:426–430
Bhatnagar AM, Mohite PN, Suthar M (2008) Fournier’s gangrene: a review of 110 cases for aetiology, predisposing conditions, microorganisms, and modalities for coverage of necrosed scrotum with bare testes. N Z Med J 121:46–56
Mallikarjuna MN, Vijayakumar A, Patil VS, Shivswamy BS (2012) Fournier’s gangrene: current practices. Int Sch Res Netw 2012:942436
Karsidag S, Akcal A, Sirvan SS, Guney S, Ugurlu K (2011) Perineoscrotal reconstruction using a medial circumflex femoral artery perforator flap. Microsurgery 31(2):116–121
Acknowledgements
We thank Prof. Aminu Mode, Department of Modern European Languages and Linguistics, Usmanu Danfodiyo University Sokoto, Nigeria, for grammatical corrections.
Funding
No external funding was received. The cost of the study was borne by the authors.
Author information
Authors and Affiliations
Contributions
ASM contributed to concept, design, data collection, data analysis, literature review, writing, preparation, revision of critical content, and final approval. NPA, AUM, and BMA performed data collection, revision of critical contents, and final approval. AAA was involved in review of critical content, concept, design, and final approval. MUM performed critical review and final approval. JNL contributed to concept, design, review of critical contents, and final approval. IAM was involved in concept, design, and final approval. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
The study was approved by ethical and research Committee of Usmanu Danfodiyo University Teaching Hospital (UDUTH/HERC 2018/no. 720). Consent to participation was obtained from the patients whose pictures appeared in the manuscript.
Consent for publication
Consent for publication was obtained from the patients whose pictures appeared in the manuscript.
Competing interest
No competing interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Muhammad, A.S., Agwu, N.P., Abduwahab-Ahmed, A. et al. Management of peno-scrotal wound defects in a tertiary hospital in North-Western Nigeria: a 20-year retrospective review. Afr J Urol 27, 67 (2021). https://doi.org/10.1186/s12301-021-00167-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12301-021-00167-5