
Abstract
Background
Klebsiella pneumoniae invasion syndrome (KPIS) is a severe multi-site infection that is usually caused by hypervirulent Klebsiella pneumoniae. The bacteria are relatively common in Asian diabetics and can cause organ abscesses or sepsis. When patients develop intracranial infection, the prognosis is poor. After anti-infective treatment, the Klebsiella pneumoniae-induced liver and lung abscesses and pulmonary fungal infection were relieved, but the brain abscesses worsened. Such complex and severe infection cases are rarely reported. Early identification of intracranial infection, selection of antibiotics with high concentrations in cerebrospinal fluid, and active treatment of complications such as diabetes and fungal infection are of great significance for the prognosis of patients.
Case presentation
A 71-year-old patient diagnosed with liver abscess in another hospital was transferred to our hospital due to a worsening condition. On day 1 (day of admission), the patient was given invasive mechanical ventilation, continuous renal replacement therapy combined with endotoxin adsorption, antimicrobial treatment with imipenem-cilastatin, and percutaneous catheter drainage for liver abscess. Metagenomic next-generation sequencing in bronchoalveolar lavage fluid indicated Klebsiella pneumoniae (K. pneumoniae), Candida albicans, and Aspergillus flavus complex, and no viruses were detected. Blood and pus cultures revealed K. pneumoniae that was sensitive to piperacillin/tazobactam. The anti-infection therapy was adjusted to piperacillin/tazobactam combined with voriconazole. On day 14, a head computed tomography (CT) scan showed no significant changes, and a chest CT scan showed absorption of multiple abscesses in both lungs. The patient was still unconscious. After the endotracheal tube was removed, cranial magnetic resonance imaging (MRI) showed multiple brain abscesses. Finally, his family gave up, and the patient was discharged and died in a local hospital.
Conclusion
In cases of K. pneumoniae infection, the possibility of intracranial, liver, lung, or other site infections should be considered, and physicians should be vigilant for the occurrence of KPIS. For patients suspected of developing an intracranial infection, cerebrospinal fluid should be tested and cultured as soon as possible, a head MRI should be performed, and antibiotics with high distribution in cerebrospinal fluid should be used early. When patients are complicated with diabetes, in addition to glycemic control, vigilance for concurrent fungal infections is also needed.
Similar content being viewed by others


Introduction
Liver abscess is one of the most common visceral abscesses. The risk factors include diabetes, hepatobiliary, and pancreatic diseases. Gram-negative bacilli such as Escherichia coli and Klebsiella pneumoniae are the main pathogens associated with liver abscesses [1]. K. pneumoniae was more common in Asian patients than in non-Asian patients (50% vs 27%, respectively) [2]. In a recent meta-analysis, diabetes and liver abscess (pooled risk ratio: 2.61 and 9.04; all P < 0.001) were predictors of hypervirulent K. pneumoniae (hvKp) infections [3]. Patients infected with hvKp or with poor glycemic control of diabetes may progress to KPIS with multiple abscesses of the liver, lung, brain, and other sites [4, 5]. It has been reported that the mortality of K. pneumoniae meningitis is 53% [6], and the mortality is significantly increased when multiple abscesses, such as those in the liver and brain, occur at the same time [7]. Fungal infection also increases the risk of death [8]. In this case report, we share a rare case of KPIS with the liver, lung, and brain abscesses complicated with pulmonary fungal infection in a diabetic patient with poor glycemic control.
Case presentation
A 71-year-old man presented with fever and dyspnea for 3 days. His highest temperature was 39.5°C, accompanied by dyspnea, nausea, and vomiting. The patient also experienced dizziness and fatigue, with no headache, chest pain, abdominal pain, altered consciousness, etc. One day before admission, the patient visited a local hospital. Laboratory investigations revealed a white blood cell (WBC) count of 13.97 *10^9/L [reference range: 3.5–9.5 *10^9/L], neutrophil percentage of 91.8% [reference range: 40–75%], platelet (PLT) of 54 *10^9/L [reference range: 100–300 *10^9/L], and CRP of 313.96 mg/L [reference range: < 10 mg/L]; hypersensitive C-reactive protein (hs-CRP), > 10 mg/L [reference range: < 10 mg/L], and procalcitonin (PCT), > 95 ng/ml [reference range: < 0.5 ng/ml]. The head CT scan showed brain atrophy. The chest CT scan revealed bilateral pulmonary nodules, with the larger nodule measuring approximately 7*5 mm. There was minimal pleural effusion bilaterally. The abdominal CT scan indicated a round-shaped slightly hypodense lesion with a diameter of approximately 46 mm at the top of the right lobe of the liver, possibly a liver abscess. Because these CT scans were performed at another hospital, we only have textual reports and do not have images. The main diagnoses were sepsis, acute respiratory distress syndrome, and liver abscess at the local hospital. The patient received non-invasive mechanical ventilation and was treated with imipenem-cilastatin. Due to the worsening of the patient’s condition and progressive alteration of consciousness, he was transferred to our hospital. Endotracheal intubation was performed in the emergency department of our hospital, and the patient was admitted to the intensive care unit. The patient’s conscious state was coma, with a Glasgow Coma Scale (GCS) score of 5. Auscultation of the chest revealed moist rales and no pain expression when pressing the abdomen. Meningeal irritation signs and pathological signs were negative.
After admission, the patient received invasive mechanical ventilation, sedation, and analgesia. Laboratory results showed WBC, 16.75 *10^9/L; neutrophil ratio, 90.1%; PLT, 54 *10^9/L; hs-CRP, 268.48 mg/L; PCT, > 95 ng/mL; aspartate aminotransferase (AST), 169 U/L [reference range: 0–50 IU/L]; alanine aminotransferase (ALT), 86 U/L [reference range: 0–50 IU/L]; venous blood glucose, 29.02 mmol/L [reference range: 3.9–6.1 mmol/L]; creatinine, 142 µmol/L [reference range: 45–84 µmol/L]; and urea nitrogen, 10.48 mmol/L [reference range: 2.1–7.2 mmol/L] (Table 1). Color Doppler ultrasound indicated a mixed echogenic mass of 4.4*4.8 cm in segment 8 of the liver, which was considered an abscess. Due to incomplete liquefaction of the liver abscess, drainage was not performed at this time. Clinical pharmacists recommended that the patient continued to use imipenem-cilastatin (1g i.v. q6h, infusion time > 3h). At the same time, he received liver protection, expectoration, nutritional support, and glycemic control. On day 3, the patient developed septic shock, and norepinephrine was administered to raise his blood pressure. He also developed decreased urine output and acute kidney injury, so continuous renal replacement therapy combined with endotoxin adsorption was given. The patient’s routine blood test showed a very low PLT of 31 *10E9/L (Table 1), and percutaneous catheter drainage was intended, so 1 unit of platelets was transfused. On day 7, the patient’s WBC increased to 34.79 *10^9/L, neutrophil ratio was 80.4%, and hs-CRP was 97.85 mg/L (Table 1). His activated partial thromboplastin time was 162.8s, and 400ml of fresh frozen plasma was transfused. The (1,3)-beta-d-glucan antigen test result was 137.5pg/ml [reference range: 0–70 pg/ml]. Galactomannan test result was normal. Metagenomic next-generation sequencing in bronchoalveolar lavage fluid indicated K. pneumoniae, Candida albicans, and Aspergillus flavus complex, and no viruses were detected. Blood culture results showed K. pneumoniae (extended-spectrum β-lactamase negative, sensitive to piperacillin/tazobactam, tetracyclines, macrolides, cephalosporins, aminoglycosides, quinolones, carbapenems; resistant to ampicillin and ticacillin). Considering that the patient had developed acute kidney injury, the antibiotic was adjusted to piperacillin/tazobactam (4.5g i.v. q8h) combined with voriconazole (200mg i.v. q12h, 300mg i.v. q12h on the first day). Color Doppler ultrasonography showed that the liver abscess turned into a mixed sac mass of 6.4 × 5.3 cm. He underwent ultrasound-guided percutaneous catheter drainage of the liver abscess. The pus was pale red and was sent for microbial culture. After discontinuation of analgesic and sedative medications, he remained in a coma with a GCS score of 4. The head CT scan showed lacunar cerebral infarction (Fig. 1a). The chest CT showed pneumonia and pulmonary nodules with cavities (Fig. 1b). The abdominal CT scan revealed an abscess in the right lobe of the liver and catheter signs (Fig. 1c). On day 10, pus culture results also showed K. pneumoniae that was sensitive to piperacillin/tazobactam. On day 14, the reexamination of the head CT scan showed no significant changes compared with before (Fig. 2a). The reexamination of the chest CT scan showed that bilateral pneumonia and abscesses were absorbed more than before (Fig. 2b). The reexamination of the abdominal CT scan showed a reduction in the size of the hepatic abscess in the right lobe of the liver compared to previous findings (Fig. 2c). On day 15, there was no liquid extraction from the drainage tube of the liver abscess, and there was no obvious liquid area in the reexamination of color Doppler ultrasound, so the drainage tube was removed. The patient’s lung abscesses and liver abscess were relieved, and the endotracheal tube was removed, but he remained in a coma with a GCS score of 3. On day 21, a cranial MRI showed multiple brain abscesses (Fig. 3a–c). The neurologist recommended a lumbar puncture, but the family refused. The final diagnoses were KPIS, pulmonary fungal infection, multiple organ failure, and sepsis. Finally, the patient’s family gave up and discharged him. The patient died at a local hospital 3 days after being discharged from our hospital.

On day 7, the head CT scan showed hypodense lesions around bilateral frontal lobes, basal ganglia, and lateral ventricles, suggestive of lacunar cerebral infarctions (a). The chest CT scan showed bilateral pulmonary nodules with central cavitation. The largest nodule was located in the right upper lobe and measured approximately 23*17 mm (b). The abdominal CT scan revealed an abscess in the right lobe of the liver, with a maximum cross-section of 33.69*37.21 mm and catheter signs (c)

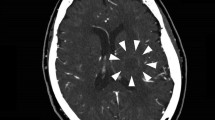
On day 14, the head CT scan showed hypodense lesions, with no apparent changes compared to previous findings (a). The chest CT scan revealed that bilateral pneumonia and abscesses had been absorbed compared to previous findings (b). The abdominal CT scan showed a reduction in the size of the hepatic abscess in the right lobe of the liver compared to previous findings, with the presence of features indicative of a catheter within it (c)

On day 21, the brain magnetic resonance imaging (MRI) revealed widespread plaques or circular abnormal signals within the brain parenchyma. These signals appeared as low intensity on T1-weighted imaging (a), high intensity on T2-weighted imaging (b), and showed restricted diffusion on diffusion-weighted imaging (c)
Discussion
K. pneumoniae is a species of the Enterobacteriaceae family, which is a normal group of bacteria found in the human mouth and intestines. K. pneumoniae includes three subspecies, but usually K. pneumoniae refers to the pneumonia subspecies. The main virulence factors of K. pneumoniae include capsule serotypes (mainly K1 and K2), hypermucoviscosity phenotype (significantly associated with the syndrome of destructive tissue abscess, including liver or other site abscesses), lipopolysaccharide, ferrisomes, and fimi [9, 10]. Hypervirulent K. pneumoniae (hvKp) strains of capsule type K1 and K2 cause invasive infections associated with liver abscesses, which can be difficult to treat and are frequently associated with recurrent infections [11, 12]. Compared with classical K. pneumoniae, hvKp has a different iron acquisition capacity, capsule polysaccharide production, phenotype, and biofilm formation, which contribute to its high invasive infection capability [11]. Primary Klebsiella pneumoniae liver abscess (KLA) refers to a liver abscess caused by K. pneumoniae in the absence of predisposing factors in the abdominal cavity, such as liver and biliary diseases, colorectal diseases, or a history of abdominal surgery or trauma. HvKp is usually the causative agent in these cases [13]. A study of KLA patients in Taiwan, China, showed that 14.1% of K1 strain-infected individuals developed pyogenic endophthalmitis, and 10.5% of K2 strain-infected individuals did so. There were no cases of pyogenic endophthalmitis in non-K1/K2 strain-infected individuals [14]. The infection rate of K. pneumoniae increases in patients with compromised primary defense functions, such as diabetes, alcoholism, malignancy, liver and biliary diseases, chronic obstructive pulmonary disease, corticosteroid therapy, and renal failure. These factors may lead to multiple site infections of K. pneumoniae [15]. When K. pneumoniae causes pulmonary abscess, endophthalmitis, central system infection, necrotic fasciitis, and other multi-site infections, it is clinically referred to as KPIS [16]. A study has shown that the incidence of KPIS caused by hvKp is approximately 12% [10]. Hypermucoviscosity phenotype is present in 98% of invasive strains, and string testing may be one of the screening methods for hvKp. However, it should be noted that 17% of the non-invasive strains also had a hypermucoviscosity phenotype [17].
Diabetes is also an important risk factor for KPIS [18]. The reasons for this are mainly as follows: (1) Elevated blood glucose levels can inhibit the cell activity of CD4, CD8, and NK cells, as well as the production of cytokines, leading to immune dysfunction. In diabetic patients, the initial symptoms of infectious diseases may not be apparent, resulting in delayed treatment [19]. (2) Hyperglycemia inhibits the adhesion, chemotaxis, and phagocytic functions of neutrophils, making infections difficult to control [20]. (3) In diabetic patients, increased blood glucose leads to peripheral vascular disease, increased permeability of the blood vessel wall, and decreased blood oxygen content in the surrounding tissues. These factors provide favorable conditions for bacterial growth and proliferation [21]. Therefore, diabetic patients infected with K. pneumoniae are prone to hematogenous dissemination, leading to multiple abscesses in locations such as the intracranial region, lungs, and liver. Strict blood glucose control can prevent the occurrence of metastatic complications, while poor blood glucose control can result in a worse prognosis for patients with KPIS [22,23,24]. In the majority of critically ill and noncritically ill patients, the target blood glucose control range was 140–180 mg/dL (7.8–10.0 mmol/L). Achieving this goal requires the use of intravenous insulin when the blood glucose level is ≥ 180 mg/dL (10.0 mmol/L) [25]. In the present case, significantly elevated glycosylated hemoglobin upon admission indicated poor recent blood glucose control, which is one of the reasons for the occurrence of KPIS and the poor prognosis of the patient.
For patients with diabetes, especially those with poor blood glucose control, comprehensive examinations should be conducted if KLA occurs. These include chest and abdominal CT scans, as well as cranial MRI, to screen for all possible infection sites. In this case, the patient presented with impaired consciousness, and the head CT scan revealed hypodense lesions. Although the imaging findings lacked specificity, it is still important to remain vigilant for the possibility of intracranial infection. However, at that time, the patient had been intubated and had been undergoing invasive mechanical ventilation, so it was not possible to complete the cranial MRI. It is undeniable that we did not have sufficient awareness of the possibility of brain abscess. These factors contributed to the delayed diagnosis of brain abscess in the patient. Additionally, the patient also had a concurrent fungal infection in the lungs, leading to a very poor prognosis.
The bronchoalveolar lavage fluid, blood, and pus cultures all showed K. pneumoniae. After admission, the patient was initially treated with imipenem-cilastatin for anti-infection therapy. Based on the drug sensitivity test and renal function, the antibiotic was switched to piperacillin/tazobactam. Follow-up examinations showed a decrease in infection markers such as WBC, CRP, and PCT. The repeat chest CT scan showed improved absorption of pneumonia, with a reduction in lung nodules and cavities. The repeat abdominal CT scan indicated improvement of the liver abscess. These findings indicate that treatment with piperacillin/tazobactam effectively targeted the infection caused by K. pneumoniae. However, the concentration of this drug in the intracranial distribution is low, which may explain the improvement in extracranial infection but the development of brain abscesses. For the selection of antibiotics against KLA, cephalosporins are the main ones at present, which can be combined with aminoglycosides. For intracranial infections, it is important to select antibiotics with high concentrations in the cerebrospinal fluid. The preferred drugs are third-generation cephalosporins, such as ceftriaxone and cefotaxime. In cases where the strain is suspected to produce broad-spectrum β-lactamases, imipenem and meropenem can be administered [24]. Research by Zhang et al. suggests that meropenem is recommended as the first-line treatment for patients with severe infections at multiple sites. However, the duration of antibiotic therapy should be determined based on laboratory and imaging results [2]. For elderly patients, those with diabetes, those with resistance to piperacillin/tazobactam or cefotaxime, patients admitted to the intensive care unit, and other high-risk patients for infection, when diagnosed with KLA, carbapenems should be the preferred choice for antimicrobial treatment [26].
In conclusion, in patients with hvKp infection or concurrent diabetes, caution should be exercised for the occurrence of KPIS when a lung abscess or liver abscess develops. For patients who may have intracranial infection, early completion of cranial MRI and selection of antibiotics with higher distribution in the cerebrospinal fluid are necessary. At the same time, active treatment of the patient’s complications and nutritional support should be provided.
Availability of data and materials
Not applicable.
References
Webb GJ, Chapman TP, Cadman PJ, Gorard DA. Pyogenic liver abscess. Frontline Gastroenterol. 2014;5(1):60–7.
Zhang CG, Wang Y, Duan M, Zhang XY, Chen XY. Klebsiella pneumoniae invasion syndrome: a case of liver abscess combined with lung abscess, endophthalmitis, and brain abscess. J Int Med Res. 2022;50(3):3000605221084881.
Namikawa H, Oinuma KI, Yamada K, Kaneko Y, Kakeya H, Shuto T. Predictors of hypervirulent Klebsiella pneumoniae infections: a systematic review and meta-analysis. J Hosp Infect. 2023;134:153–60.
Zhao B, Hu R, Gong L, Wang X, Zhu Y, Wu G. Pyogenic liver abscess and endogenous endophthalmitis due to K64-ST1764 hypervirulent Klebsiella pneumoniae: a case report. Infect Drug Resist. 2021;14:71–7.
Sun R, Zhang H, Xu Y, Zhu H, Yu X, Xu J. Klebsiella pneumoniae-related invasive liver abscess syndrome complicated by purulent meningitis: a review of the literature and description of three cases. BMC Infect Dis. 2021;21(1):15.
Chang WN, Huang CR, Lu CH, Chien CC. Adult Klebsiella pneumoniae meningitis in Taiwan: an overview. Acta Neurol Taiwan. 2012;21(2):87–96.
Sun R, Zhang H, Xu Y, Zhu H, Yu X, Xu J. Klebsiella pneumoniae-related invasive liver abscess syndrome complicated by purulent meningitis: a review of the literature and description of three cases. BMC Infect Dis. 2021;21(1):15 Published 2021 Jan 6.
Muthu V, Gogineni RR, Agarwal R, et al. Treatment of pulmonary mucormycosis with adjunctive nebulized amphotericin B (MUCONAB trial): results of an open-label randomized controlled trial. Mycoses. 2023;66(8):688–96.
Wyres KL, Lam MMC, Holt KE. Population genomics of Klebsiella pneumoniae. Nat Rev Microbiol. 2020;18(6):344–59.
Ku YH, Chuang YC, Yu WL. Clinical spectrum and molecular characteristics of Klebsiella pneumoniae causing community-acquired extrahepatic abscess. J Microbiol Immunol Infect. 2008;41(4):311–7.
Zhu J, Wang T, Chen L, Du H. Virulence factors in hypervirulent Klebsiella pneumoniae. Front Microbiol. 2021;12:642484.
Fang CT, Lai SY, Yi WC, Hsueh PR, Liu KL, Chang SC. Klebsiella pneumoniae genotype K1: an emerging pathogen that causes septic ocular or central nervous system complications from pyogenic liver abscess. Clin Infect Dis. 2007;45(3):284–93.
Russo TA, Marr CM. Hypervirulent Klebsiella pneumoniae. Clin Microbiol Rev. 2019;32(3):e00001-19.
Fung CP, Chang FY, Lee SC, et al. A global emerging disease of Klebsiella pneumoniae liver abscess: is serotype K1 an important factor for complicated endophthalmitis? Gut. 2002;50(3):420–4.
Hu Y, Anes J, Devineau S, Fanning S. Klebsiella pneumoniae: prevalence, reservoirs, antimicrobial resistance, pathogenicity, and infection: a hitherto unrecognized zoonotic bacterium. Foodborne Pathog Dis. 2021;18(2):63–84.
Evangelista V, Gonçalves CV, Almeida R, et al. Klebsiella pneumoniae invasive syndrome. Eur J Case Rep Intern Med. 2018;5(3):000800.
Fang CT, Chuang YP, Shun CT, Chang SC, Wang JT. A novel virulence gene in Klebsiella pneumoniae strains causing primary liver abscess and septic metastatic complications. J Exp Med. 2004;199(5):697–705.
Yang CC, Yen CH, Ho MW, Wang JH. Comparison of pyogenic liver abscess caused by non-Klebsiella pneumoniae and Klebsiella pneumoniae. J Microbiol Immunol Infect. 2004;37(3):176–84.
Turk Wensveen T, Gašparini D, Rahelić D, Wensveen FM. Type 2 diabetes and viral infection; cause and effect of disease. Diabetes Res Clin Pract. 2021;172:108637.
Llorente L, De La Fuente H, Richaud-Patin Y, et al. Innate immune response mechanisms in non-insulin dependent diabetes mellitus patients assessed by flow cytoenzymology. Immunol Lett. 2000;74(3):239–44.
Zhang CG, Duan M, Zhang XY, et al. Klebsiella pneumoniae infection secondary to spontaneous renal rupture that presents only as fever: a case report. World J Clin Cases. 2021;9:2602–10.
Liao WI, Sheu WH, Chang WC, Hsu CW, Chen YL, Tsai SH. An elevated gap between admission and A1C-derived average glucose levels is associated with adverse outcomes in diabetic patients with pyogenic liver abscess. PLoS One. 2013;8(5):e64476.
Zhang S, Zhang X, Wu Q, et al. Clinical, microbiological, and molecular epidemiological characteristics of Klebsiella pneumoniae-induced pyogenic liver abscess in southeastern China. Antimicrob Resist Infect Control. 2019;8:166.
Siu LK, Yeh KM, Lin JC, Fung CP, Chang FY. Klebsiella pneumoniae liver abscess: a new invasive syndrome. Lancet Infect Dis. 2012;12(11):881–7.
American Diabetes Association Professional Practice Committee. 16. Diabetes care in the hospital: standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S244–53.
He S, Yu J, Wang H, Wang L, Chen Y, Zhou W. Association of blood culture with carbapenem use in pyogenic liver abscess: a two-center retrospective study. BMC Emerg Med. 2021;21(1):58.
Acknowledgements
Grammar consulting and writing assistance were kindly provided by Ying Liu.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
YL and WH were major contributors to the conception, design, writing, and literature review. LW and SD were involved in editing the manuscript. XZ supervised and reviewed the manuscript. All the authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This case report was approved by the ethics committee of Chengdu First People’s Hospital. All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee(s) and with the Helsinki Declaration (as revised in 2013). Written informed consent was obtained from the patient’s guardian.
Consent for publication
Informed written consent was obtained from the patient’s guardian for publication of this report and any accompanying images.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Luo, Y., Hu, W., Wu, L. et al. Klebsiella pneumoniae invasive syndrome with liver, lung, and brain abscesses complicated with pulmonary fungal infection: a case report and review of the literature. Int J Emerg Med 16, 92 (2023). https://doi.org/10.1186/s12245-023-00574-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12245-023-00574-1