
Abstract
Background
E-cigarette use, or vaping, is an alternative nicotine delivery system that is becoming increasingly prevalent in adolescents and young adults. There is currently a lack of comprehensive research on the adverse effects of vaping on the upper airway.
Acute epiglottitis is a potentially life-threatening condition that can lead to airway obstruction. It is commonly caused by bacterial infections such as streptococci, staphylococcus, and Moraxella. Adult patients with acute epiglottitis mainly present with odynophagia, dysphagia, and respiratory difficulties. The diagnosis of epiglottitis is made by direct laryngoscopy, and the mainstay of treatment is antibiotics.
Bozella et al. (2020) reported a case of subacute non-infectious epiglottitis associated with e-cigarette use in a pediatric patient (Pediatrics 145(3), 2020). Here we present a case of acute epiglottitis in a healthy young adult after vaping, with a negative infectious workup. To our knowledge, there has been no such reported case of epiglottitis associated with e-cigarette use in an adult patient.
Case description
A previously healthy 29-year-old male with daily e-cigarette use presented to the emergency department with a severe sore throat, dysphagia, mild hoarseness, and shortness of breath, especially when lying supine. A lateral neck soft tissue radiograph revealed a thickened epiglottis with a thumb sign. Direct bedside laryngoscopy showed a swollen epiglottis, partially obstructing the supraglottic region confirming the diagnosis of acute epiglottitis. Throat and nasal swabs were negative for streptococcus and COVID-19 infection, respectively. The patient’s condition improved significantly after receiving intravenous Dexamethasone and antibiotics for 2 days. Repeat laryngoscopy showed the resolution of epiglottis swelling, and subjective symptoms had resolved entirely 2 weeks following the start of the treatment.
Conclusions
Although bacterial infections usually cause acute epiglottitis, this case presents the second report of this condition associated with vaping with negative microbiological investigations. Therefore, we recommend that physicians consider non-infectious causes such as vaping in their differential diagnosis for patients with acute and subacute epiglottitis. More research is warranted on the utility of antibiotics in treating vaping-induced epiglottitis.
Similar content being viewed by others


Introduction
Electronic cigarette (e-cigarette) use or vaping is an alternative nicotine delivery system that has been promoted as a safer option to conventional smoking. E-cigarettes can be purchased prefilled or as reusable cartilages containing a mixture of flavours and various concentrations of nicotine, making them accessible and popular among teenagers and young adults. In 2018, it was estimated that 13 million Americans were active e-cigarette users [1]. There have been several reports of developing vaping-associated lung injury and atypical pneumonia in e-cigarette users [2,3,4,5], promoting researchers focusing on the adverse effects of vaping on the respiratory system. However, there is still a lack of comprehensive understanding of the effects of vaping on the upper respiratory tract.
E-cigarette smoking produces a vaporized liquid that passes through the pharynx, larynx, and vocal cords before reaching the lungs. This aerosol adheres to upper airway surfaces and can pose physiological changes to oropharyngeal health. In a recent in-vitro study, Lungova et al. showed epithelial erosion and disruption of the innate immune response 1 week after exposure to e-cigarette vapour extract. They further demonstrated epithelial and basal cell hyperplasia and membrane thickening [6].
Here we present a case of acute epiglottitis in an otherwise healthy young adult who was an active e-cigarette user. Considering the increasing prevalence of e-cigarette use in teenagers and young adults, we aim to highlight some of the unknown health risks associated with vaping. Further, we propose that primary practitioners and emergency physicians consider acute epiglottitis in their differential diagnosis for active e-cigarette users with acute or subacute dysphagia and odynophagia.
Case presentation
A previously healthy 29-year-old male with no medical history of respiratory illness, recurrent throat infections, or hospital admissions presented to the emergency department with a 3-day history of progressively worsening sore throat, odynophagia, and dysphagia. On presentation day, he started experiencing mild hoarseness and shortness of breath, especially when lying supine, which prompted seeking medical attention. On further questioning, the patient was not taking any prescribed medications and had no known drug allergies. He reported continuous e-cigarette use starting 2 days prior to the development of symptoms, minimal alcohol intake, and no use of recreational drugs.
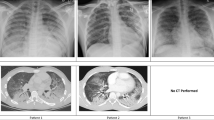
The patient received intravenous Dexamethasone In the emergency department, which immediately improved his shortness of breath. A throat culture was negative for group A, B, and C Streptococcus. COVID-19 was ruled out with a PCR nasal swab. The total peripheral white blood cell count was mildly elevated, but the rest of the renal and metabolic panels were normal. A lateral soft tissue radiograph of the neck showed a poorly defined and thickened epiglottis with a classic thumb sign, indicating acute epiglottitis (Fig. 1).

Lateral neck soft tissue radiograph: poorly defined and thickened epiglottis. The arrow points to the thumb sign which is commonly associated with acute epiglottitis
Considering his respiratory concerns, the Otolaryngology team was consulted. On examination, the patient was afebrile and was not experiencing trismus or stridor. Direct bedside laryngoscopy showed an enlarged, erythematous, and swollen epiglottis, partially obstructing the supraglottic region (Fig. 2a). Arytenoids were noted to be edematous bilaterally with normal vocal cord mobility.

Direct laryngoscope examination of the epiglottis. A On initial presentation: the epiglottis appears swollen, erythematous, and is occluding the supraglottic region. B Post-therapy: normal appearing glottis, epiglottis, and larynx
The patient was admitted to the hospital for airway monitoring and was started on intravenous Ceftriaxone and oral Metronidazole. He was also given another dose of intravenous Dexamethasone and was asked to stop using his e-cigarette.
The patient’s condition improved significantly after 2 days, and a repeat laryngoscopy showed resolution of the swelling in the epiglottis (Fig. 2b). The patient was switched to oral Amoxicillin for 10 days and was discharged from the hospital.
Discussion and conclusions
Acute epiglottitis is a potentially life-threatening condition, often associated with an infection, which can lead to airway obstruction. It was historically considered a pediatric disease caused by Haemophilus influenza infection, but the incidence has dramatically declined in pediatrics after the introduction of the conjugate vaccines. There have been reports of a shift in etiology and epidemiology towards younger adults. Other more common etiologies are streptococci, staphylococcus, and Moraxella infections.
Adult patients with acute epiglottitis mainly present with odynophagia, dysphagia, drooling, and respiratory difficulties [7]. Direct laryngoscopy often shows a swollen, inflamed epiglottis, and soft tissue neck radiographs can often confirm an enlarged epiglottis [7, 8]. Acute epiglottitis is a clinical diagnosis, and direct visualization of the epiglottis remains the gold standard for diagnosis [9]. The mainstay of epiglottitis management is rapid airway assessment and maintenance, supplemental oxygen, and empirical antibiotic therapy [10]. Bronchodilators and parenteral glucocorticoids have also been suggested as additional therapies in severe cases [11].
E-cigarettes or vape pens are marketed as a healthier alternative to conventional smoking tobacco products. E-cigarette users can adjust the amount of nicotine delivered by each device; therefore, they can sometimes be used as an aid for smoking cessation and relieving withdrawal symptoms [12]. E-cigarettes are becoming increasingly prevalent in the adolescent and young adult population [13]. In recent years, a growing body of evidence has described the adverse effects and toxicity of e-cigarette use. In addition, there has been a report of microbial contamination in the E-cigarettes sold in the USA [14].
The biological and physiological effects of e-cigarettes on the oropharyngeal mucosa have been recently investigated. The oxidative stress causes increased production of inflammatory cytokines and decreased activity of innate immune cells [15]. Oral mucosal lesions such as hairy tongue and nicotine stomatitis are also more prevalent in e-cigarette users [16].
Bozella et al. (2020) reported a case of non-infectious acute epiglottitis in an adolescent female patient [17]. Similar to our case, the patient had presented to the emergency department with severe dysphagia and acute respiratory distress. However, their patient’s condition was more severe, and she needed a prolonged admission to the hospital and was treated with systemic antibiotics and Dexamethasone. After ruling out infectious etiologies, they hypothesized a direct chemical and thermal injury from vaping as the main cause of her epiglottitis.
This case presents the second report of acute epiglottitis directly associated with e-cigarettes with no evidence of infection. We cannot completely rule out the possibility of an infectious cause, and patients in both cases were treated with antibiotics. However, we also speculate that a primary direct thermal injury from the vaporized liquid promoted an inflammatory reaction in the supraglottic region, causing oxidative stress and epiglottis swelling. In addition, the oxidative stress causes increased viral replication and decreased antimicrobial activity of neutrophils and macrophages, resulting in immunosuppression and likely a secondary infection [15]. Moreover, antimicrobial and heavy metal contamination in the vape product could also play a role in producing this inflammatory reaction [14]. We recommend that physicians consider non-infectious primary causes such as vaping in their differential diagnosis for patients with acute and subacute epiglottitis. Future research is warranted on the utility of antibiotics in treating such patients with negative infectious workup.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Abbreviations
- E-cigarettes:
-
Electronic cigarettes
References
Sosnowski TR, Odziomek M. Particle size dynamics: toward a better understanding of electronic cigarette aerosol interactions with the respiratory system. Front Physiol. 2018;9:853.
Cherian SV, Kumar A, Estrada-Y-Martin RM. E-cigarette or vaping product-associated lung injury: a review. Am J Med. 2020;133(6):657–63.
Kalininskiy A, Bach CT, Nacca NE, Ginsberg G, Marraffa J, Navarette KA, McGraw MD, Croft DP. E-cigarette, or vaping, product use associated lung injury (EVALI): case series and diagnostic approach. Lancet Respir Med. 2019;7(12):1017–26.
Triantafyllou GA, Tiberio PJ, Zou RH, Lamberty PE, Lynch MJ, Kreit JW, Gladwin MT, Morris A, Chiarchiaro J. Vaping-associated acute lung injury: a case series. Am J Respir Crit Care Med. 2019;200(11):1430–1.
Salzman GA, Alqawasma M, Asad H. Vaping associated lung injury (EVALI): an explosive United States epidemic. Missouri Med. 2019;116(6):492.
Lungova V, Wendt K, Thibeault SL. Exposure to e-cigarette vapor extract induces vocal fold epithelial injury and triggers intense mucosal remodeling. Dis Models Mech. 2022;15(8):dmm049476.
Guldfred LA, Lyhne D, Becker BC. Acute epiglottitis: epidemiology, clinical presentation, management and outcome. J Laryngol Otol. 2008;122(8):818–23.
Mayo-Smith MF, Spinale JW, Schiffman FJ, Donskey CJ, Yukawa M, Li RH. Acute epiglottitis: an 18-year experience in Rhode Island. Chest. 1995;108(6):1640–7.
Solomon P, Weisbrod M, Irish JC, Gullane PJ. Audit epiglottitis: The Toronto hospital experience. J Otolaryngol Head Neck Surg. 1998;27(6):332.
Shah RK, Roberson DW, Jones DT. Epiglottitis in the Hemophilus influenzae type B vaccine era: changing trends. Laryngoscope. 2004;114(3):557–60.
Glynn F, Fenton JE. Diagnosis and management of supraglottitis (epiglottitis). Curr Infect Dis Rep. 2008;10(3):200–4.
Gualano MR, Passi S, Bert F, La Torre G, Scaioli G, Siliquini R. Electronic cigarettes: assessing the efficacy and the adverse effects through a systematic review of published studies. J Public Health. 2015;37(3):488–97.
Walley SC, Wilson KM, Winickoff JP, Groner J. A public health crisis: electronic cigarettes, vape, and JUUL. Pediatrics. 2019;143(6).
Lee MS, Allen JG, Christiani DC. Endotoxin and (1→ 3)-β-D-glucan contamination in electronic cigarette products sold in the United States. Environ Health Perspect. 2019;127(4): 047008.
Scott A, Lugg ST, Aldridge K, Lewis KE, Bowden A, Mahida RY, Grudzinska FS, Dosanjh D, Parekh D, Foronjy R, Sapey E. Pro-inflammatory effects of e-cigarette vapour condensate on human alveolar macrophages. Thorax. 2018;73(12):1161–9.
Bardellini E, Amadori F, Conti G, Majorana A. Oral mucosal lesions in electronic cigarettes consumers versus former smokers. Acta Odontologica Scandinavica. 2018;76(3):226–8.
Bozzella MJ, Magyar M, DeBiasi RL, Ferrer K (2020) Epiglottitis associated with intermittent E-cigarette use: the vagaries of Vaping toxicity. Pediatrics. 145(3).
Acknowledgements
Not applicable.
Funding
This study was conducted without any funding from any grant or commercial interest.
Author information
Authors and Affiliations
Contributions
A.K. performed literature review, drafted, and edited the manuscript. MA.K edited the manuscript according to the reviewer’s comments. H.G. collected and interpreted patient data regarding the inflammatory condition as well as supervision, reviewing and editing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee(s) and with the Helsinki Declaration (as revised in 2013). Ethics board approval was not required for this case report as per University of British Columbia ethics review board. Written informed consent was obtained from all the participants in this study.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the editorial office of this journal.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Khorrami, A., Khorrami, M.A. & Gheriani, H. Vaping-induced acute epiglottitis: a case report. Int J Emerg Med 16, 56 (2023). https://doi.org/10.1186/s12245-023-00532-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12245-023-00532-x