
Abstract
Objective
To compare laparoscopic hysterectomy (LH) with total abdominal hysterectomy (TAH) regarding different outcome measures at our tertiary hospital.
Study design
This retrospective comparative cross-sectional study was conducted at the Department of Obstetrics and Gynecology Department, Women’s Hospital, Hamad Medical Corporation, Doha, Qatar. It included 44 patients who had LH (group 1) and 95 patients who had TAH (group 2) during the period from January 2009 through June 2014.
Results
Three patients were converted from LH to TAH and were excluded from the final analysis. The size of the uterus was smaller in the LH group than the TAH group (7.38 ± 1.92 vs 10.25 ± 3.84 cm, respectively; p < 0.0005). The operative time was shorter in TAH than in LH (2.22 ± 0.93 vs 2.43 ± 0.94, respectively; p = NS). The blood loss was less in the LH group than the TAH group (258.54 ± 65.26 vs 370.32 ± 74.8, respectively; p = NS). There were no significant differences between both groups regarding rates intraoperative and early postoperative complications; however, late postoperative complications were significantly higher in the TAH group (p < 0.05). The length of hospital stay was shorter with LH than TAH (3.63 ± 1.28 vs 5.22 ± 4 days, respectively; p < 0.001)
Conclusion
LH compares to TAH in terms of duration of surgery, rates of intraoperative and early postoperative complications, and the need for blood transfusion. However, it has significantly less rate of late postoperative complications and length of hospital stay.
Similar content being viewed by others


Introduction
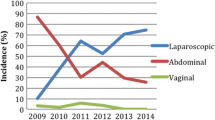
Over 430,000 hysterectomies were performed in the USA in 2010, making it the most common gynecological surgical operation. Between 1998 and 2010, the distribution of the surgical approach was 65% abdominal, 20% vaginal, 13% laparoscopic, 0.9% robotic, and 1.2% had a radical hysterectomy. 2002 was the peak year for hysterectomy, after that there was a decline in the rates of hysterectomy due to approaches of utilizing less invasive alternatives to hysterectomy [1].
Most studies comparing abdominal and vaginal routes of hysterectomy have concluded that the vaginal approach should be the preferred route as it is associated with less complication rates, shorter hospital stay, and lower cost compared to the abdominal route [2,3,4]. However, the indication and complexity of the procedure can influence the route of surgery; thus, data from observational studies must be interpreted with caution.
Recent developments of minimally invasive surgery (MIS) in gynecologic surgery have expanded the laparoscopic route of hysterectomy. Less invasive procedures, when possible, are typically preferable to more invasive procedures [5], and in general, a surgeon should choose the procedure which best achieves the goal of surgery and at the same time maximizes patient safety. A statement from the American College of Obstetricians and Gynecologists (ACOG) advises surgeons to use a vaginal approach whenever possible, and for patients in whom vaginal hysterectomy is not feasible or indicated, laparoscopic hysterectomy should be performed over open abdominal hysterectomy. In all cases, the choice of the route of hysterectomy should take into account the clinical factors and surgeon’s experience to maximize patient’s safety and optimize outcomes [6]. The aim of this study was to compare laparoscopic hysterectomy (LH) with total abdominal hysterectomy (TAH) regarding different outcome measures at our tertiary hospital.
Patients and methods
This retrospective comparative cross-sectional study included 44 patients who underwent LH with or without salpingo-oophorectomy at the Department of Obstetrics and Gynecology, Women’s Hospital, Hamad Medical Corporation, Doha, Qatar, from January 2009 through June 2014. They were compared to 95 patients who had TAH with or without salpingo-oophorectomy during the same period. The study was approved by the local research and ethics committee at Hamad Medical Corporation (#14362/14). The medical records of the studied cases were reviewed. The study included all cases that undergone hysterectomies for different gynecological indications whether via laparoscopy or laparotomy. Patients that had hysterectomies due to advanced gynecological malignancy, intractable procidentia, and complications of childbirth such as uterine rupture or intractable hemorrhage were excluded from this study.
The hospital records were retrospectively studied for age, body mass index (BMI), parity, indication for surgery, medical co-morbidities, previous operations, size of the uterus (confirmed by either ultrasound or magnetic resonant imaging (MRI)), operative bleeding/estimated blood loss (EBL), pre- and post-operative hemoglobin (HB) level, operative time (time from the first incision to the last stitch), hospital stay, need for postoperative analgesia, the need for blood transfusion, early (occurring within 30 days of surgery) and late (occurring after 30 days of surgery) postoperative complications, and the conversion rate from laparoscopy to laparotomy.
Group 1 included 44 cases that had LH (27 (61.4%) had LAVH [laparoscopically assisted vaginal hysterectomy] and 17 (38.4%) had TLH [total laparoscopic hysterectomy]), and group 2 included 95 cases that had TAH. All surgeries were performed by senior gynecologists. In all cases, the vaginal cuff was closed using polyglactin 910 suture. All uteri in the LH group were removed through the vagina, there were no cases that had subtotal LH, and morcellation was not used. The outcome in both laparotomy and laparoscopy groups was reviewed regarding the hospital stay, operating time, estimated blood loss, pain scale, and complications.
Statistical analysis was performed using Student’s t test and X2 test where appropriate. P < 0.05 was considered statistically significant with < 0.001 as highly significant. Statistical analysis was performed on the SPSS Advanced Statistical Software Version 10 (SPSS, Inc., Chicago, USA).
Results
In the present study, a total of 139 cases were recruited, divided into 2 groups; group 1 including 44 LH cases and group 2 including 95 TAH cases, from January 2009 till June 2014. Only 3 out of 44 cases of LH were converted to TAH due to severe adhesions from prior surgeries, and they were excluded from the final analysis.
There were no statistical significant differences in the age, parity, BMI, or preoperative hemoglobin level between both groups. However, the size of the uterus was significantly smaller in the LH group than the TAH group (7.38 ± 1.92 vs 10.25 ± 3.84 cm, respectively; p < 0.0005) (Table 1).
As shown in Table 2, the commonest indications for surgery in group 1 were endometrial hyperplasia (43.9%), fibroids (24.4%, CIN (17%), and abnormal uterine bleeding (9.8%). While in group 2, the commonest indications were fibroids (62%), abnormal uterine bleeding (18.9%), endometrial hyperplasia (6.3%), and endometriosis (5.2%).
Table 3 shows that the operative time was shorter in TAH than in LH (2.22 ± 0.93 vs 2.43 ± 0.94, respectively), but it was not statistically significant. There was no statistical significant difference in the EBL, but the LH group had less blood loss (mean 258.54 ml) compared to TAH (mean 370.32). TAH had less intraoperative complications than LH, with less bleeding, and bladder injury, but more vaginal laceration; however, these differences were not statistically significant.
The length of hospital stay was significantly shorter in the LH group than the TAH group (3.63 ± 1.28 vs 5.22 ± 4.00 days, respectively; p < 0.001). Likewise, the rate of late postoperative complications was significantly less with LH than with TAH (p < 0.05). However, there were no significant differences between both groups regarding the need for blood transfusion, the use of antibiotics, postoperative HB level, rate of early postoperative complications, and the need for postoperative analgesia (Table 4).
Discussion
As laparoscopic and vaginal hysterectomies have the advantages of lower morbidity, rapid recovery, and shorter hospital stay, there has been a recent trend away from abdominal hysterectomy [7]. The choice between LH and TAH depends on the underlying pathology and the surgeon’s skills/preferences.
The current study showed that both LH and TAH groups were matching regarding age, parity, BMI, and preoperative hemoglobin level; however, the size of the uterus was significantly smaller in the LH group compared to the TAH group (7.38 ± 1.92 vs 10.25 ± 3.84 cm, respectively; p < 0.0005). This could be attributed to selection bias by the surgeons, as most gynecologists would prefer performing LH on small uteri and those with larger uterine size will be more likely to have their hysterectomies performed through laparotomy.
In the present study, the commonest indications for surgery in the LH group were endometrial hyperplasia (43.9%), fibroids (24.4%), CIN (17%), and abnormal uterine bleeding (9.8%). While in the TAH group, the commonest indications were fibroids (62%), abnormal uterine bleeding (18.9%), endometrial hyperplasia (6.3%), and endometriosis (5.2%). These results match many previous reports [8, 9]. These results, as quoted from Nambiar et al. [10], show that “the trends in indication for hysterectomy have remained the same over the past two decades irrespective of the type of population.”
As was shown in the current study, the average operating times were (2.43 ± 0.94 h) for LH compared to (2.22 ± 0.93 h) for TAH; however, it was not statistically significant. Balci [7] and Garry [11] reported a longer operative time with laparoscopic hysterectomy than abdominal hysterectomy. On the other hand, Kongwattanakul and Khampitak [12] reported that the operative time in the LH group was shorter than the TAH group, although this difference was not statistically significant, which may be attributed to the small number of case (60 cases) in their cohort, and/or more experienced gynecologists performing the surgeries, and also the technology used for hemostasis/cutting could be a factor.
Our results showed that LH compared to TAH carried less operative blood loss (258.54 ± 265.26 vs 370.32 ± 74.8 mL, respectively; p = NS), going with Kongwattanakul and Khampitak [12] who reported similar results. The relatively less amount of blood loss with LH in our study could be explained by the surgeons’ expertise, and also, patients in the LH group had smaller sized uteri making surgery much easier, thus minimizing the intra-operative blood loss.
In our study, analgesia requirements were measured by the amount of use of both injectable and oral pain medications. 43.9% of patients in the LH group needed post-operative analgesics compared to 54.7% in the TAH group, which was similar to the results of Marana et al. [13] and Nambiar et al. [10] who reported that abdominally operated women needed more pain medications than laparoscopically operated women.
In our report, the length of hospital stay was significantly shorter with LH than TAH (3.63 ± 1.28 vs 5.22 ± 4 days, respectively; p < 0.001). Other studies have reported similar results [6, 7, 11].
The rate of intraoperative bleeding, hematoma formation, wound infection, urinary tract infection (UTI), and bladder injury was higher in TAH group compared to LH group, in contrast to vaginal vault laceration and post-operative fever that were higher in LH compared to TAH; however, these differences were statistically non-significant. Higher rates of UTI in the TAH group could be caused by the need for prolonged catheterization, and increased rates of postoperative fever following LH can be attributed to upper respiratory tract infection following endotracheal intubation [10]. There was no significant difference between both groups in mean BMI, with patients in the LH group having a mean ± SD BMI of 34.47 ± 7.42 compared to 32.17 ± 6.85 in the TAH group. Despite the higher BMI in the LH group, the rate of late postoperative complications was significantly less than the TAH group with no difference in the early postoperative complications. These results match those of Tinelli et al. [14] who reported that LH is safe and improves the quality of life in the postoperative period in morbidly obese patients. Vaginal cuff dehiscence is a rare complication of hysterectomy with a reported incidence of 0.39%, and the rate is higher after laparoscopic rather than abdominal or vaginal hysterectomy [15, 16]. This could be attributed to the use of energy source to perform the colpotomy incision during LH, thus causing tissue necrosis and poor healing. Also, laparoscopic magnification may lead to failure to achieve full-thickness closure of the cuff and poor knot tying technique are potential causes [17]. There were no reported cases of vaginal cuff dehiscence in any of the study groups.
One of the main concerns with LH is the presence of unexpected sarcoma at the time of hysterectomy for presumed benign indication. The risk of dissemination of sarcoma increases with the use of power morcellation; this prompted the US Food and Drug Administration in 2014 to issue a black box warning against the use of power morcellator for the treatment of uterine fibroids resulting in new guidelines for the use of electromechanical morcellators and a subsequent decrease in their use [18,19,20,21,22,23]. Morcellation was not used in the present study. There were no reported cases of uterine sarcoma after the surgery. These results match those of Multinu et al. [24] who reported a 0.13% incidence of unexpected sarcoma (5 per 3759 hysterectomies for presumed benign indication [95% confidence interval, 0.04–0.31%]).
The limitations of the present study include its retrospective design, relatively small number of patients, and disparity in the number of patients between both LH and TAH groups.
Conclusion
The present study concluded that LH is associated with less hospital stay, less blood loss, less use of analgesics, and fewer intraoperative and postoperative complications when compared to TAH, which makes it a better approach than total abdominal hysterectomy in selected groups of patients.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request. All data generated or analyzed during this study are included in this published article.
References
Wright JD, Herzog TJ, Tsui J, Ananth CV, Lewin SN, Lu YS, Neugut AI, Hershman DL (2013) Nationwide trends in the performance of inpatient hysterectomy in the United States. Obstet Gynecol 122:233–241. https://doi.org/10.1097/AOG.0b013e318299a6cf
Kovac SR (2000) Hysterectomy outcomes in patients with similar indications. Obstet Gynecol 95:787–793
Nieboer TE, Johnson N, Lethaby A, Tavender E, Curr E, Garry R, van Voorst S, Mol BW, Kluivers KB (2009) Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev 8(3):CD003677. https://doi.org/10.1002/14651858.CD003677.pub4
Mäkinen J, Johansson J, Tomás C, Tomás E, Heinonen PK, Laatikainen T, Kauko M, Heikkinen AM, Sjöberg J (2001) Morbidity of 10 110 hysterectomies by type of approach. Hum Reprod 16:1473–1478
Jonsdottir GM, Jorgensen S, Cohen SL, Wright KN, Shah NT, Chavan N, Einarsson JI (2011) Increasing minimally invasive hysterectomy: effect on cost and complications. Obstet Gynecol 117:1142. https://doi.org/10.1097/AOG.0b013e3182166055
American College of Obstetricians and Gynecologists (2017) Choosing the route of hysterectomy for benign disease. ACOG Committee Opinion No. 701. Obstet Gynecol 129:e155–e159. https://doi.org/10.1097/AOG.0000000000002112
Balcı O (2014) Comparison of laparoscopic and abdominal hysterectomy. J Turk Soc Obstet Gynecol 4:224–227
Arbogast JD, Welch RA, Riza ED, Ricaurte EL, Pieper DR (1994) Laparoscopically assisted vaginal hysterectomy appears to be an alternative to total abdominal hysterectomy. Journal of laparoendoscopic surgery 4(3):185–190
Sutasanasuang S (2011) Laparoscopic hysterectomy versus total abdominal hysterectomy: a retrospective comparative study. J Med Assoc Thai 94(1):8–16
KPM N, Supriya K, Thunga S, Kaur S, Karunakaran J (2016) LAVH or TAH – choosing it wise and making it safe. Int J Reprod Contracept Obstet Gynecol 5(3):659–662. https://doi.org/10.18203/2320-1770.ijrcog20160562
Garry R, Fountain J, Mason S, Napp V, Brown J, Hawe J, Clayton R, Abbott J, Phillips G, Whittaker M, Lilford R, Bridgman S (2004) The eVALuate study: two parallel randomised trials, one comparing laparoscopic with abdominal hysterectomy, the other comparing laparoscopic with vaginal hysterectomy. BMJ 328:129–133. https://doi.org/10.1136/bmj.37984.623889
Kongwattanakul K, Khampitak K (2012) Comparison of laparoscopically assisted vaginal hysterectomy and abdominal hysterectomy: a randomized controlled trial. J Minim Invasive Gynecol 19(1):89–94. https://doi.org/10.1016/j.jmig.2011.10.003
Marana R, Busacca M, Zupi E, Garcea N, Paparella P, Catalano GF (1999) Laparoscopically assisted vaginal hysterectomy versus total abdominal hysterectomy: a prospective, randomized, multicenter study. Am J Obstet Gynecol 180:270–275. https://doi.org/10.1016/S0002-9378(99)70199-7
Tinelli R, Litta P, Meir Y, Surico D, Leo L, Fusico A, Angioni S, Cicinelli E (2014) Advantages of laparoscopy versus laparotomy in extremely obese women (BMI > 35) with early-stage endometrial cancer: a multicenter study. Anticancer Res 34(5):2497–2502
Hur HC, Donnellan N, Mansuria S, Barber RE, Guido R, Lee T (2011) Vaginal cuff dehiscence after different modes of hysterectomy. Obstet Gynecol 118:794
Hur HC, Lightfoot M, McMillin MG, Kho KA (2016) Vaginal cuff dehiscence and evisceration: a review of the literature. Curr Opin Obstet Gynecol 28:297
Hur HC (2019) Vaginal cuff dehiscence after hysterectomy. UpToDate
Wright JD, Chen L, Burke WM et al (2016) Trends in use and outcomes of women undergoing hysterectomy with electric power morcellation. JAMA 316:877
Hurd WW (2017) On the road to safer morcellation. Obstet Gynecol 129:976
Ottarsdottir H, Cohen SL, Cox M et al (2017) Trends in mode of hysterectomy after the U.S. Food and Drug Administration power morcellation advisory. Obstet Gynecol 129:1014
Stentz NC, Cooney LG, Sammel M, Shah DK (2017) Changes in myomectomy practice after the U.S. Food and Drug Administration safety communication on power morcellation. Obstet Gynecol 129:1007
Zaritsky E, Tucker LY, Neugebauer R et al (2017) Minimally invasive hysterectomy and power morcellation trends in a West Coast Integrated Health System. Obstet Gynecol 129:996
Redberg RF, Jacoby AF, Sharfstein JM (2017) Power morcellators, postmarketing surveillance, and the US Food and Drug Administration. JAMA 318:325
Multinu F, Casarin J, Tortorella L, Huang Y, Weaver A, Angioni S, Melis GB, Mariani A, Stewart EA, Laughlin-Tommaso SK (2019) Incidence of sarcoma in patients undergoing hysterectomy for benign indications: a population-based study. Am J Obstet Gynecol 220(2):179.e1–179.e10. https://doi.org/10.1016/j.ajog.2018.11.1086.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
MEA conceived the idea, designed the study protocol, and wrote the initial and the final draft of the manuscript. FC collected the data, performed the statistical analysis, and shared in revising the manuscript. AFM shared in data collection and revised the manuscript. All authors agreed for the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the local research and ethics committee at Hamad Medical Corporation (#14362/14).
Consent for publication
Not applicable.
Competing interests
The authors declare they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Aboulfotouh, M.E., Chaalan, F. & Mohammed, A.F. Laparoscopic hysterectomy versus total abdominal hysterectomy: a retrospective study at a tertiary hospital. Gynecol Surg 17, 1 (2020). https://doi.org/10.1186/s10397-020-01068-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s10397-020-01068-1