
Abstract
Background
Glenoid version is an important factor in the evaluation of shoulder stability and shoulder pathologies. However, there are neither established reference values nor known factors that influence the glenoid version, even though valid reference values are needed for diagnostic and orthopaedic surgery like corrective osteotomy and total or reverse shoulder arthroplasty (TSA/RSA). The aim of our population-based study was to identify factors influencing the glenoid version and to establish reference values from a large-scale population cohort.
Results
Our study explored the glenoid versions in a large sample representing the general adult population. We investigated 3004 participants in the population-based Study of Health in Pomerania (SHIP). Glenoid version was measured for both shoulders via magnetic resonance imaging (MRI). Associations with the glenoid version were calculated for sex, age, body height, body weight and BMI. The reference values for glenoid version in the central European population range between −9° and 7.5°, while multiple factors are associated with the glenoid version.
Conclusion
To achieve a reliable interpretation prior to orthopaedic surgery, sex- and age-adjusted reference values are proposed.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
The glenoid version is a frequently used measure to quantify the orientation of the glenoid surface in relation to the scapular body. It is relevant for the diagnostics and treatment of multiple pathologies of the shoulder. Particularly in anterior [1, 2] and posterior [3, 4] shoulder instability and dislocations, the glenoid version is considered an important factor [1]. Eichinger et al. detected a direct effect between glenoid version and the force required for a dislocation [5]. This knowledge is of relevance for total and reverse shoulder arthroplasty (TSA/RSA). In TSA/RSA, accurate positioning of the glenoid component is critical to achieve a good outcome and to prevent poor function, ongoing pain and implant failure [6]. Especially in anatomical arthroplasty, incorrect positioning leads to a high failure rate [7]. Exact knowledge of the physiological glenoid version is crucial, particularly for successful preoperative planning in the treatment of many shoulder pathologies. However, published reference values are mostly based on cadaver studies of scapular bones [8] or small cohorts [9, 10], or they originate from small control groups of hospital-based patients [11].
In 1992, Friedmann et al. described the first measurement of the glenoid version using axial computed tomography (CT) images. Their data suggested that the normal glenoid version is slightly anteverted [11]. In contrast to this, some authors found that a nearly neutral [8, 12] or retroverted glenoid version [9, 13, 14] was normal. Considering the previous publications, the angulation of the glenoid seems to vary in healthy populations. Imhoff et al. were among the first to propose bony corrections of the glenoid version in posterior shoulder instability with a retroversion of > 15° [4]. However, accepted thresholds for resultant therapy have not been defined yet. Therefore, population-based studies are needed to establish reliable reference values.
Additionally, associated factors of the glenoid version are rarely investigated. Possible sex-based differences in glenoid version have been assessed with varying results. Some authors have documented more retroverted glenoids for men [9, 10, 15], while other authors did not find any difference between the sexes [8, 11, 13, 14]. Regarding ethnic differences, Churchill et al. [8] described a significant difference in glenoid version between black and white patients. The influence of the patient’s age is even less well documented. Bouchaib et al. [15] determined that the glenoid version in the upper half of the glenoid decreased with age, while no influence of age was found in the lower half. Concerning side differences, varying results are described. Friedman et al. [11] and Piponov et al. [10] did not find significant differences between the left and right scapulae, whereas several authors found significantly more retroverted glenoids on the dominant side [1, 9, 16]. Associations between body height and body weight and the glenoid version have not been identified to this day [10].
Given the lack of population-based reference values and the limited knowledge of influencing factors for the glenoid version, the aim of this study was to determine reference values based on a representative sample, to determine associations between the glenoid version and sex, age, body weight and body height as well as body mass index (BMI), and to calculate adjusted reference values.
Methods
Design and sample
This study investigated data from 3004 volunteers (mean age 53 years; range 21–90 years) as a project associated with the Study of Health in Pomerania (SHIP) [17]. It is an ongoing population-based study. For a representative sample of the population, participants were recruited randomly from official resident registry office files for a defined region in north-eastern Germany. This sample was randomly selected and stratified by sex and age to resemble the general population of Germany.
The examinations were performed between 1997 and 2012.
In total, 3317 of 6753 participants underwent the MRI examination, whereof 3051 completed the whole shoulder protocol. Forty-seven of 3051 completed shoulder imaging had to be excluded because of a humeral head fracture in the participant’s history. Overall, the MRIs of 3004 volunteers with an equal sex distribution were eligible for this study. Due to stratification, a sample resembling the diversity of the general population with respect to sportiness, cardiovascular risk factors and secondary diseases like osteoporosis was investigated. Detailed sample characteristics can be found in Table 1.
MRI protocol
Shoulder imaging was performed as part of the standardized whole-body MRI on a 1.5-T MR scanner (Magnetom Avanto; Siemens Medical Systems, Erlangen, Germany) by four trained technicians in a standardized manner.
The glenoid version was acquired on straight axial T1-weighted volume interpolated breath-hold examination sequences using five phased-array surface coils with a repetition time of 3.1 ms, an echo time of 1.1 ms, an 8° flip angle, a field of view of 365 × 450 mm, a 256 × 208 matrix and a bandwidth of 560 Hz/pixel, with a resulting voxel size of 1.8 × 1.8 × 3.0 mm. Additionally, a coronal turbo inversion recovery magnitude sequence with a repetition time of 4891 ms, an echo time of 67 ms, a flip angle of 180° and a voxel size of 2.1 × 1.6 × 5.0 mm was used to asses the correct position of the measurement. All sequences were performed while the participant was lying on their back with the palms of their hands positioned medially. Further details can be found in the SHIP pilot study [18].
Image analysis
All measurements were performed by a trained observer (MF), and the participants were blinded to all clinical information. OsiriX software (PIXMEO, Bern, Switzerland) was used to conduct the measurements.

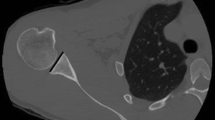
The glenoid version angle (α) is the angle between the glenoid axis and perpendicular line to the scapule axis
The glenoid version was measured according to the original work of Friedman et al. [11]. The glenoid axis was drawn by connecting the anterior and the posterior borders of the glenoid. To form the scapula axis, the medial border of the scapula was marked and connected with the centre of the glenoid (the midpoint of the glenoid axis). The glenoid version angle is the angle between the glenoid axis and a perpendicular line to the scapula axis (Fig. 1).

The positive association between glenoid version and age (p ≤ 0.001)
Statistics
One examiner (MF) measured 25 cases twice to assess the reliability. In addition, another examiner (JL) measured those cases again. Intrareader and interreader variability were assessed by using Bland–Altman plots.
Descriptive statistics such as mean values, standard deviations (SDs), ranges and percentiles were used to describe the sample. Student’s t-test was used for numerical variables. A p value < 0.05 was considered to be statistically significant. Spearman’s correlation coefficient was determined to calculate the correlation between the left and the right sides.
Associations of age, sex and anthropometric markers with glenoid version were analysed by linear regression models. Fractional polynomials (FP) were tested for potential non-linear associations between age and glenoid version. The dose–response relation was found using FP of up to the second degree, with all possible combinations of powers selected from the set (−2, −1, −0.5, 0, 0.5, 1, 2, 3) and compared using log likelihood to determine the best-fitting model. If none of the FP models fitted the data significantly better than the linear model, linear regression was applied. Stratified by sex, age-specific upper and lower reference limits were calculated using quantile regressions for the 2.5th and the 97.5th percentiles. The statistical analysis was performed using Stata 16.1 (Stata Corp., College Station, TX, USA).
Results
The mean age of the 3,004 participants (52% female) was 52.8 ± 13.8 years. The mean values of body weight, body height and BMI were higher in males than in females. Among the participants, 2,976 were right-handed, 19 were left-handed and 8 were two-handed. One participant did not provide information on his dominant side.
Low intrareader and interreader variabilities of between −0.81% ± 2.59% and 0.55% ± 2.90% (mean difference ± SD) were achieved.
The mean glenoid version for all 6,008 assessed glenoids (left and right sides) was slightly retroverted: −0.6° ± 4.1° (range between −42.5° and 12.7°). Right glenoids were more retroverted (−0.7 ± 4.6) than left glenoids (−0.5 ± 4.4, p = 0.041). Additionally, male participants showed a retroverted glenoid, while female glenoids were slightly anteverted on both sides. Detailed results can be found in Table 2.
The correlation between the right and left glenoid version values was r = 0.65. Additionally, age was positively associated with glenoid version (Fig. 2; p < 0.001), meaning the older the individual, the more anteverted the glenoid. Body height was inversely associated with the glenoid version (Fig. 3; p = 0.049), meaning that the higher the individual, the more retroverted the glenoid. Body weight and BMI were not associated with the glenoid version (p = 0.44 and 0.92, respectively). All factors associated with the glenoid version, and their corresponding 95% confidence intervals, are shown in Table 3.

The negative association between glenoid version and body height (p = 0.049)

Sex- and age-dependent reference values for the glenoid version based on fractional polynomials are shown in terms of the lower limit, median and upper limit. The formulas for women are: \(lower limit = - 6.7231{ }{-}{ }0.0021{\times}\left( {\frac{{{\text{age}}}}{10}} \right)^{3}\) \(median = { }0.6769{ }{-}{ }7.9611{\times}\left( {\frac{{{\text{age}}}}{10}} \right)^{ - 2}\) and \(upper limit = { }7.8189{ }{-}20.7634{\times}\left( {\frac{{{\text{age}}}}{10}} \right)^{ - 2}\). For men, the formulas are: \(lower limit = - 15.587{ } + { }0.0966{\times}{\text{age}}\), \(median = - 3.0613{ } + { }0.0332{\times}{\text{age}}\) and \(upper limit = 4.9738{ } + { }0.0181{\times}{\text{age}}\)
As reference values for the glenoid version were stratified by sex, the female reference range was −6.7° to 7.2°, while the male range was −10.2° to 7.1°. Age- and sex-adjusted reference values as well as the formulas are presented for women and men in Fig. 4.
Discussion
The glenoid version is often used as part of the decision-making process for surgical correction of many pathologies of the shoulder. For men, our study showed a reference range of −10.2° to 7.1° for the glenoid version, with a slightly retroverted mean (−1.5° ± 4.4°), while women had a nearly neutral glenoid version of 0.2° ± 3.6° (reference range: −6.7° to 7.2°). Moreover, associations between the glenoid version and the age and body height were determined. Consequently, age-specific reference values for both sexes were calculated (Fig. 4).
Several cadaveric biomechanical studies have stressed the important role of the glenoid version in contact pressure, load transfer, shear stress, cement stress, micromotions at the interface, and resulting instability and loosening in TSA [7, 19, 20].
Additionally, the glenoid version is an important factor to consider in instability of the shoulder, and it has a direct effect on the force required for dislocation [5]. A surgical procedure of a posterior opening-wedge osteotomy is one option to correct the glenoid version and instability [21]. Early clinical results have shown successful outcomes, while a high rate of degenerative changes was observed postoperatively [22]. Recent studies have shown an excellent correction of the glenoid version after a posterior opening-wedge osteotomy, with a low rate of clinical failure, although small sample sizes were investigated [23,24,25]. In a cadaveric study, Imhoff et al. suggested bony correction of the glenoid version in posterior shoulder instability with retroversion > 15° [4]. There is no consensus on ideal version correction [26, 27]. This stresses the importance of knowledge of the normal glenoid version.
No generally accepted reference ranges for the glenoid version have been published until now. Various mean values ranging between 2° anteversion [11] and 9° retroversion [28] have been described for normal or control groups in recent decades (Table 4).
Churchill et al. [8] found an overall glenoid retroversion of 1.23° upon measuring 172 matched pairs of scapular bones of persons between 20 and 30 years old at the time of death. Because of the wide range (−10.5° to 9.5°), Churchill et al. supported the view that there is high variability of the glenoid version amongst the general population. Due to the different measurement technique used, a direct comparison to our results is challenging. In 2014, Matsumura et al. [9] investigated 410 healthy shoulders in a relatively young cohort (mean age 30.6 ± 5.0 years) of 205 volunteers on bilateral CT scans. They obtained a mean glenoid version of −1° and a range between −9° and 13° following the Friedman technique, as we did. Additionally, the glenoid retroversion was significantly higher in men as well as on the dominant side of the patients, while the glenoid version values correlated well with those on the contralateral side. This corresponds to our findings.
In conclusion, most studies that investigated general populations considered a slight retroversion of 1° and therefore a nearly neutral version of the glenoid to be normal [8,9,10, 16, 29]. Despite the different measurement techniques, smaller sample sizes and differences in age compared to previous studies, our study determined nearly the same mean values, with an average glenoid version of 0.6° retroversion, for a representative cross-section of the central European population.
Various results regarding the differences between men and women are described. Our study detected significantly more retroverted glenoids in men. This supports the results of the latest studies on normal values by Matsumura et al. [9] and Piponov et al. [10] as well as some other publications [12, 30].
Regarding the association with age, we found an increasing glenoid version with increasing age. This contradicts the results of Bouchaib et al. [15]. We are aware that longitudinal data are needed to detect whether our observations result from a change in glenoid version across the lifespan. However, Bouchaib et al. [15] examined only 114 CT arthrographies of a hospital-based sample with four defined age groups. In contrast, our study had a population-based sample size of 6008 MRIs, with an asymptomatic subgroup of 4476 MRIs. Consequently, we assume that reliable population-based values were obtained. Matsen et al. stated that adjusted values for age and sex might be beneficial for arthritic patients [30]. Consequently, age- and sex-adjusted reference values were generated (Fig. 4).
A high correlation between right and left glenoid version values was revealed. This matches the results of Matsumura et al. [9]. As Bockmann et al. [6] described, knowledge of the normal anatomy as well as the individual’s anatomy is essential to perform anatomic reconstruction in fractures and in shoulder arthroplasty. To our mind, the contralateral side can be considered a template for the reconstruction due to the good correlation between sides in glenoid version. Piponov et al. [10] did not detect any associations with patient body height and weight. However, by calculating fractional polynomials, our study detected more retroverted glenoids in taller participants. Regarding body weight, no significant association was determined. Further studies need to be performed before adjusted reference values can be calculated.
A limitation of our study may be the determination of the glenoid version in axial MRI slices of the thorax using 3-mm slices, which is comparable to a two-dimensional shoulder MRI of the clinical routine. However, we interpreted bilateral images acquired with the same method, which does not allow the alignment of the prescribed image volume to the glenoid or scapular blade and likely introduces measurement errors comparable to those from clinical unilateral scans on which the glenoid version is measured clinically. A further limitation is that our study does not use a three-dimensional approach. Kwon et al. [29] suggested that three-dimensional imaging could be beneficial, whereas several studies did not find any advantage of 3D measurements or any significant difference between 2D and 3D measurements of the glenoid version [31, 32].
Considering this limitation, a 2D measurement should be appropriate for an epidemiological approach. Regarding the measurement technique, most of the previous studies assessed the glenoid version on CT images [10, 11]. Due to the epidemiological design of our study, exposure to radiation was not ethically justifiable. Therefore, we used MRI images, which lead to a similar efficacy when measuring the glenoid version according to Cagle et al. [33]. Prada et al. even stated that the measurement of the glenoid version is not altered when the medial end of the scapula is only partially displayed on the axial MRI image [34].
Regarding dependencies, a limitation of our study may be its cross-sectional design, which limits conclusions about cause-and-effect relationships. The cross-sectional design meant to resemble a general population. This also means that individuals with secondary diseases like osteoporosis are included. These secondary disease could be cofounders. However, to our mind, the study design provided reliable results for the adult glenoid version.
Conclusion
There is a lack of established reference values and associated factors for the glenoid version, and valid reference values are needed. In this work, we have provided reliable data that were determined by applying reproducible imaging protocols to a large population-based cohort of 3004 adult participants. Moreover, we have identified multiple factors related to the glenoid version. Consequently, we have proposed sex- and age-adjusted reference values for the glenoid version as well as formulas to calculate them, allowing better interpretation in the future. Nonetheless, even with reliable reference values, radiological findings are not enough to declare a glenoid pathological. For evidence of cause–effect relationships, longitudinal studies are needed. Further studies are required to clarify whether different populations have different ranges of glenoid version.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- SHIP:
-
Study of Health in Pomerania
- TSA:
-
Total shoulder arthroplasty
- RSA:
-
Revserse shoulder arthroplasty
- MRI:
-
Magnetic resonance imaging
References
Aygün Ü, Çalik Y, Işik C, Şahin H, Şahin R, Aygün DÖ (2016) The importance of glenoid version in patients with anterior dislocation of the shoulder. J Shoulder Elbow Surg 25:1930–1936. https://doi.org/10.1016/j.jse.2016.09.018
Hohmann E, Tetsworth K (2015) Glenoid version and inclination are risk factors for anterior shoulder dislocation. J Shoulder Elbow Surg 24:1268–1273. https://doi.org/10.1016/j.jse.2015.03.032
Galvin JW, Parada SA, Li X, Eichinger JK (2016) Critical findings on magnetic resonance arthrograms in posterior shoulder instability compared with an age-matched controlled cohort. Am J Sports Med 44:3222–3229. https://doi.org/10.1177/0363546516660076
Imhoff FB, Camenzind RS, Obopilwe E, Cote MP, Mehl J, Beitzel K, Imhoff AB, Mazzocca AD, Arciero RA, Dyrna FGE (2019) Glenoid retroversion is an important factor for humeral head centration and the biomechanics of posterior shoulder stability. Knee Surg Sports Traumatol Arthrosc 27:3952–3961. https://doi.org/10.1007/s00167-019-05573-5
Eichinger JK, Massimini DF, Kim J, Higgins LD (2016) Biomechanical evaluation of glenoid version and dislocation direction on the influence of anterior shoulder instability and development of Hill-Sachs lesions. Am J Sports Med 44:2792–2799. https://doi.org/10.1177/0363546516659281
Bockmann B, Soschynski S, Lechler P, Schwarting T, Debus F, Soca B, Ruchholtz S, Frink M (2016) The osseous morphology of nondegenerated shoulders shows no side-related differences in elderly patients: an analysis of 102 computed tomography scans. J Shoulder Elbow Surg 25:1297–1302. https://doi.org/10.1016/j.jse.2015.12.024
Farron A, Terrier A, Büchler P (2006) Risks of loosening of a prosthetic glenoid implanted in retroversion. J Shoulder Elbow Surg 15:521–526. https://doi.org/10.1016/j.jse.2005.10.003
Churchill RS, Brems JJ, Kotschi H (2001) Glenoid size, inclination, and version: an anatomic study. J Shoulder Elbow Surg 10:327–332. https://doi.org/10.1067/mse.2001.115269
Matsumura N, Ogawa K, Kobayashi S, Oki S, Watanabe A, Ikegami H, Toyama Y (2014) Morphologic features of humeral head and glenoid version in the normal glenohumeral joint. J Shoulder Elbow Surg 23:1724–1730. https://doi.org/10.1016/j.jse.2014.02.020
Piponov HI, Savin D, Shah N, Esposito D, Schwartz B, Moretti V, Goldberg B (2016) Glenoid version and size: does gender, ethnicity, or body size play a role? Int Orthop 40:2347–2353. https://doi.org/10.1007/s00264-016-3201-8
Friedman RJ, Hawthorne KB, Genez BM (1992) The use of computerized tomography in the measurement of glenoid version. J Bone Joint Surg Am 74:1032–1037
de Wilde LF, Verstraeten T, Speeckaert W, Karelse A (2010) Reliability of the glenoid plane. J Shoulder Elbow Surg 19:414–422. https://doi.org/10.1016/j.jse.2009.10.005
Matsuki K, Sugaya H, Hoshika S, Ueda Y, Takahashi N, Tokai M, Banks SA (2019) Three-dimensional measurement of glenoid dimensions and orientations. J Orthop Sci 24:624–630. https://doi.org/10.1016/j.jos.2018.11.019
Tackett JJ, Ablove RH (2011) Magnetic resonance imaging study of glenohumeral relationships between genders. J Shoulder Elbow Surg 20:1335–1339. https://doi.org/10.1016/j.jse.2011.03.018
Bouchaib J, Clavert P, Kempf J-F, Kahn J-L (2014) Morphological analysis of the glenoid version in the axial plane according to age. Surg Radiol Anat 36:579–585. https://doi.org/10.1007/s00276-013-1238-6
Matsumura N, Ogawa K, Ikegami H, Collin P, Walch G, Toyama Y (2014) Computed tomography measurement of glenoid vault version as an alternative measuring method for glenoid version. J Orthop Surg Res 9:17. https://doi.org/10.1186/1749-799X-9-17
Völzke H, Alte D, Schmidt CO, Radke D, Lorbeer R, Friedrich N, Aumann N, Lau K, Piontek M, Born G, Havemann C, Ittermann T, Schipf S, Haring R, Baumeister SE, Wallaschofski H, Nauck M, Frick S, Arnold A, Jünger M, Mayerle J, Kraft M, Lerch MM, Dörr M, Reffelmann T, Empen K, Felix SB, Obst A, Koch B, Gläser S, Ewert R, Fietze I, Penzel T, Dören M, Rathmann W, Haerting J, Hannemann M, Röpcke J, Schminke U, Jürgens C, Tost F, Rettig R, Kors JA, Ungerer S, Hegenscheid K, Kühn J-P, Kühn J, Hosten N, Puls R, Henke J, Gloger O, Teumer A, Homuth G, Völker U, Schwahn C, Holtfreter B, Polzer I, Kohlmann T, Grabe HJ, Rosskopf D, Kroemer HK, Kocher T, Biffar R, John U, Hoffmann W (2011) Cohort profile: the study of health in Pomerania. Int J Epidemiol 40:294–307. https://doi.org/10.1093/ije/dyp394
Hegenscheid K, Kühn JP, Völzke H, Biffar R, Hosten N, Puls R (2009) Whole-body magnetic resonance imaging of healthy volunteers: pilot study results from the population-based SHIP study. RoFo 181:748–759. https://doi.org/10.1055/s-0028-1109510
Terrier A, Büchler P, Farron A (2006) Influence of glenohumeral conformity on glenoid stresses after total shoulder arthroplasty. J Shoulder Elbow Surg 15:515–520. https://doi.org/10.1016/j.jse.2005.09.021
Shapiro TA, McGarry MH, Gupta R, Lee YS, Lee TQ (2007) Biomechanical effects of glenoid retroversion in total shoulder arthroplasty. J Shoulder Elbow Surg 16:S90–S95. https://doi.org/10.1016/j.jse.2006.07.010
Brewer BJ, Wubben RC, Carrera GF (1986) Excessive retroversion of the glenoid cavity. a cause of non-traumatic posterior instability of the shoulder. J Bone Joint Surg Am 68:724–731
Graichen H, Koydl P, Zichner L (1999) Effectiveness of glenoid osteotomy in atraumatic posterior instability of the shoulder associated with excessive retroversion and flatness of the glenoid. Int Orthop 23:95–99. https://doi.org/10.1007/s002640050316
Pogorzelski J, Braun S, Imhoff AB, Beitzel K (2016) Open-wedge-glenoidosteotomie als therapie bei posteriorer schulterinstabilität aufgrund vermehrter glenoidretroversion (Open-wedge osteotomy of the glenoid for treatment of posterior shoulder instability with increased glenoid retroversion). Oper Orthop Traumatol 28:438–448. https://doi.org/10.1007/s00064-016-0457-5
Ortmaier R, Moroder P, Hirzinger C, Resch H (2017) Posterior open wedge osteotomy of the scapula neck for the treatment of advanced shoulder osteoarthritis with posterior head migration in young patients. J Shoulder Elbow Surg 26:1278–1286. https://doi.org/10.1016/j.jse.2016.11.005
Lacheta L, Singh TSP, Hovsepian JM, Braun S, Imhoff AB, Pogorzelski J (2019) Posterior open wedge glenoid osteotomy provides reliable results in young patients with increased glenoid retroversion and posterior shoulder instability. Knee Surg Sports Traumatol Arthrosc 27:299–304. https://doi.org/10.1007/s00167-018-5223-9
Iannotti JP, Greeson C, Downing D, Sabesan V, Bryan JA (2012) Effect of glenoid deformity on glenoid component placement in primary shoulder arthroplasty. J Shoulder Elbow Surg 21:48–55. https://doi.org/10.1016/j.jse.2011.02.011
Hsu JE, Ricchetti ET, Huffman GR, Iannotti JP, Glaser DL (2013) Addressing glenoid bone deficiency and asymmetric posterior erosion in shoulder arthroplasty. J Shoulder Elbow Surg 22:1298–1308. https://doi.org/10.1016/j.jse.2013.04.014
Welsch G, Mamisch TC, Kikinis R, Schmidt R, Lang P, Forst R, Fitz W (2003) CT-based preoperative analysis of scapula morphology and glenohumeral joint geometry. Comput Aided Surg 8:264–268. https://doi.org/10.3109/10929080309146062
Kwon YW, Powell KA, Yum JK, Brems JJ, Iannotti JP (2005) Use of three-dimensional computed tomography for the analysis of the glenoid anatomy. J Shoulder Elbow Surg 14:85–90. https://doi.org/10.1016/j.jse.2004.04.011
Matsen FA, Whitson A, Hsu JE, Stankovic NK, Neradilek MB, Somerson JS (2019) Prearthroplasty glenohumeral pathoanatomy and its relationship to patient’s sex, age, diagnosis, and self-assessed shoulder comfort and function. J Shoulder Elbow Surg 28:2290–2300. https://doi.org/10.1016/j.jse.2019.04.043
Budge MD, Lewis GS, Schaefer E, Coquia S, Flemming DJ, Armstrong AD (2011) Comparison of standard two-dimensional and three-dimensional corrected glenoid version measurements. J Shoulder Elbow Surg 20:577–583. https://doi.org/10.1016/j.jse.2010.11.003
Rouleau DM, Kidder JF, Pons-Villanueva J, Dynamidis S, Defranco M, Walch G (2010) Glenoid version: how to measure it? Validity of different methods in two-dimensional computed tomography scans. J Shoulder Elbow Surg 19:1230–1237. https://doi.org/10.1016/j.jse.2010.01.027
Cagle PJ, Werner B, Shukla DR, London DA, Parsons BO, Millar NL (2019) Interobserver and intraobserver comparison of imaging glenoid morphology, glenoid version and humeral head subluxation. Shoulder Elbow 11:204–209. https://doi.org/10.1177/1758573218768507
Parada SA, Shaw KA, Antosh IJ, Eichinger JK, Li X, Curry EJ, Provencher MT (2020) Magnetic resonance imaging correlates with computed tomography for glenoid version calculation despite lack of visibility of medial scapula. Arthroscopy 36:99–105. https://doi.org/10.1016/j.arthro.2019.07.030
Acknowledgements
The authors thank the initiators and coordinators of the SHIP project. We acknowledge support from the Open Access Publication Fund of the University of Tübingen.
Funding
Open Access funding enabled and organized by Projekt DEAL. This study was performed as a SHIP-associated project (SHIP/2015/145/D) at University Medicine Greifswald, Germany. The SHIP study is part of the Community Medicine Research Net of the University of Greifswald, Germany, which is funded by the Federal Ministry of Education and Research (grant no. 03ZIK012), the Ministry of Cultural Affairs, as well as the Social Ministry of the Federal State of Mecklenburg–West Pomerania. MR imaging was supported by the Federal State of Mecklenburg-Vorpommern, the Federal Ministry of Education and Research, and a joint grant from Siemens Healthcare, Erlangen, Germany.
Author information
Authors and Affiliations
Contributions
C.F., R.G. and C.E.G. compiled the data and authored the manuscript. M.F. and T.I. collected and compiled the data. R.B. and C.S. contributed to the preparation and to the interpretation of the results. J.L. proofread the manuscript. All authors provided critical feedback and helped shape the research, analysis and manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the local ethics committee (BB 39/08, 19.06.2008). Each participant gave written informed consent to participate in the study.
Consent for publication
Each participant gave written informed consent for publication.
Competing interests
There are no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fischer, C.S., Floß, M., Ittermann, T. et al. Gender-specific factors influencing the glenoid version and reference values for it. J Orthop Traumatol 25, 39 (2024). https://doi.org/10.1186/s10195-024-00778-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s10195-024-00778-y