
Abstract
Background
This systematic review investigates the role of synthetic graft for primary medial patellofemoral ligament (MPFL) reconstruction in patients with recurrent patellofemoral instability, focusing on clinical scores and the rate of complications.
Methods
This systematic review was conducted according to the PRISMA statement. The main online databases were accessed in January 2022 without time constraints. All clinical studies investigating the use of synthetic grafts for MPFL reconstruction were accessed. Revision settings were not considered. Only articles reporting data on patients with recurrent patellofemoral instability were eligible. Studies regarding congenital or acute patellofemoral dislocation were excluded. Only studies performing a follow-up longer than 24 months were considered.
Results
Data on 199 patients [mean age 22.3 (range 19.0–28.0) years] were collected. The mean follow-up was 60.5 (39.0–142.8) months. All the scores of interest improved at last follow-up: Kujala (+ 24.8; P = 0.0002), Lysholm (+ 42.0; P = 0.02), Tegner (+ 1.2; P = 0.03), IKDC (+ 20.9; P = 0.02). Post-operatively, a positive apprehension test was detected in 6.1% (7/115) of patients, and a sensation of instability was reported by 1.5% (3/199) of patients. The rate of re-dislocations was 2.5% (5 of 199 patients), and revision procedures were performed in less than 1% (1 of 199) of patients.
Conclusion
Synthetic graft may be reliable and feasible for primary MPFL reconstruction in patients with recurrent patellofemoral instability.
Similar content being viewed by others


Introduction
Patellofemoral instability (PFI) is common, especially in active adolescents [1,2,3]. The etiology of PFI is multifactorial, with several pathoanatomical risk factors predisposing to instability [4,5,6,7,8]. Moreover, most patients who suffer from PFI present several risk factors which synergistically predispose to instability [9,10,11]. Clinically, patients with PFI experience patellar subluxations and dislocations [11,12,13]. Lateral patellar displacement of the patella usually damages the medial patellofemoral ligament (MPFL) [14]. This ligament is the most important passive stabilizer of abnormal patellar lateralization during the first degrees of knee flexion [15, 16]. Thus, surgical MPFL reconstruction may be recommended to avoid persistent instability and further dislocations [12, 13, 17,18,19]. MPFL reconstruction achieves very good outcomes and patient satisfaction, along with a low rate of complications [3, 14, 20,21,22,23]. Given the greater lateralizing forces acting on the MPFL in patients with PFI [24,25,26], accurate reconstruction and graft selection are pivotal. While allografts and autografts are widely employed for MPFL reconstruction, the role of synthetic graft for this purpose is still unclear [18, 27,28,29,30,31,32]. Most of the literature pertaining to synthetic graft for MPFL reconstruction is based on retrospective investigations with heterogeneous criteria and results. Despite the limited evidence, results from these studies are promising. Thus, we conducted a systematic review investigating the role of synthetic graft for primary MPFL reconstruction in patients with recurrent PFI. The focus of the present study was on clinical scores and the rate of complications.
Material and methods
Search strategy
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the PRISMA statement [33]. A PIOT algorithm was performed preliminarily:
-
P (problem): patellofemoral instability;
-
I (intervention): synthetic MPFL reconstruction;
-
O (outcomes): clinical scores and complications;
-
T (timing): > 24 months of follow-up.
Data source and extraction
Two authors independently (F.M. & J.E.) performed the literature search in January 2022. The following databases were accessed: PubMed, Google Scholar, Embase, and Scopus. No time constraints were set for the database search. The following keywords were used in combination: knee, patella, patellofemoral, joint, instability, synthetic, dislocations, apprehension, subluxation, revision, failure, revision, Tegner, Kujala, Lysholm, score, graft, medial patellofemoral ligament, MPFL, rupture, tear, reconstruction, pain, trochlea. The resulting articles were screened by the same two authors. The full text of the articles of interest was accessed. The bibliographies of the full-text articles were also screened. Disagreements were debated and solved by a third author (N.M.).
Eligibility criteria
All the clinical studies investigating the role of synthetic graft for MPFL reconstruction were accessed. Given the authors’ language capabilities, articles in English, German, Italian, French and Spanish were considered. Studies of evidence of levels I–III according to the Oxford Centre of Evidence-Based Medicine [34] were eligible. Only articles reporting data on patients with recurrent PFI were eligible. Only studies performing a follow-up longer than 24 months were eligible. Only articles reporting quantitative data on the outcomes of interest were considered for inclusion. Missing data on the outcomes of interest warranted exclusion from this study. Reviews or meta-analyses, editorials, letters, expert opinions, and case reports were not considered. Articles reporting data from registries were also not eligible. Cadaveric, animal and biomechanical studies were not included; nor were articles regarding revision settings. Studies regarding congenital or acute patellofemoral dislocation were also excluded. Only studies reporting quantitative data on the outcomes of interest were included.
Outcomes of interest
Two authors (F.M. & J.E.) independently performed data extraction. Data on study generalities (author and year, journal, study design, follow-up), baseline characteristics of the patients (number of procedures, mean age), type of graft and intervention (isolated and/or combined) were collected. The outcomes of interest were the following: the Kujala Anterior Knee Pain Scale [35], the Lysholm Knee Scoring Scale [36], the Tegner Activity Scale [37] and the International Knee Documentation Committee (IKDC) [38]. The following complications were recorded: positive apprehension test, persistent sensation of instability, and rates of revision and re-dislocation. Persistent instability was defined as recurrence and/or a subjective sensation of subluxation or instability [39, 40].
Methodological quality assessment
To evaluate the methodological quality assessment, the Coleman Methodology Score (CMS) [41] was applied. An independent author (A.P.) performed the scoring. Part A of the CMS analyses the study size, follow-up, surgical approach, type of analysis, description of diagnosis, surgical technique and postoperative rehabilitation. Part B focuses on the outcome criteria along with related assessing procedures and the description of the subject selection process. The CMS for the quality of the study was calculated. The CMS can range from 0 (poor) to 100 (excellent), with a score of > 60 considered satisfactory.
Statistical analysis
The statistical analyses were performed by the main author (F.M.). IBM SPSS software (version 25) was used. Continuous variables were analysed through the mean difference (MD), while the complication rate was analysed through the odds ratio (OR) effect measure. Confidence intervals (CIs) were set at 95% in all comparisons. The t-test was used to assess significance for continuous variables, and the \(\chi\)2 test was used for dichotomous ones. Values of P < 0.05 were considered statistically significant.
Results
Search results
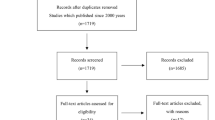
The literature search resulted in 494 articles. Of these, 155 were excluded because they were duplicates. A further 332 articles were excluded because they did not match the topic (N = 184), they were not clinical studies or had a poor level of evidence (N = 92), there were language limitations (N = 9), they considered the treatment of acute/congenital/habitual dislocations and/or revision settings (N = 19), they had a short follow-up (N = 7), there was a lack of quantitative data on the outcomes of interest (N = 14), or they had a high risk of bias (e.g. they had uncertain results or a population that was too small; N = 7). This left seven investigations for inclusion: three prospective and four retrospective clinical studies. The flow chart of the literature search results is shown in Fig. 1.

Flow chart of the literature search
Methodological quality assessment
The CMS highlighted several strengths and limitations of the articles included in this study. The retrospective design of most studies represents the most important limitation. The surgical approach, diagnosis and rehabilitation were often well described, representing important strengths of this study. Criteria selection, outcome measures and related timing of assessment were adequately described. General health measures were rarely reported, while the procedures used to assess outcomes were often biased. The CMS of this study was 71 points, attesting that it provides a good methodological quality assessment. The results for the CMS are shown in Table 1.
Patient demographics
Data from 199 patients were available. The mean age of the patients was 22.3 (19.0 to 28.0) years. The mean follow-up was 60.5 (39.0 to 142.8) months. Four studies reported a double-bundle reconstruction, while three reported a single-bundle reconstruction. The generalities and patient baselines of the included studies are shown in Table 2.
Outcomes of interest
All the scores of interest improved at last follow-up: Kujala (+ 24.8; P = 0.0002), Lysholm (+ 42.0; P = 0.02), Tegner (+ 1.2; P = 0.03), and IKDC (+ 20.9; P = 0.02). A positive apprehension test was detected in 6.1% (7/115) of patients, while a persistent sensation of instability was present in 1.5% (3/199) of patients. The rate of re-dislocations was 2.5% (5 of 199 patients), while the rate of revision was less than 1% (1 of 199 patients). Table 3 shows the results for the scores.
Double-bundle vs single-bundle patellar fixation subgroups
There was similarity of the two groups at baseline concerning follow-up duration, age and number of patients (P > 0.1). No difference was found between single- and double-bundle reconstruction with regards to the apprehension test (OR 0.05; 95% CI: 0.0026 to 0.8261; P = 0.05), persistent instability (OR 0.6; 95% CI: 0.0570 to 7.1707; P = 0.7), re-dislocation rate (OR 0.1; 95% CI: 0.0061 to 2.0478; P = 0.1) and revision rate (OR 3.9; 95% CI: 0.1570 to 96.9637; P = 0.4). These results are shown in detail in Table 4.
Discussion
According to the main findings of the present systematic review, synthetic graft can be a reliable and feasible option for primary MPFL reconstruction in patients with recurrent PFI. All the scores of interest significantly improved postoperatively, and all exceeded the relevant minimally clinically important difference (MCID) at last follow-up [37, 49, 50]. The rate of complications was similar to those reported in previous reviews concerning MPFL reconstruction with an autograft [51,52,53,54]. No difference was found between single- and double-bundle patellar fixation techniques.
McNeilan et al. [55] performed a systematic review in 2018 that analysed three studies (76 patients) in a synthetic reconstruction cohort. Similar to the main findings of the present study, synthetic grafts achieved excellent clinical outcomes, with low complication rates.
Graft choice is complex, and to date there are no agreed recommendations. Most surgeon prefer autografts. Of the several tendon autografts available, the most commonly used are gracilis and semitendinosus tendon autografts [3, 26,27,28, 31, 56,57,58,59,60] because of their intrinsic biomechanical properties [61], geometric properties [62], availability and low donor-site morbidity [63]. In the current literature, to our knowledge, there is only one study protocol for a randomized controlled trial comparing synthetic versus autologous graft for MPFL reconstruction (ISRCTN 16657952, March 2017) [64]. The ideal biomechanical properties (e.g. stiffness, viscoelasticity, tensile strength, thickness) of a graft for MPLF reconstruction remain undefined. Indeed, the tendency for lateralization of the patella is related to the presence and amount of pathoanatomical risk factors and the bone morphology. Thus, graft selection should be customized accordingly. In this context, the mechanical properties of synthetic grafts can be adapted to the surgeon’s preferences. Compared to autografts, synthetic grafts allow a shorter surgical duration and lead to less donor-site morbidity, most likely inducing less post-operative pain. Regarding the latter two issues, their prevention may favour the early phases of rehabilitation. While tendon grafts have the tendency to stretch over time, the biomechanical properties of a synthetic graft are predictable. This is important to remember during graft tensioning, since overtightening of the synthetic graft must be avoided. To avoid overtightening, Lee et al. [45] suggest tensioning the MPFL graft under direct arthroscopic vision to observe the patella position over the trochlea without the use of a thigh tourniquet. In a retrospective study, Suganuma et al. [48] investigated whether the position of the patella in the trochlea after MPFL reconstruction using a synthetic graft (Poly-Tape) affects surgical outcome. They suggest that slight undertensioning or residual lateral positioning of the patella within the trochlear groove may have a positive influence on surgical outcomes [48]. Lee et al. [45] compared synthetic versus autologous grafts for MPFL reconstruction. They reported no differences between a gracilis autograft and ultra-high-molecular-weight polyester FiberTape (Arthrex, FL, USA) in clinical outcomes and complications. Tsushima et al. [65] compared the biomechanical properties of FiberTape with a semitendinosus autograft for MPFL reconstruction. They concluded that MPFL reconstruction using FiberTape was stronger than the native MPFL, and that a semitendinosus autograft with soft-tissue anchors was weaker than FiberTape with knotless anchors. The latter achieves enough strength for MPFL reconstruction, avoiding the complications associated with graft harvesting. These considerations allow new insight and perpectives in our understanding of MPFL reconstruction.
This study does not come without limitations. The current literature lacks investigations concerning synthetic grafts for MPFL reconstruction. Consequently, the number of procedures for analysis was limited. The retrospective design and small sample sizes of most of the investigations negatively affected the reliability of the present study. This systematic review considered patients with different degrees of patellar instability. Some authors also reported data on MPFL reconstruction with combined proximal and distal alignment. However, given the lack of available data and information, it was not possible to conduct further subgroup analyses. Patients with acute patellofemoral dislocation were not included in the present study. The treatment of acute patellofemoral dislocation is controversial [17, 66,67,68]. Surgery is indicated as the first-line management in patients with displaced osteochondral defects or mechanical symptoms [69,70,71]. However, a growing tendency to treat the first patellar dislocation surgically has been evidenced [72, 73]. Given these controversies, studies which performed primary surgery in patients with acute patellofemoral dislocation were not considered. The eligibility criteria of the studies included for analysis were heterogeneous. Indeed, Nomura et al. [47] included patients with previous surgical intervention, while three of the seven included studies [42, 43, 46] did not report relevant information. Suganuma et al. [48] were the only authors who excluded patients with pathoanatomical risk factors, while there was high variability among the other included studies. Khemka et al. [44] also included patients with pathological ligamentous laxity. This heterogeneity certainly introduces an important source of bias; however, considering the lack of data in the literature, no additional subgroup analyses were possible. We must further acknowledge that two studies also combined MPFL reconstruction with tibial tuberosity transposition for different indications in a small percentage of patients. The Elmslie–Trillat procedure was performed by Berruto et al. [42] in patients with tibial tubercle-tibial groove (TT-TG) distance greater than 20 mm (5 of 18 procedures). Khemka et al. [44] performed tibial tuberosity medialization in patients with TT-TG > 15 mm (2 of 31 procedures). Moreover, they also combined every MPFL reconstruction procedure with lateral retinacular release (LRR). LRR was also performed by Nomura et al. [46, 47] in patients with severe tightness of the lateral patellar structures. Patellar and femoral graft fixation was heterogeneous among the studies, thus representing another possible source of bias. Some authors did not state whether additional surgical procedures were performed. Lastly, the dimensions and type of the synthetic ligament used was also dissimilar between the studies. Therefore, given these limitations, results from the present study must be interpreted with caution. Future studies should improve these limitations, allowing for higher-quality analyses.
Conclusion
According to the main findings of the present systematic review, synthetic graft may be reliable and feasible for primary MPFL reconstruction in patients with recurrent patellofemoral instability. Results must be interpreted within the limitations of this study.
Availability of data and materials
The data underlying this article are available in the article and in its online supplementary material.
Abbreviations
- MPFL:
-
Medial patellofemoral ligament
- PFI:
-
Patellofemoral instability
- CMS:
-
Coleman Methodology Score
- MD:
-
Mean difference
- OR:
-
Odds ratio
- CI:
-
Confidence interval
References
Sillanpää PMV, Iivonen T et al (2008) Incidence and risk factors of acute traumatic primary patellar dislocation. Med Sci Sports Exerc 40(4):606–611
Migliorini F, Marsilio E, Cuozzo F, Oliva F, Eschweiler J, Hildebrand F, Maffulli N (2021) Chondral and soft tissue injuries associated to acute patellar dislocation: a systematic review. Life (Basel). https://doi.org/10.3390/life11121360
Migliorini F, Rath B, Tingart M, Meisen N, Eschweiler J (2019) Surgical management for recurrent patellar dislocations in skeletally immature patients. Eur J Orthop Surg Traumatol 29(8):1815–1822. https://doi.org/10.1007/s00590-019-02483-7
Vetrano M, Oliva F, Bisicchia S, Bossa M, De Carli A, Di Lorenzo L, Erroi D, Forte A, Foti C, Frizziero A, Gasparre G, Via AG, Innocenti B, Longo UG, Mahmoud A, Masiero S, Mazza D, Natali S, Notarangelo C, Osti L, Padulo J, Pellicciari L, Perroni F, Piccirilli E, Ramponi C, Salvatore G, Panni AS, Suarez T, Tarantino U, Vittadini F, Vulpiani MC, Ferretti A, Maffulli N (2017) I.S.Mu.L.T. first-time patellar dislocation guidelines. Muscles Ligaments Tendons J 7(1):1–10. https://doi.org/10.11138/mltj/2017.7.1.001
Petri M, Ettinger M, Stuebig T, Brand S, Krettek C, Jagodzinski M, Omar M (2015) Current concepts for patellar dislocation. Arch Trauma Res 4(3):e29301. https://doi.org/10.5812/atr.29301
Bartsch A, Lubberts B, Mumme M, Egloff C, Pagenstert G (2018) Does patella alta lead to worse clinical outcome in patients who undergo isolated medial patellofemoral ligament reconstruction? A systematic review. Arch Orthop Trauma Surg 138(11):1563–1573. https://doi.org/10.1007/s00402-018-2971-4
Ren B, Zhang X, Zhang L, Zhang M, Liu Y, Tian B, Zhang B, Zheng J (2019) Isolated trochleoplasty for recurrent patellar dislocation has lower outcome and higher residual instability compared with combined MPFL and trochleoplasty: a systematic review. Arch Orthop Trauma Surg 139(11):1617–1624. https://doi.org/10.1007/s00402-019-03244-1
Felli L, Alessio-Mazzola M, Lovisolo S, Capello AG, Formica M, Maffulli N (2021) Anatomy and biomechanics of the medial patellotibial ligament: a systematic review. Surgeon 19(5):e168–e174. https://doi.org/10.1016/j.surge.2020.09.005
Boling MC, Padua DA, Marshall SW, Guskiewicz K, Pyne S, Beutler A (2009) A prospective investigation of biomechanical risk factors for patellofemoral pain syndrome: the Joint Undertaking to Monitor and Prevent ACL Injury (JUMP-ACL) cohort. Am J Sports Med 37(11):2108–2116. https://doi.org/10.1177/0363546509337934
Steensen RN, Bentley JC, Trinh TQ, Backes JR, Wiltfong RE (2015) The prevalence and combined prevalences of anatomic factors associated with recurrent patellar dislocation: a magnetic resonance imaging study. Am J Sports Med 43(4):921–927. https://doi.org/10.1177/0363546514563904
Migliorini F, Eschweiler J, Betsch M, Knobe M, Tingart M, Maffulli N (2021) Prognostic factors for isolated medial patellofemoral ligament reconstruction: a systematic review. Surgeon. https://doi.org/10.1016/j.surge.2021.03.003
Panni AS, Alam M, Cerciello S, Vasso M, Maffulli N (2011) Medial patellofemoral ligament reconstruction with a divergent patellar transverse 2-tunnel technique. Am J Sports Med 39(12):2647–2655. https://doi.org/10.1177/0363546511420079
Maffulli N, Aicale R, D’Addona A, Young DA, Kader DF, Oliva F (2020) Combined medial patellofemoral and patellotibial reconstruction with soft tissue fixation in recurrent patellar dislocation. Injury 51(8):1867–1873. https://doi.org/10.1016/j.injury.2020.06.028
Carmont MR, Maffulli N (2007) Medial patellofemoral ligament reconstruction: a new technique. BMC Musculoskelet Disord 8:22. https://doi.org/10.1186/1471-2474-8-22
Desio SM, Burks RT, Bachus KN (1998) Soft tissue restraints to lateral patellar translation in the human knee. Am J Sports Med 26(1):59–65. https://doi.org/10.1177/03635465980260012701
Conlan T, Garth WP Jr, Lemons JE (1993) Evaluation of the medial soft-tissue restraints of the extensor mechanism of the knee. J Bone Joint Surg Am 75(5):682–693. https://doi.org/10.2106/00004623-199305000-00007
Migliorini F, Driessen A, Quack V, Gatz M, Tingart M, Eschweiler J (2020) Surgical versus conservative treatment for first patellofemoral dislocations: a meta-analysis of clinical trials. Eur J Orthop Surg Traumatol. https://doi.org/10.1007/s00590-020-02638-x
Migliorini F, Driessen A, Quack V, Schenker H, Tingart M, Eschweiler J (2021) Correction to: Patellar fixation graft via suture anchors versus tunnel techniques during isolated MPFL reconstruction for recurrent patellofemoral instability: a systematic review of the literature. Arch Orthop Trauma Surg 141(9):1625–1626. https://doi.org/10.1007/s00402-021-03987-w
Longo UG, Berton A, Salvatore G, Migliorini F, Ciuffreda M, Nazarian A, Denaro V (2016) Medial patellofemoral ligament reconstruction combined with bony procedures for patellar instability: current indications, outcomes, and complications. Arthroscopy 32(7):1421–1427. https://doi.org/10.1016/j.arthro.2016.01.013
Reagan J, Kullar R, Burks R (2015) MPFL reconstruction: technique and results. Orthop Clin North Am 46(1):159–169. https://doi.org/10.1016/j.ocl.2014.09.012
Migliorini F, Driessen A, Quack V, Schenker H, Tingart M, Eschweiler J (2020) Patellar fixation graft via suture anchors versus tunnel techniques during isolated MPFL reconstruction for recurrent patellofemoral instability: a systematic review of the literature. Arch Orthop Trauma Surg. https://doi.org/10.1007/s00402-020-03420-8
Ronga M, Oliva F, Longo UG, Testa V, Capasso G, Maffulli N (2009) Isolated medial patellofemoral ligament reconstruction for recurrent patellar dislocation. Am J Sports Med 37(9):1735–1742. https://doi.org/10.1177/0363546509333482
Migliorini F, Rath B, Tingart M, Niewiera M, Eschweiler J (2019) Distal alignment procedures for patellofemoral instability: comprehensive review of the literature. Eur J Orthop Surg Traumatol 29(7):1579–1588. https://doi.org/10.1007/s00590-019-02451-1
Migliorini F, Trivellas A, Driessen A, Quack V, Tingart M, Eschweiler J (2020) Graft choice for isolated MPFL reconstruction: gracilis versus semitendinosus. Eur J Orthop Surg Traumatol. https://doi.org/10.1007/s00590-020-02636-z
Migliorini F, Driessen A, Quack V, Schenker H, Tingart M, Eschweiler J (2020) Patellar fixation graft via suture anchors versus tunnel techniques during isolated MPFL reconstruction for recurrent patellofemoral instability: a systematic review of the literature. Arch Orthop Trauma Surg 140(9):1201–1210. https://doi.org/10.1007/s00402-020-03420-8
Migliorini F, Trivellas A, Colarossi G, Eschweiler J, Tingart M, Rath B (2020) Single- versus double-bundle patellar graft insertion for isolated MPFL reconstruction in patients with patellofemoral instability: a systematic review of the literature. Arch Orthop Trauma Surg 140(6):769–776. https://doi.org/10.1007/s00402-020-03376-9
Abramowitch SD, Zhang X, Curran M, Kilger R (2010) A comparison of the quasi-static mechanical and non-linear viscoelastic properties of the human semitendinosus and gracilis tendons. Clin Biomech (Bristol, Avon) 25(4):325–331. https://doi.org/10.1016/j.clinbiomech.2009.12.007
Kyung HS, Kim HJ (2015) Medial patellofemoral ligament reconstruction: a comprehensive review. Knee Surg Relat Res 27(3):133–140. https://doi.org/10.5792/ksrr.2015.27.3.133
Marcheggiani Muccioli GM, Lullini G, Grassi A, Macchiarola L, Cammisa E, Maccaferri B, Rinaldi VG, Di Paolo S, Zaffagnini S (2020) Good results are reported at 60-month follow-up after medial patello-femoral ligament reconstruction with fascia lata allograft for recurrent patellar dislocation. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-020-06142-x
Migliorini F, Maffulli N, Eschweiler J, Quack V, Tingart M, Driessen A (2021) Lateral retinacular release combined with MPFL reconstruction for patellofemoral instability: a systematic review. Arch Orthop Trauma Surg 141(2):283–292. https://doi.org/10.1007/s00402-020-03689-9
Migliorini F, Trivellas A, Eschweiler J, Betsch M, Tingart M, Maffulli N (2021) Pedicled strip of quadriceps tendon graft for primary medial patellofemoral ligament reconstruction in recurrent patellofemoral instability: a systematic review. Arthroscopy 37(6):1992–1999. https://doi.org/10.1016/j.arthro.2021.01.048
Migliorini F, Trivellas A, Eschweiler J, Knobe M, Tingart M, Maffulli N (2021) Comparable outcome for autografts and allografts in primary medial patellofemoral ligament reconstruction for patellofemoral instability: systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-021-06569-w
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339:b2535. https://doi.org/10.1136/bmj.b2535
Howick J, Chalmers I, Glasziou P, Greenhalgh T, Heneghan C, Liberati A, Moschetti I, Phillips B, Thornton H, Goddard O, Hodgkinson M (2011) The 2011 Oxford CEBM levels of evidence. Oxford Centre for Evidence-Based Medicine, Oxford. https://www.cebm.net/indexaspx?o=5653. Accessed Jan 2022
Kujala UM, Jaakkola LH, Koskinen SK, Taimela S, Hurme M, Nelimarkka O (1993) Scoring of patellofemoral disorders. Arthroscopy 9(2):159–163
Lysholm J, Gillquist J (1982) Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am J Sports Med 10(3):150–154. https://doi.org/10.1177/036354658201000306
Briggs KK, Lysholm J, Tegner Y, Rodkey WG, Kocher MS, Steadman JR (2009) The reliability, validity, and responsiveness of the Lysholm score and Tegner activity scale for anterior cruciate ligament injuries of the knee: 25 years later. Am J Sports Med 37(5):890–897. https://doi.org/10.1177/0363546508330143
Higgins LD, Taylor MK, Park D, Ghodadra N, Marchant M, Pietrobon R, Cook C, International Knee Documentation Committee (2007) Reliability and validity of the International Knee Documentation Committee (IKDC) Subjective Knee Form. Joint Bone Spine 74(6):594–599. https://doi.org/10.1016/j.jbspin.2007.01.036
Nikku R, Nietosvaara Y, Aalto K, Kallio PE (2005) Operative treatment of primary patellar dislocation does not improve medium-term outcome: a 7-year follow-up report and risk analysis of 127 randomized patients. Acta Orthop 76(5):699–704. https://doi.org/10.1080/17453670510041790
Aicale R, Maffulli N (2020) Combined medial patellofemoral and medial patellotibial reconstruction for patellar instability: a PRISMA systematic review. J Orthop Surg Res 15(1):529. https://doi.org/10.1186/s13018-020-02072-z
Coleman BD, Khan KM, Maffulli N, Cook JL, Wark JD (2000) Studies of surgical outcome after patellar tendinopathy: clinical significance of methodological deficiencies and guidelines for future studies. Victorian Institute of Sport Tendon Study Group. Scand J Med Sci Sports 10(1):2–11. https://doi.org/10.1034/j.1600-0838.2000.010001002.x
Berruto M, Ferrua P, Uboldi F, Usellini E, Gala L, Tassi A, Marelli B (2014) Medial patellofemoral ligament reconstruction with bioactive synthetic ligament is an option. A 3-year follow-up study. Knee Surg Sports Traumatol Arthrosc 22(10):2419–2425. https://doi.org/10.1007/s00167-014-2970-0
Ellera Gomes JL (1992) Medial patellofemoral ligament reconstruction for recurrent dislocation of the patella: a preliminary report. Arthroscopy 8(3):335–340
Khemka A, Lord SJ, Doyle Z, Bosley B, Al Muderis M (2016) Minimally invasive medial patellofemoral ligament reconstruction for patellar instability using an artificial ligament: A two year follow-up. Knee 23(2):261–266. https://doi.org/10.1016/j.knee.2015.07.002
Lee PYF, Golding D, Rozewicz S, Chandratreya A (2018) Modern synthetic material is a safe and effective alternative for medial patellofemoral ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 26(9):2716–2721. https://doi.org/10.1007/s00167-017-4711-7
Nomura E, Horiuchi Y, Kihara M (2000) A mid-term follow-up of medial patellofemoral ligament reconstruction using an artificial ligament for recurrent patellar dislocation. Knee 7(4):211–215
Nomura E, Inoue M, Kobayashi S (2007) Long-term follow-up and knee osteoarthritis change after medial patellofemoral ligament reconstruction for recurrent patellar dislocation. Am J Sports Med 35(11):1851–1858. https://doi.org/10.1177/0363546507306161
Suganuma J, Mochizuki R, Sugiki T, Inoue Y, Kitamura K, Akutsu S, Ono H (2016) Reconstruction of the medial patellofemoral ligament using a synthetic graft with arthroscopic control of patellofemoral congruence. Arthroscopy 32(11):2259–2268. https://doi.org/10.1016/j.arthro.2016.02.004
Collins NJ, Misra D, Felson DT, Crossley KM, Roos EM (2011) Measures of knee function: International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form, Knee Injury and Osteoarthritis Outcome Score (KOOS), Knee Injury and Osteoarthritis Outcome Score Physical Function Short Form (KOOS-PS), Knee Outcome Survey Activities of Daily Living Scale (KOS-ADL), Lysholm Knee Scoring Scale, Oxford Knee Score (OKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Activity Rating Scale (ARS), and Tegner Activity Score (TAS). Arthritis Care Res (Hoboken) 63(Suppl 11):S208–228. https://doi.org/10.1002/acr.20632
Mostafaee N, Negahban H, Shaterzadeh Yazdi MJ, Goharpey S, Mehravar M, Pirayeh N (2020) Responsiveness of a Persian version of Knee Injury and Osteoarthritis Outcome Score and Tegner activity scale in athletes with anterior cruciate ligament reconstruction following physiotherapy treatment. Physiother Theory Pract 36(9):1019–1026. https://doi.org/10.1080/09593985.2018.1548672
Nha KW, Bae JH, Hwang SC, Nam YJ, Shin MJ, Bhandare NN, Kumar A, Kang DG, Lee DY (2019) Medial patellofemoral ligament reconstruction using an autograft or allograft for patellar dislocation: a systematic review. Knee Surg Relat Res 31(1):8. https://doi.org/10.1186/s43019-019-0008-0
Stupay KL, Swart E, Shubin Stein BE (2015) Widespread implementation of medial patellofemoral ligament reconstruction for recurrent patellar instability maintains functional outcomes at midterm to long-term follow-up while decreasing complication rates: a systematic review. Arthroscopy 31(7):1372–1380. https://doi.org/10.1016/j.arthro.2014.12.029
Mackay ND, Smith NA, Parsons N, Spalding T, Thompson P, Sprowson AP (2014) Medial patellofemoral ligament reconstruction for patellar dislocation: a systematic review. Orthop J Sports Med 2(8):2325967114544021. https://doi.org/10.1177/2325967114544021
Schiphouwer L, Rood A, Tigchelaar S, Koeter S (2017) Complications of medial patellofemoral ligament reconstruction using two transverse patellar tunnels. Knee Surg Sports Traumatol Arthrosc 25(1):245–250. https://doi.org/10.1007/s00167-016-4245-4
McNeilan RJ, Everhart JS, Mescher PK, Abouljoud M, Magnussen RA, Flanigan DC (2018) Graft choice in isolated medial patellofemoral ligament reconstruction: a systematic review with meta-analysis of rates of recurrent instability and patient-reported outcomes for autograft, allograft, and synthetic options. Arthroscopy 34(4):1340–1354. https://doi.org/10.1016/j.arthro.2017.11.027
Migliorini F, Baroncini A, Eschweiler J, Tingart M, Maffulli N (2020) Interference screws vs. suture anchors for isolated medial patellofemoral ligament femoral fixation: a systematic review. J Sport Health Sci. https://doi.org/10.1016/j.jshs.2020.11.011
Migliorini F, Oliva F, Maffulli GD, Eschweiler J, Knobe M, Tingart M, Maffulli N (2021) Isolated medial patellofemoral ligament reconstruction for recurrent patellofemoral instability: analysis of outcomes and risk factors. J Orthop Surg Res 16(1):239. https://doi.org/10.1186/s13018-021-02383-9
Migliorini F, Trivellas A, Driessen A, Quack V, Tingart M, Eschweiler J (2020) Graft choice for isolated MPFL reconstruction: gracilis versus semitendinosus. Eur J Orthop Surg Traumatol 30(5):763–770. https://doi.org/10.1007/s00590-020-02636-z
Maffulli N, Aicale R, Tarantino D, Young DA (2019) Combined reconstruction of the medial patellotibial and patellofemoral ligaments. Muscle Ligaments Tendons J 09:181. https://doi.org/10.32098/mltj.02.2019.06
Migliorini F, Trivellas A, Colarossi G, Eschweiler J, Tingart M, Rath B (2021) Correction to: Single versus doublebundle patellar graft insertion for isolated MPFL reconstruction in patients with patellofemoral instability: a systematic review of the literature. Arch Orthop Trauma Surg 141(9):1627. https://doi.org/10.1007/s00402-021-04012-w
West RV, Harner CD (2005) Graft selection in anterior cruciate ligament reconstruction. J Am Acad Orthop Surg 13(3):197–207
Coobs BR, LaPrade RF, Griffith CJ, Nelson BJ (2007) Biomechanical analysis of an isolated fibular (lateral) collateral ligament reconstruction using an autogenous semitendinosus graft. Am J Sports Med 35(9):1521–1527. https://doi.org/10.1177/0363546507302217
Maletis GB, Cameron SL, Tengan JJ, Burchette RJ (2007) A prospective randomized study of anterior cruciate ligament reconstruction: a comparison of patellar tendon and quadruple-strand semitendinosus/gracilis tendons fixed with bioabsorbable interference screws. Am J Sports Med 35(3):384–394. https://doi.org/10.1177/0363546506294361
Tucker A, McMahon S, McArdle B, Rutherford B, Acton D (2018) Synthetic versus autologous reconstruction (Syn-VAR) of the medial patellofemoral ligament: a study protocol for a randomised controlled trial. Trials 19(1):268. https://doi.org/10.1186/s13063-018-2622-7
Tsushima T, Tsukada H, Sasaki S, Naraoka T, Yamamoto Y, Tsuda E, Ishibashi Y (2019) Biomechanical analysis of medial patellofemoral ligament reconstruction: FiberTape(R) with knotless anchors versus a semitendinosus tendon autograft with soft anchors. J Orthop Sci 24(4):663–667. https://doi.org/10.1016/j.jos.2018.11.018
Christiansen SE, Jakobsen BW, Lund B, Lind M (2008) Isolated repair of the medial patellofemoral ligament in primary dislocation of the patella: a prospective randomized study. Arthroscopy 24(8):881–887. https://doi.org/10.1016/j.arthro.2008.03.012
Petri M, Liodakis E, Hofmeister M, Despang FJ, Maier M, Balcarek P, Voigt C, Haasper C, Zeichen J, Stengel D, Krettek C, Frosch KH, Lill H, Jagodzinski M (2013) Operative vs conservative treatment of traumatic patellar dislocation: results of a prospective randomized controlled clinical trial. Arch Orthop Trauma Surg 133(2):209–213. https://doi.org/10.1007/s00402-012-1639-8
Camanho GL, Viegas Ade C, Bitar AC, Demange MK, Hernandez AJ (2009) Conservative versus surgical treatment for repair of the medial patellofemoral ligament in acute dislocations of the patella. Arthroscopy 25(6):620–625. https://doi.org/10.1016/j.arthro.2008.12.005
Dall’Oca C, Elena N, Lunardelli E, Ulgelmo M, Magnan B (2020) MPFL reconstruction: indications and results. Acta Biomed. https://doi.org/10.23750/abm.v91i4-S.9669
Wolfe S, Varacallo M, Thomas JD, Carroll JJ, Kahwaji CI (2022) Patellar instability. StatPearls, Treasure Island
Yeung M, Leblanc MC, Ayeni OR, Khan M, Hiemstra LA, Kerslake S, Peterson D (2016) Indications for medial patellofemoral ligament reconstruction: a systematic review. J Knee Surg 29(7):543–554. https://doi.org/10.1055/s-0035-1564730
Fukushima K, Horaguchi T, Okano T, Yoshimatsu T, Saito A, Ryu J (2004) Patellar dislocation: arthroscopic patellar stabilization with anchor sutures. Arthroscopy 20(7):761–764. https://doi.org/10.1016/j.arthro.2004.06.010
Hing CB, Smith TO, Donell S, Song F (2011) Surgical versus non-surgical interventions for treating patellar dislocation. Cochrane Database Syst Rev 11:CD008106. https://doi.org/10.1002/14651858.CD008106.pub2
Acknowledgements
Filippo Migliorini and Jörg Eschweiler contributed equally to the manuscript and share the first authorship.
Funding
Open Access funding enabled and organized by Projekt DEAL. No external source of funding was used.
Author information
Authors and Affiliations
Contributions
FM: literature search, data extraction, methodological quality assessment, writing, final approval; JE: literature search, data extraction, methodological quality assessment, final approval; FS: supervision, final approval; FH: supervision, final approval; MK: supervision, final approval; NM: revision, final approval. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Migliorini, F., Eschweiler, J., Spiezia, F. et al. Synthetic graft for medial patellofemoral ligament reconstruction: a systematic review. J Orthop Traumatol 23, 41 (2022). https://doi.org/10.1186/s10195-022-00660-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s10195-022-00660-9