
Abstract
Background
The reamer irrigator aspirator (RIA) is a relatively recent device that is placed in the medullary canal of long bones to harvest a large volume of bone marrow, which is collected in a filtered canister. This study compares outcomes and complications of the RIA versus a traditional iliac crest bone graft (ICBG) for the treatment of bone defects.
Methods
This meta-analysis was conducted according to the PRISMA guidelines. The Embase, Google Scholar, PubMed, and Scopus databases were accessed in June 2021. All clinical trials comparing the RIA and ICBG with a minimum of 6 months follow-up were included.
Results
Data from 4819 patients were collected. The RIA group demonstrated lower site pain (P < 0.0001), fewer infections (P = 0.001), and a lower rate of adverse events (P < 0.0001). The ICBG group demonstrated a greater rate of bone union (P < 0.0001). There was no difference between groups in VAS (P = 0.09) and mean time to union (P = 0.06).
Conclusion
The current evidence supports the use of the RIA, given its low morbidity and short learning curve.
Similar content being viewed by others


Introduction
Autologous bone grafting is a commonly performed procedure [1]. Arthrodesis, long bone nonunion, osteomyelitis, and regenerative strategies for osteochondral defects are some of the surgical procedures in which autologous bone grafting is indicated [2,3,4,5,6,7]. An iliac crest bone graft (ICBG) is commonly used to obtain autologous bone for grafting [8, 9]. Usually, a skin incision is made parallel to the iliac crest and the iliac spine is exposed subperiosteally, with the periosteum and muscle fascia on the medial edge of the crest preserved [10, 11]. This harvest typically involves a horizontal cut through the outer cortex of the iliac crest followed by the crest reflection medially, without disturbing the attachment site of the abdominal muscles [12]. After sufficient graft material has been harvested, the iliac crest is sutured [13]. Autologous crest bone grafting is not without complications, the most common being pain at the harvest site, wound infections, fractures, and hematomas [9, 14,15,16]. A relatively recent harvesting technique includes the use of the reamer irrigator aspirator (RIA) [17]. This new device has the advantage of allowing large amounts of autologous bone graft to be harvested from the medullary canal of a long bone with a lower rate of morbidities and complications [18, 19]. After introducing the RIA and performing combined reaming and aspiration, the graft is collected inside a filtered canister [20]. This technique is versatile and has a short learning curve, suggesting that it represents a valid alternative to traditional techniques [17].
This study compares the ICBG and RIA, seeking to demonstrate the noninferiority of RIA as a harvesting technique. The primary outcomes were the visual analogue scale (VAS) score and time to union. The secondary outcome includes the most common complications, such as donor site pain, fracture, infections, and hematoma/seroma.
Materials and methods
Search strategy
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the PRISMA guidelines [21]. The PICOT framework was followed:
-
P (problem): long bones non-union, arthrodesis, osteomyelitis, maxillofacial surgery;
-
I (intervention): autologous bone grafting;
-
C (comparison): RIA vs ICBG;
-
O (outcomes): PROMs, time to union, rate of union, complications;
-
T (timing): ≥ 6 months follow-up.
Data source and extraction
Two authors (FC; ET) independently performed the literature search in June 2021. PubMed and Google Scholar were accessed. Embase and Scopus were successively accessed to identify further articles. The following keywords were used in combination: “autologous,” “iliac,” “crest,” “bone,” “marrow,” “graft,” “reamer,” “irrigator,” “aspirator,” “posterior,” “anterior,” “ACBG,” “PCBG,” “ICBG,” “RIA,” “device,” “technique,” “long,” “bone,” “non-union,” “arthrodesis,” “osteomyelitis,” “PROMs,” “complications,” “morbidity,” “donor,” “site,” “surgery,” “harvesting,” “collection,” “medullary,” “canal,” and “invasiveness.” If the title and abstract matched the topic, the full-text article was accessed. The bibliographies of the full-text articles were screened for inclusion. Disagreements were resolved by a third author (**).
Eligibility criteria
All clinical studies comparing autologous crest bone grafting using the anterior or posterior harvesting technique with the RIA technique were accessed. Given the authors’ language capabilities, articles in English, German, Italian, French, and Spanish were eligible. Level I–IV evidence (according to the Oxford Centre of Evidence-Based Medicine) was considered. Only studies published in peer-reviewed journals were considered. Editorials, systematic reviews, meta-analyses, technical notes, narrative reviews, expert opinions, and letters were excluded. Animal, biomechanical, and cadaveric studies were also excluded. Only articles reporting a minimum of 6 months follow-up were included. Studies involving skeletally immature patients were not eligible. Only articles reporting quantitative data under the outcomes of interest were considered for inclusion.
Outcomes of interest
Two authors (**; **) independently performed data extraction. The following data were collected: generalities (author, year, type of study), demographic baseline (number of samples, mean age), mean follow-up, mean BMI, indication for surgical intervention (long bone nonunion, spinal surgery, osteomyelitis), and harvesting site. The following outcomes of interest were collected: visual analogue scale (VAS) and time to union (mean).
Methodological quality assessment
Methodological quality assessment was performed by a single author (**) through the Coleman Methodology Score (CMS). The CMS is a reliable and validated tool to evaluate the methodological quality of systematic reviews and meta-analyses [22]. This score analyses the included articles, evaluating the population size, length of follow-up, surgical approach, study design, description of diagnosis, surgical technique, and rehabilitation. Outcome criteria assessment and the subject selection process were also evaluated. The quality of each study was scored between 0 (poor) and 100 (excellent), with a value of > 60 considered satisfactory.
Statistical analysis
The statistical analysis was performed by a single author (**) using the IBM SPSS software, version 25. Baseline comparability was assessed through the mean difference (MD) and the unpaired t-test, with values of P > 0.1 considered satisfactory. For the noncomparative studies included in the systematic review, the MD was used for continuous variables and the odds ratio (OR) for dichotomic data. The t-test and the χ2 test were performed, respectively, with values of P < 0.05 considered statistically significant. The confidence interval (CI) was set at 95%. Comparative studies were included in the meta-analyses. The meta-analyses were performed using Review Manager 5.3 software (The Nordic Cochrane Collaboration, Copenhagen). For continuous data, the inverse variance method was used, with MD as the effect measure. For dichotomic data, the Mantel–Haenszel method was used, with OR as the effect measure. A fixed model analysis was used as default in all the comparisons. Heterogeneity was evaluated through the Higgins I2 test. I2 was interpreted according to the Cochrane Handbook for Systematic Reviews of Interventions (http://www.cochrane-handbook.org) as follows: 0–40%, poor heterogeneity; 30–60%, moderate heterogeneity; 50–90%, substantial heterogeneity; 75–100%, considerable heterogeneity. If I2 > 60%, we switched to a random model analysis. Values of P < 0.05 were considered statistically significant.
Results
Search results
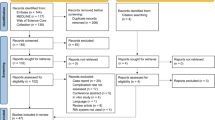
The literature search resulted in 915 articles. After the removal of duplicates (N = 400), a further 475 articles were found to be ineligible for the following reasons: study design (N = 365); language limitation (N = 17); short follow-up (N = 38); lacking quantitative data under the endpoints of interest (N = 49); cadaveric studies (N = 6). Finally, 40 comparative studies were included: one randomized controlled trial (RCT) and 10 prospective and 29 retrospective clinical studies. The literature search results are shown in Fig. 1.

Flow chart of the literature search
Methodological quality assessment
The CMS identified limitations and strengths of the present study. The study size and length of the follow-up were adequate. The surgical approach and diagnosis were well described in most articles.
Outcome measures and timing of assessment were frequently defined, providing moderate reliability. The procedures used for assessing outcomes and selecting subjects were often biased and poorly described. The CMS was 67 points, indicating that the methodological quality was fair. The CMS results are shown in Table 1.
Risk of publication bias
A funnel plot of the most commonly reported outcome (infections) was used to evaluate the risk of publication bias. The plot evidenced good symmetry, and all the referrals were located within the pyramid. Thus, the funnel plot indicated a low risk of publication bias (Fig. 2).

Funnel plot
Patient demographics
Data from 4819 patients were collected, 1908 of whom were women. There was comparability between the two groups in terms of mean age, mean BMI, and mean harvest volume. Study generalities and patient demographics are shown in detail in Table 2, while the results of the baseline comparison are reported in Table 3.
Outcomes of interest
There was no difference between the groups in terms of VAS (P = 0.09) and mean time to union (P = 0.06) (Table 4).
Complications
The RIA group demonstrated lower site pain (OR 13.2; 95% CI 8.4926–20.4135; P < 0.0001), a lower incidence of infection (OR 2.85; 95% CI 1.5060–5.4168; P = 0.001), and a lower rate of adverse events (OR 5.80; 95% CI 3.2118–10.50; P < 0.0001). The ICBG group demonstrated a greater rate of bone union (OR 17.28; 95% CI 12.8770–23.1941; P < 0.0001) compared to RIA. No difference was found in the fracture rate (P = 0.7) and the hematoma/seroma rate (P = 0.4). These results are shown in detail in Table 5.
Meta-analyses
Six studies that directly compared the RIA to ICBG were included in the meta-analysis [2, 17, 23,24,25,26]. A total of 487 patients were included, 213 of whom were female. The mean follow-up was 12.5 ± 0.7 months. The mean age was 46.8 ± 5.8, and the mean BMI was 27.6 ± 3.1 kg/m2. Comparability was found at baseline in terms of age and BMI (P > 0.1). Similarity was found in the length of the surgical intervention (P = 0.07), the transfusion rate (P = 1.0), the fracture rate (P = 1.0), the hematoma rate (P = 0.6), and the union rate (P = 0.4). The RIA demonstrated lower painful harvest site (OR 0.17; 95%CI 0.03–0.95; P = 0.04) and infection (OR 0.29; 95%CI 0.09–0.90; P = 0.03) rates. These results are shown in greater detail in Fig. 3.

Meta-analyses
Discussion
According to the main findings of the present study, the RIA was associated with less morbidity than the ICBG. There was no difference in terms of VAS and mean time to union between the two groups. The RIA demonstrated a lower incidence of harvest site pain, with only 22 of 481 patients reporting this symptom, in contrast to the ICBG cohort, for which there were 674 cases of site pain in 1742 patients. Belthur et al. [17] investigated the intensity and frequency of donor site pain. In the first 48 postoperative hours, the total pain score was higher for the ICBG than for the RIA cohort; in the period between 48 h and three months postoperatively, site pain was lower in the RIA group; after three months, the RIA group did not report donor site pain, unlike the ICBG group [17]. Donor site pain is one of the most common complications in all bone marrow harvesting procedures [16, 27,28,29,30]. Moreover, the ICBG procedure may impair sexual function, limit daily activities, and expose patients to infections [31,32,33,34]. Calori et al. reported no site infections in the RIA cohort (0/35) but a site infection rate of 14% (5/35) in the ICBG group [2]. Similarly, Belthur et al. noted that there were no infections in the RIA group (0/41) but that 8% (3/40) of the donor sites were infected in the ICBG cohort [17].
No difference was found between the groups in fracture or hematoma/seroma occurrence. The groups were similar in terms of surgery duration and transfusion rate, although the RIA is often reported in the literature to produce greater blood loss [2, 18, 26]. Overall, the adverse event rate was lower in the RIA cohort. Regarding the union rate, our results are controversial. Although the overall union rate was statistically significantly greater in the ICBG cohort (88.3% versus 81.6%), the meta-analysis of comparative studies demonstrated no significant difference between the cohorts. In this context, our findings are not fully generalizable, and no reliable conclusions can be inferred. The current evidence is controversial. Dawson et al. reported a higher union rate in the ICBG cohort compared to the RIA group [24]. Carlock et al. reported a high union rate after ICBG, with 232 unions in 242 treated patients [35]. Furthermore, On Salawu et al. reported a higher union rate following ICBG, with 81 unions in 86 patients [36]. In this regard, the data in the literature are controversial, because the RIA group is characterized by a higher union rate [17, 25]. Han et al. reported 50 unions in 57 patients after the RIA procedure [18]. Kanakaris and colleagues reported 41 unions in 42 procedures after RIA [37]. Conversely, Le Baron et al. reported nearly the same union rates in these two groups [23]. Dimitriou et al. compared the main complications after RIA use or after autologous crest bone grafting, and described two different access sites on the iliac crest: anterior and posterior [14]. The use of the RIA as a harvesting method seems to be characterized by lower rates of infection, hematoma formation, and fracture [14]. Cox et al. reported that the RIA appears relatively safe, with a lower morbidity rate than ICBG. Moreover, when complications occur, patients treated with the RIA respond better than those treated with an ICBG [38].
Our study is not free of limitations. The retrospective design of most of the included studies is an important limitation. Unfortunately, only one study was a randomized clinical trial [24], which represents an important source of selection bias. The postoperative rehabilitation was seldom described, and the follow-up was limited in most of the studies. The description of the surgical technique used was fair in several studies, representing a further limitation. Given the limited data available, and to increase the data pooling, anterior and posterior iliac crest bone grafting were not analyzed separately. However, previous evidence demonstrated that posterior and anterior ICBG produce similar outcomes [8, 9]. Finally, it is strongly recommended that further high-quality clinical trials that provide long-term follow-up should be performed to establish whether RIA can be considered the new gold standard.
Conclusion
Current evidence supports the use of the RIA, given its lower morbidity and shorter learning curve than ICBG. The RIA should become the new gold standard technique for bone marrow harvesting, but other clinical studies with long follow-ups are needed to prove it.
Availability of data and materials
The data underlying this article are available in the article and in its online supplementary material.
Abbreviations
- RIA:
-
Reamer irrigator aspirator
- ICBG:
-
Iliac crest bone graft
- BMI:
-
Body mass index
- VAS:
-
Analogue scale
- CMS:
-
Coleman Methodology Score
- MD:
-
Mean difference
- OR:
-
Odds ratio
- CI:
-
Confidence interval (CI)
References
Sen MK, Miclau T (2007) Autologous iliac crest bone graft: should it still be the gold standard for treating nonunions? Injury 38(Suppl 1):S75–80. https://doi.org/10.1016/j.injury.2007.02.012
Calori GM, Colombo M, Mazza EL, Mazzola S, Malagoli E, Mineo GV (2014) Incidence of donor site morbidity following harvesting from iliac crest or RIA graft. Injury 45(Suppl 6):S116–120. https://doi.org/10.1016/j.injury.2014.10.034
Qvick LM, Ritter CA, Mutty CE, Rohrbacher BJ, Buyea CM, Anders MJ (2013) Donor site morbidity with reamer-irrigator-aspirator (RIA) use for autogenous bone graft harvesting in a single centre 204 case series. Injury 44(10):1263–1269. https://doi.org/10.1016/j.injury.2013.06.008
Migliorini F, Eschweiler J, Maffulli N, Schenker H, Baroncini A, Tingart M, Rath B (2021) Autologous matrix-induced chondrogenesis (AMIC) and microfractures for focal chondral defects of the knee: a medium-term comparative study. Life (Basel) 11(3). doi:https://doi.org/10.3390/life11030183
Migliorini F, Eschweiler J, Maffulli N, Schenker H, Driessen A, Rath B, Tingart M (2021) Autologous matrix induced chondrogenesis (AMIC) compared to microfractures for chondral defects of the talar shoulder: a five-year follow-up prospective cohort study. Life (Basel) 11(3). doi:https://doi.org/10.3390/life11030244
Migliorini F, Eschweiler J, Maffulli N, Driessen A, Rath B, Tingart M, Schenker H (2021) Management of patellar chondral defects with autologous matrix induced chondrogenesis (AMIC) compared to microfractures: a four years follow-up clinical trial. Life (Basel) 11(2):183. https://doi.org/10.3390/life11020141
Migliorini F, Maffulli N, Baroncini A, Knobe M, Tingart M, Eschweiler J (2021) Matrix-induced autologous chondrocyte implantation versus autologous matrix-induced chondrogenesis for chondral defects of the talus: a systematic review. Br Med Bull 138(1):144–154. https://doi.org/10.1093/bmb/ldab008
Younger EM, Chapman MW (1989) Morbidity at bone graft donor sites. J Orthop Trauma 3(3):192–195. https://doi.org/10.1097/00005131-198909000-00002
Ahlmann E, Patzakis M, Roidis N, Shepherd L, Holtom P (2002) Comparison of anterior and posterior iliac crest bone grafts in terms of harvest-site morbidity and functional outcomes. J Bone Joint Surg Am 84(5):716–720. https://doi.org/10.2106/00004623-200205000-00003
Meeder PJ, Eggers C (1994) Techniques for obtaining autogenous bone graft. Injury 25(Suppl 1):A5–16. https://doi.org/10.1016/0020-1383(94)90255-0
Myeroff C, Archdeacon M (2011) Autogenous bone graft: donor sites and techniques. J Bone Joint Surg Am 93(23):2227–2236. https://doi.org/10.2106/JBJS.J.01513
Ebraheim NA, Elgafy H, Xu R (2001) Bone-graft harvesting from iliac and fibular donor sites: techniques and complications. J Am Acad Orthop Surg 9(3):210–218. https://doi.org/10.5435/00124635-200105000-00007
Ilankovan V, Stronczek M, Telfer M, Peterson LJ, Stassen LF, Ward-Booth P (1998) A prospective study of trephined bone grafts of the tibial shaft and iliac crest. Br J Oral Maxillofac Surg 36(6):434–439. https://doi.org/10.1016/s0266-4356(98)90459-4
Dimitriou R, Mataliotakis GI, Angoules AG, Kanakaris NK, Giannoudis PV (2011) Complications following autologous bone graft harvesting from the iliac crest and using the RIA: a systematic review. Injury 42(Suppl 2):S3-15. https://doi.org/10.1016/j.injury.2011.06.015
Arrington ED, Smith WJ, Chambers HG, Bucknell AL, Davino NA (1996) Complications of iliac crest bone graft harvesting. Clin Orthop Relat Res 329:300–309. https://doi.org/10.1097/00003086-199608000-00037
Almaiman M, Al-Bargi HH, Manson P (2013) Complication of anterior iliac bone graft harvesting in 372 adult patients from May 2006 to May 2011 and a literature review. Craniomaxillofac Trauma Reconstr 6(4):257–266. https://doi.org/10.1055/s-0033-1357510
Belthur MV, Conway JD, Jindal G, Ranade A, Herzenberg JE (2008) Bone graft harvest using a new intramedullary system. Clin Orthop Relat Res 466(12):2973–2980. https://doi.org/10.1007/s11999-008-0538-3
Han F, Peter L, Lau ET, Thambiah J, Murphy D, Kagda FH (2015) Reamer irrigator aspirator bone graft harvesting: complications and outcomes in an Asian population. Injury 46(10):2042–2051. https://doi.org/10.1016/j.injury.2015.07.027
Becker ST, Warnke PH, Behrens E, Wiltfang J (2011) Morbidity after iliac crest bone graft harvesting over an anterior versus posterior approach. J Oral Maxillofac Surg 69(1):48–53. https://doi.org/10.1016/j.joms.2010.05.061
McCall TA, Brokaw DS, Jelen BA, Scheid DK, Scharfenberger AV, Maar DC, Green JM, Shipps MR, Stone MB, Musapatika D, Weber TG (2010) Treatment of large segmental bone defects with reamer-irrigator-aspirator bone graft: technique and case series. Orthop Clin North Am 41(1):63–73. https://doi.org/10.1016/j.ocl.2009.08.002
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hrobjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71. https://doi.org/10.1136/bmj.n71
Coleman BD, Khan KM, Maffulli N, Cook JL, Wark JD (2000) Studies of surgical outcome after patellar tendinopathy: clinical significance of methodological deficiencies and guidelines for future studies. Victorian Institute of Sport Tendon Study Group. Scand J Med Sci Sports 10(1):2–11. https://doi.org/10.1034/j.1600-0838.2000.010001002.x
Le Baron M, Vivona JP, Maman P, Volpi R, Flecher X (2019) Can the reamer/irrigator/aspirator system replace anterior iliac crest grafting when treating long bone nonunion? Orthop Traumatol Surg Res 105(3):529–533. https://doi.org/10.1016/j.otsr.2018.12.011
Dawson J, Kiner D, Gardner W 2nd, Swafford R, Nowotarski PJ (2014) The reamer-irrigator-aspirator as a device for harvesting bone graft compared with iliac crest bone graft: union rates and complications. J Orthop Trauma 28(10):584–590. https://doi.org/10.1097/BOT.0000000000000086
Nodzo SR, Kaplan NB, Hohman DW, Ritter CA (2014) A radiographic and clinical comparison of reamer-irrigator-aspirator versus iliac crest bone graft in ankle arthrodesis. Int Orthop 38(6):1199–1203. https://doi.org/10.1007/s00264-014-2348-4
Marchand LS, Rothberg DL, Kubiak EN, Higgins TF (2017) Is this autograft worth it?: The blood loss and transfusion rates associated with reamer irrigator aspirator bone graft harvest. J Orthop Trauma 31(4):205–209. https://doi.org/10.1097/BOT.0000000000000811
DeOrio JK, Farber DC (2005) Morbidity associated with anterior iliac crest bone grafting in foot and ankle surgery. Foot Ankle Int 26(2):147–151. https://doi.org/10.1177/107110070502600206
Pollock R, Alcelik I, Bhatia C, Chuter G, Lingutla K, Budithi C, Krishna M (2008) Donor site morbidity following iliac crest bone harvesting for cervical fusion: a comparison between minimally invasive and open techniques. Eur Spine J 17(6):845–852. https://doi.org/10.1007/s00586-008-0648-3
Goulet JA, Senunas LE, DeSilva GL, Greenfield ML (1997) Autogenous iliac crest bone graft. Complications and functional assessment. Clin Orthop Relat Res 339:76–81. https://doi.org/10.1097/00003086-199706000-00011
Westrich GH, Geller DS, O’Malley MJ, Deland JT, Helfet DL (2001) Anterior iliac crest bone graft harvesting using the corticocancellous reamer system. J Orthop Trauma 15(7):500–506. https://doi.org/10.1097/00005131-200109000-00007
Beirne JC, Barry HJ, Brady FA, Morris VB (1996) Donor site morbidity of the anterior iliac crest following cancellous bone harvest. Int J Oral Maxillofac Surg 25(4):268–271. https://doi.org/10.1016/s0901-5027(06)80053-6
Dimar JR 2nd, Glassman SD, Burkus JK, Pryor PW, Hardacker JW, Carreon LY (2009) Two-year fusion and clinical outcomes in 224 patients treated with a single-level instrumented posterolateral fusion with iliac crest bone graft. Spine J 9(11):880–885. https://doi.org/10.1016/j.spinee.2009.03.013
Silber JS, Anderson DG, Daffner SD, Brislin BT, Leland JM, Hilibrand AS, Vaccaro AR, Albert TJ (2003) Donor site morbidity after anterior iliac crest bone harvest for single-level anterior cervical discectomy and fusion. Spine (Phila Pa 1976) 28(2):134–139. https://doi.org/10.1097/00007632-200301150-00008
Schnee CL, Freese A, Weil RJ, Marcotte PJ (1997) Analysis of harvest morbidity and radiographic outcome using autograft for anterior cervical fusion. Spine (Phila Pa 1976) 22(19):2222–2227. https://doi.org/10.1097/00007632-199710010-00005
Carlock KD, Hildebrandt KR, Konda SR, Egol KA (2019) Autogenous iliac crest bone grafting for the treatment of fracture nonunion is equally effective in elderly and nonelderly patients. J Am Acad Orthop Surg 27(18):696–703. https://doi.org/10.5435/JAAOS-D-18-00322
Salawu ON, Babalola OM, Ahmed BA, Ibraheem GH, Kadir DM (2017) Comparative study of proximal tibia and iliac crest bone graft donor sites in treatment of orthopaedic pathologies. Malays Orthop J 11(2):15–19. https://doi.org/10.5704/MOJ.1707.011
Kanakaris NK, Morell D, Gudipati S, Britten S, Giannoudis PV (2011) Reaming irrigator aspirator system: early experience of its multipurpose use. Injury 42(Suppl 4):S28-34. https://doi.org/10.1016/S0020-1383(11)70009-2
Cox G, Jones E, McGonagle D, Giannoudis PV (2011) Reamer-irrigator-aspirator indications and clinical results: a systematic review. Int Orthop 35(7):951–956. https://doi.org/10.1007/s00264-010-1189-z
Banwart JC, Asher MA, Hassanein RS (1995) Iliac crest bone graft harvest donor site morbidity. A statistical evaluation. Spine (Phila Pa 1976) 20(9):1055–1060. https://doi.org/10.1097/00007632-199505000-00012
Burstein FD, Simms C, Cohen SR, Work F, Paschal M (2000) Iliac crest bone graft harvesting techniques: a comparison. Plast Reconstr Surg 105(1):34–39. https://doi.org/10.1097/00006534-200001000-00006
Conway JD, Shabtai L, Specht SC, Herzenberg JE (2014) Sequential harvesting of bone graft from the intramedullary canal of the femur. Orthopedics 37(9):e796-803. https://doi.org/10.3928/01477447-20140825-56
David R, Folman Y, Pikarsky I, Leitner Y, Catz A, Gepstein R (2003) Harvesting bone graft from the posterior iliac crest by less traumatic, midline approach. J Spinal Disord Tech 16(1):27–30. https://doi.org/10.1097/00024720-200302000-00005
Delawi D, Dhert WJ, Castelein RM, Verbout AJ, Oner FC (2007) The incidence of donor site pain after bone graft harvesting from the posterior iliac crest may be overestimated: a study on spine fracture patients. Spine (Phila Pa 1976) 32(17):1865–1868. https://doi.org/10.1097/BRS.0b013e318107674e
Fernyhough JC, Schimandle JJ, Weigel MC, Edwards CC, Levine AM (1992) Chronic donor site pain complicating bone graft harvesting from the posterior iliac crest for spinal fusion. Spine (Phila Pa 1976) 17(12):1474–1480. https://doi.org/10.1097/00007632-199212000-00006
Finkemeier CG, Neiman R, Hallare D (2010) RIA: one community’s experience. Orthop Clin North Am 41(1):99–103. https://doi.org/10.1016/j.ocl.2009.07.007
Haubruck P, Ober J, Heller R, Miska M, Schmidmaier G, Tanner MC (2018) Complications and risk management in the use of the reaming-irrigator-aspirator (RIA) system: RIA is a safe and reliable method in harvesting autologous bone graft. PLoS ONE 13(4):e0196051. https://doi.org/10.1371/journal.pone.0196051
Hill NM, Horne JG, Devane PA (1999) Donor site morbidity in the iliac crest bone graft. Aust N Z J Surg 69(10):726–728. https://doi.org/10.1046/j.1440-1622.1999.01674.x
Kim DH, Rhim R, Li L, Martha J, Swaim BH, Banco RJ, Jenis LG, Tromanhauser SG (2009) Prospective study of iliac crest bone graft harvest site pain and morbidity. Spine J 9(11):886–892. https://doi.org/10.1016/j.spinee.2009.05.006
Kusnezov N, Prabhakar G, Dallo M, Thabet AM, Abdelgawad AA (2017) Bone grafting via reamer-irrigator-aspirator for nonunion of open Gustilo–Anderson type III tibial fractures treated with multiplanar external fixator. SICOT J 3:30. https://doi.org/10.1051/sicotj/2017002
Loeffler BJ, Kellam JF, Sims SH, Bosse MJ (2012) Prospective observational study of donor-site morbidity following anterior iliac crest bone-grafting in orthopaedic trauma reconstruction patients. J Bone Joint Surg Am 94(18):1649–1654. https://doi.org/10.2106/JBJS.K.00961
Merritt AL, Spinnicke A, Pettigrew K, Alamin TF (2010) Gluteal-sparing approach for posterior iliac crest bone graft: description of a new technique and assessment of morbidity in ninety-two patients after spinal fusion. Spine (Phila Pa 1976) 35(14):1396–1400. https://doi.org/10.1097/BRS.0b013e3181cabf69
Metsemakers WJ, Claes G, Terryn PJ, Belmans A, Hoekstra H, Nijs S (2019) Reamer-irrigator-aspirator bone graft harvesting for treatment of segmental bone loss: analysis of defect volume as independent risk factor for failure. Eur J Trauma Emerg Surg 45(1):21–29. https://doi.org/10.1007/s00068-017-0821-7
Mirovsky Y, Neuwirth MG (2000) Comparison between the outer table and intracortical methods of obtaining autogenous bone graft from the iliac crest. Spine (Phila Pa 1976) 25(13):1722–1725. https://doi.org/10.1097/00007632-200007010-00018
Robertson PA, Wray AC (2001) Natural history of posterior iliac crest bone graft donation for spinal surgery: a prospective analysis of morbidity. Spine (Phila Pa 1976) 26(13):1473–1476. https://doi.org/10.1097/00007632-200107010-00018
Schizas C, Triantafyllopoulos D, Kosmopoulos V, Stafylas K (2009) Impact of iliac crest bone graft harvesting on fusion rates and postoperative pain during instrumented posterolateral lumbar fusion. Int Orthop 33(1):187–189. https://doi.org/10.1007/s00264-007-0446-2
Schwartz CE, Martha JF, Kowalski P, Wang DA, Bode R, Li L, Kim DH (2009) Prospective evaluation of chronic pain associated with posterior autologous iliac crest bone graft harvest and its effect on postoperative outcome. Health Qual Life Outcomes 7:49. https://doi.org/10.1186/1477-7525-7-49
Acknowledgements
None.
Funding
Open Access funding enabled and organized by Projekt DEAL. No external source of funding was used.
Author information
Authors and Affiliations
Contributions
FM: conception and design of the study, literature search, data extraction, methodological quality assessment, writing, analysis, interpretation of data, and final approval; FC: literature search, data extraction, methodological quality assessment, writing, and final approval; NM: revision and final approval; FO, FH: supervision, final approval. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Oliva, F., Migliorini, F., Cuozzo, F. et al. Outcomes and complications of the reamer irrigator aspirator versus traditional iliac crest bone graft harvesting: a systematic review and meta-analysis. J Orthop Traumatol 22, 50 (2021). https://doi.org/10.1186/s10195-021-00612-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s10195-021-00612-9