
Abstract
Background
In the last 10 years, the rate of femur fractures treated within 48 h from trauma has been introduced as a performance index for hospital management in Italy. Literature showed a significant indirect correlation between early treatment and mortality/comorbidity. The aims of early treatment are pain management and reduction of time to ambulation. The purpose of this study is to evaluate whether early treatment has reduced time to ambulation in femur fracture.
Materials and methods
All patients admitted to two level I trauma centers with proximal femoral fracture between 1/1/2017 and 31/12/2017 were included in this study. Exclusion criteria were patient age younger than 65 years, death before surgery, and nonsurgical treatment. The following data were collected: age, gender, date and time of admission to emergency department, height, weight, body mass index (BMI), type and side of fracture, American Society of Anesthesiologists (ASA) score, date and time of surgery, surgical time, length of hospitalization, death during hospitalization, time from surgery to physiotherapy start, and time from surgery to first walking day.
Results
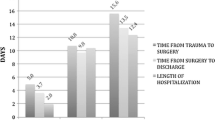
The study sample resulted in 660 patients. Mean age was 82 years, 64 % were female, mean BMI was 24 kg/m2, mean ASA score was 2.7, and 42 % were medial fractures. Mean time from admission to surgery was 95 h; 49.8 % were treated within the first 48 h. Mean time from surgery to physiotherapy start was 2 days, 21 % were not able to walk during hospitalization, time from surgery to first walking day was 5 days, and mean hospitalization time was 15 days. Early surgery was significantly (p = 0.008) associated with the probability of ambulation recovery during hospitalization. No association (p = 0.513) was found between early surgery and time in bed without walking.
Conclusions
Early surgery in femur fracture became a priority in the health system. However, according to our data, although 51 % of patients were treated within the first 48 h, time from surgery to physiotherapy start (2 days) was still too long. Furthermore, time from surgery to first walking day was 6 days, longer than in most published papers. These data suggest that the performance index (rate of femur fractures treated within 48 h) may be improved by changing it to rate of femur fractures surgically treated with return to walking in 96 h.
Level of evidence
Level 4 (retrospective study).
Similar content being viewed by others

Introduction
Hip fractures in the elderly will increase greatly in the coming decades due to aging of the population [1, 2]. Evidence suggests that surgery is the most effective treatment for femur fracture, and recent guidelines assess that early surgical treatment reduces mortality and complications [3,4,5,6,7]. Several published papers have suggested a cutoff of 48 h for operation [5]. The aims of early treatment are pain management and to reduce time to ambulation. Since 2008, the Ministry of Health in Italy has introduced the rate of femur fracture treated within 48 h as one of the indicators of hospital efficiency [8]. The aim of this study is to evaluate whether early treatment reduced time to ambulation in femur fracture.
Materials and methods
Settings
All patients admitted to two level I trauma centers with proximal femoral fracture between 1/1/2017 and 31/12/2017 were included in this study. Exclusion criteria included patient age younger than 65 years, death before surgery, and nonsurgical treatment.
Data collection
Hospital charts were retrospectively reviewed after patients had given informed consent for use of their data. The present study was approved by the Institutional Review Board and was conducted in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. The following data were collected: age at admission, gender, date and time of admission to emergency department (ER), height, weight, body mass index (BMI) [9], type of fracture (pertrochanteric, subtrochanteric, basicervical, subcapital, transcervical; then grouped into intracapsular or extracapsular), side of fracture (right or left), American Society of Anesthesiologists (ASA) score [10], date and time of surgery, surgical time, length of hospitalization, death during hospitalization, time from surgery to physiotherapy start, time from surgery to first walking day, and time from physiotherapy start to first ambulation (including and excluding weekends and public holidays).
Patients were also divided into two groups according to early (within 48 h) or delayed (> 48 h) surgical treatment in order to evaluate whether early surgery (among other factors) was significantly related to early recovery of ambulation and to time from surgery to first walking day. All data were analyzed using standard descriptive statistics. The data for the two trauma centers were compared using the chi-squared test or Fisher’s exact test for categorical outcomes, and Student’s t test or Mann–Whitney test for continuous outcomes. The Kolmogorov–Smirnov test was used to determine whether data were normally distributed. p-Values lower than 0.05 were considered statistically significant. All analyses were performed using Stata version 12 (Stata Corporation, College Station, TX, USA).
Results
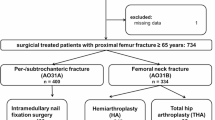
Out of 785 patients (636 from trauma center I, 149 from trauma center II), 125 were excluded (71 younger than 65 years, 48 nonsurgical treatment, 3 death before surgery, and 3 incomplete data). Therefore, the study sample resulted in 660 patients (516 from trauma center I, 144 from trauma center II). Table 1 presents baseline data, while Table 2 presents timing, ability to walk before discharge, and mortality.. Among patients who walked again after surgery, 54 % were operated within 48 h from admission, while 46 % were operated after 48 h. Among patients who did not walked again after surgery, 41 % were operated within 48 h from admission, while 59 % were operated after 48 h. The data show a decreasing trend in reaching ambulation among patients operated after 48 h from admission, with a statistically significant association (p = 0.008, Pearson correlation coefficient).
Patients who underwent operation within 48 h from admission started to walk again after 5.4 days on average, versus 5.9 days for patients operated later than 48 h from admission, albeit without a statistically significant association (p = 0.0658, Mann–Whitney test).
Comparing the two trauma centers (Table 3), no significant differences emerged regarding demographic data (age, sex, BMI, ASA score). Even if there were significant differences in favor of trauma center I in terms of length of hospitalization (p = 0.001) and the rate of patients treated in the first 48 h (p = 0.002), there were no differences considering the time between surgery and start of physiotherapy (p = 0.838), time between surgery and start of ambulation (p = 0.846), or probability of walking again after surgery (p = 0.185).
Discussion
The main purpose of this study is to evaluate whether early surgery of femoral fracture influences early recovery of ambulation in elderly people.
The data, like in other studies [11], show that early surgery significantly increases the probability of ambulation recovery but is not significantly correlated with faster recovery of ambulation.
This finding may be explained by poor attention to a fast and effective rehabilitation protocol: our study shows that recovery of ambulation takes significantly longer than the average results found in literature. In our study, patients experienced an average of 5.2 days of immobility, while in the majority of studies found in literature the average is 2 days [12,13,14], with only the study by Siu et al. [15] showing results comparable to ours. More importantly, our study did not show any significant differences between the two trauma centers in terms of either time between surgery and start of physiotherapy or time between surgery and start of ambulation.
Even if there is no clear and structured protocol to improve mobility after surgery for femoral fracture (Cochrane Review, Handoll [16], AAOS), numerous international guidelines (NICE [17], SIGN [18], NZGG, SEGG-SECOT, and GEIOS [19]) recommend that mobilization start on the day of the operation or the day after. A prospective study by Koval et al. [20] investigated the effects of immediate unrestricted weight bearing after femoral fracture; the results supported its application, since it was not associated with an increase of comorbidities.
The results of another prospective study by Siu et al. [15] showed that early ambulation is associated with a better outcome in terms of 6-month mortality, with a greater benefit for more vulnerable patients. The effect of immobility was mediated largely by postoperative delay. Furthermore, in a trial by Marcantonio et al. [21], early ambulation was associated with lower incidence of delirium, along with other determining factors.
Comparison of our results with existing literature highlights how early recovery of ambulation depends mostly on hospital protocols for rehabilitation and how early ambulation could lead to a reduction of hospitalization time and fewer nosocomial comorbidities [22, 23]. Our study provides an interesting analysis on this topic, based on data from a significant number of patients coming from two major trauma centers. Based on these results and the analogies between the two centers, it can be asserted that the question of early recovery of ambulation plays an important role not only at the local or regional scale, but presumably at the national scale. Consequently, this study highlights the importance of and necessity for appropriate and efficient organization of rehabilitation [24], which can lead to a great reduction of the duration of hospitalization and a smaller number of nosocomial comorbidities.
This study is limited by its retrospective design; furthermore, only patients and hospitals from a single European country were included, thus findings may not be generalizable to other geographical regions. Another limitation is the absence of data regarding the walking ability of the patients before trauma. Also, this study lacks clinical follow-up to understand whether its conclusions are also supported by the mortality rate.
Our results suggest that, even if early surgery increases the probability of walking again after femur fracture, it is not the only factor influencing the time between surgery and first walking day. Our data suggest that, although 51 % of patients were operated within 48 h, both the time between surgery and start of physiotherapy (median 2 days) and the time between surgery and recovery of ambulation (5–6 days) were above expectations and above the average results published in literature (2–3 days). Nonmedical issues largely influenced the time from surgery to physiotherapy start and from surgery to first walking day. In conclusion, we think that a direct connection between physiotherapist and orthopedic communities should be established to reduce these timings, and the performance indicator of the rate of fractures operated within 48 h should be improved, possibly by converting it to the rate of patients who are operated and start to walk again within 96 h.
Abbreviations
- ER:
-
Emergency department
- BMI:
-
Body mass index
- ASA:
-
American Society of Anesthesiologists (ASA)
References
Laforgia R, Maggi S, Marzari C, Bianchi D, Crepaldi G (2006) Epidemiology of femoral neck fracture in old people in Italy. J Bone Joint Surg Br 88(Suppl I):42
Beaupre LA, Jones CA, Saunders LD, Johnston DW, Buckingham J, Majumdar SR (2005) Best practices for elderly hip fracture patients: a systematic overview of the evidence. J Gen Intern Med 20(11):1019–1025
Uzoigwe CE, Burnand HG, Cheesman CL, Aghedo DO, Faizi M, Middleton RG (2013) Early and ultra early surgery in hip fracture patients improves survival. Injury 44(6):726–729
Grimes JP, Gregory PM, Noveck H, Butler MS, Carson JL (2002) The effects of time-to-surgery on mortality and morbidity in patients following hip fracture. Am J Med 112(9):702–709
Simunovic N, Devereaux PJ, Sprague S, Guyatt GH, Schemitsch E, Debeer J, Bhandari M (2010) Effect of early surgery after hip fracture on mortality and complications: systematic review and meta-analysis. CMAJ 182(15):1609–1616
Bretherton CP, Parker MJ (2015) Early surgery for patients with a fracture of the hip decreases 30-day mortality. Bone Joint J 97(1):104–108
Moja L, Piatti A, Pecoraro V, Ricci C, Virgili G, Salanti G, Germagnoli L, Liberati A, Banfi G (2012) Timing matters in hip fracture surgery: patients operated within 48 hours have better outcomes. A meta-analysis and meta-regression of over 190,000 patients. PLoS ONE 7(10):e46175
Ministero della salute—Agenzia Nazionale per I Servizi Sanitari Regionali—National Outcome Evaluation Program, PNE, Italian. http://95.110.213.190/PNEed17/risultati/tipo1/intr_struasl1_HC.php?ind=42&tipo=2&area=5. Accessed 19 July 2017
BMI Body Mass Index Classification System. World Health Organization. http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi. Accessed 19 July 2017
ASA Physical Status Classification System. American Society of Anesthesiologists. https://www.asahq.org/resources/clinical-information/asa-physical-status-classification-system. Accessed 19 July 2017
Orosz GM, Magaziner J, Hannan EL, Morrison RS, Koval K, Gilbert M, McLaughlin M, Halm EA, Wang JJ, Litke A, Silberzweig SB, Siu AL (2004) Association of timing of surgery for hip fracture and patient outcomes. JAMA 291(14):1738–1743
Barone A, Giusti A, Pizzonia M, Razzano M, Oliveri M, Palummeri E, Pioli G (2009) Factors associated with an immediate weight-bearing and early ambulation program for older adults after hip fracture repair. Arch Phys Med Rehabil 90(9):1495–1498
Kamel HK, Iqbal MA, Mogallapu R, Maas D, Hoffmann RG (2003) Time to ambulation after hip fracture surgery: relation to hospitalization outcomes. J Gerontol A Biol Sci Med Sci 58(11):1042–1045
Oldmeadow LB, Edwards ER, Kimmel LA, Kipen E, Robertson VJ, Bailey MJ (2006) No rest for the wounded: early ambulation after hip surgery accelerates recovery. ANZ J Surg 76(7):607–611
Siu AL, Penrod JD, Boockvar KS, Koval K, Strauss E, Morrison RS (2006) Early ambulation after hip fracture: effects on function and mortality. Arch Intern Med 166(7):766–771
Handoll HH, Sherrington C, Mak JC (2011) Interventions for improving mobility after hip fracture surgery in adults. Cochrane Database Syst Rev 3:CD001704. https://doi.org/10.1002/14651858.CD001704.pub4
National Institute for Health and Care Excellence Clinical Guideline (2011) Hip fracture: management. NICE [CG124] Published date: June 2011, Last updated: May 2017. https://www.nice.org.uk/guidance/cg124. Accessed 19 July 2017
Scottish Intercollegiate Guidelines Network Guideline (2009) Management of hip fracture in older people. SIGN [CG111]. https://www.sign.ac.uk/sign-111-management-of-hip-fracture-in-older-people.html. Accessed 19 July 2017
Mas YB, Montalvo JIG, Soler PA, Alarcon MT (2012) Guías clínicas de fractura de cadera. Comparación de sus principales recomendaciones. Revista Española de Geriatría y Gerontología 47(5):220–227
Koval KJ, Friend KD, Aharonoff GB, Zukerman JD (1996) Weight bearing after hip fracture: a prospective series of 596 geriatric hip fracture patients. J Orthop Trauma 10(8):526–530
Marcantonio ER, Flacker JM, Wright RJ, Resnick NM (2001) Reducing delirium after hip fracture: a randomized trial. J Am Geriatr Soc 49(5):516–522
Chua MJ, Hart AJ, Mittal R, Harris IA, Xuan W, Naylor JM (2017) Early mobilisation after total hip or knee arthroplasty: a multicentre prospective observational study. PLoS ONE 12(6):e0179820
Masaracchio M, Hanney WJ, Liu X, Kolber M, Kirker K (2017) Timing of rehabilitation on length of stay and cost in patients with hip or knee joint arthroplasty: a systematic review with meta-analysis. PLoS ONE 12(6):e0178295
Aprato A, Longo D, Giachino M, Agati G, Massè A (2017) Should hospital managers read the orthopedic literature before surgeons? The example of femur fracture management. J Orthop Traumatol 18(2):107–110
Authors’ contributions
A.A. and A.M. conceived the study. A.C., G.P., M.B., C.G., and A.S. collected the data. A.A. was involved in the conception and design of the study, oversaw, and provided quality assurance on all study output. All patients included in this study were operated on by the groups directed by A.M. and D.C. A.C. and G.P. were involved in the conception and design of the study and drafted the manuscript. M.B., C.G., and A.S. collected the patient data and assisted in revising the manuscript. All authors read and approved the final manuscript.
Acknowledgements
The authors thank Mrs. Laura Rossi for support.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
A paper copy of the database is available at Città della Salute e della Scienza di Torino.
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Funding
No funding has been received for this study.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Aprato, A., Casiraghi, A., Pesenti, G. et al. 48 h for femur fracture treatment: are we choosing the wrong quality index?. J Orthop Traumatol 20, 11 (2019). https://doi.org/10.1186/s10195-019-0518-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s10195-019-0518-2