
Abstract
Current definitions of migraine that are based mainly on clinical characteristics do not account for other patient’s features such as those related to an impaired quality of life, due to loss of social life and productivity, and the differences related to the geographical distribution of the disease and cultural misconceptions which tend to underestimate migraine as a psychosocial rather than neurobiological disorder.
Global differences definition, care access, and health equity for headache disorders, especially migraine are reported in this paper from a collaborative group of the editorial board members of the Journal of Headache and Pain. Other components that affect patients with migraine, in addition to the impact promoted by the migraine symptoms such as stigma and social determinants, are also reported.
Similar content being viewed by others


Introduction
Migraine is a complex neurological disorder that involves not only neurobiological symptoms but also multiple domains for each patient (e.g. psychosocial, personal and economic). Current definitions of migraine are based on the occurrence of attacks of moderate to severe, throbbing and pulsating pain on one side of the head, exacerbated by physical exercise and associated with nausea/vomiting and/or photo/phonophobia. This definition does not account for other patient’s features which are no less important, such as those related to an impaired quality of life due to loss of social life and productivity [1]. Also, the classic definition does not evaluate the differences related to the geographical distribution of the disease, which is not attributable only to the geographic nuances inherent in each country, but also to the differences in terms of estimation method, the definition that is used for diagnosis but also cultural misconceptions which tend to underestimate migraine as a psychosocial rather than neurobiological disorder [2].
The Global Burden of Disease (GBD) study estimates the global prevalence of migraine to be around 14% (95% CI 12.9–15.2) and of active headache disorders around 52% (48.9–55.4). The GBD 2021 study is not based on a direct data surveillance system and relies primarily on secondary data collected by a broad network of government officials, medical professionals and scientists [3]. However, the vast majority of studies have been conducted in high-income countries, therefore estimation bias can account for the difference of epidemiology across the different population groups [3].
The recent pandemic from the novel coronavirus disease 2019 (COVID-19), the introduction of effective vaccines and the recent conflict-related economic crises have contributed to change the definition of migraine from a single headache disorder to a complex multifaceted disease, and to the different geographic framework [4].
This document, written by a collaborative group of the editorial board of the Journal of Headache and Pain coming from multiple geographical areas, aims to report the differences in terms of definition, care access, and health equity for headache, especially migraine and secondary headaches. We also addressed challenges in headache medicine based on the experience of the COVID-19 pandemic. Stigma and social determinants of migraine are also described. Part 1 is an introduction to continue our discussion in Part 2, which will cover the organization of headache services with a focus on challenges in low-, middle- and high-income countries. Our other goal is the desire to draw attention to pressing issues in headache medicine and to spark academic, social, and political discussion to improve patients’ lives.
Epidemiology
Geographical/geoeconomical differences
About half of the global population is afflicted by an active headache disorder, predominantly tension-type headache (TTH) and migraine [3, 5]. Prevalence statistics, drawn from a plethora of epidemiologic studies, are nonetheless limited by methodologic issues [4]. These include differences in case definitions used, sampling method, and geographic particularities inherent in each country. An interesting observation is that migraine prevalence is reported to be highest in Nepal – a phenomenon that might be linked to the country’s altitude – and lowest in China [6, 7]. For TTH, Afghanistan and Brazil have the highest prevalence, while China has the lowest rate [6].
The geographic differences are further highlighted in the GBD study, which found a lower headache prevalence in Southeast Asia, East Asia, Oceania (SEEAO), and Sub-Saharan Africa (SSA), compared with high-income countries [6]. The latter accounts for about 15% of the global population, but most of the available epidemiological data is derived from these countries and few prevalence studies are available from low- and middle-income countries (LMIC) [3]. The underrepresentation of data from LMIC invites a measured interpretation of the prevalence estimates. This observation also highlights an urgent need for epidemiological research in LMICs.
In tandem with geographic variations in prevalence estimates, one must also account for the profound influence of geo-economic and cultural factors [5]. These forces shape societal attitudes toward headache disorders and, in part, dictate the availability, accessibility, and affordability of headache care. People in LMICs face considerable challenges related to the recognition and management of headache disorders, a struggle amplified by limited economic resources, overburdened healthcare services, and a dearth of specialized clinics [5]. Cultural misconceptions can further muddy the waters. For instance, migraine is often regarded as a psychosocial rather than neurobiological disorder in emerging economies such as China and India [8, 9]. This, in turn, hampers the delivery of appropriate treatment and allocation of adequate headache care services.
The economic ramifications of headache disorders have primarily been studied in high-income countries, with direct costs for migraine management exceeding $1000 per person per year [10, 11]. It is also worth mentioning that indirect costs due to productivity losses are more than double [10, 12, 13]. Unfortunately, comparable data for LMICs is conspicuously sparse. Available estimates from nations like Russia, Zambia, and China hint at a similar economic burden, with indirect costs amounting to about 2% of their Gross Domestic Product [14,15,16].
Cost-efficiency can be improved through strategic reorientation of healthcare resources towards headache management, complemented by education interventions, especially in low- and middle-countries [5], where the self-management with simple analgesics has been by far the most cost-effective strategy for migraine treatment and represents a highly efficient use of health resources. Predictive modeling for China, India, Russia, and Zambia suggests that acute treatments using simple analgesics might offer the greatest cost-benefits among all therapeutic interventions [17].
To confront the geographic and geo-economic disparities in headache care, a thorough overhaul of existing healthcare policies and an increased allocation of resources for headache disorders in LMICs is much needed. This recalibration, aimed at improving patient outcomes and reducing the economic burden, should incorporate the development of sustainable healthcare models that prioritize comprehensive management of headache disorders.
Environmental and occupational issues based on the example of the COVID-19 pandemic
Headache and pandemics/syndemics
The recent widespread diffusion of a novel coronavirus (SARS-CoV-2) has radically changed the epidemiological, clinical and diagnostic scenario of several disorders, especially headache [18]. In the context of the pandemic from the novel coronavirus disease 2019 (COVID-19), headache can be a clinical manifestation of the acute form of the disease, or the persistent, difficult-to-treat and disabling symptom of post-acute sequelae of SARS-CoV-2 infection (also known as long COVID headache) or can act as comorbidity with COVID-19, with a synergy effect on clinical picture in term of intensity of pain and refractoriness to the treatment [19, 20]. The different geographical spread of the pandemic, at least in the first wave, has modified the different geographical distribution of symptoms such as headache, resulting in a higher prevalence of headache also in countries where the prevalence was lower before the pandemic (e.g. China) [21]. The aggregation of two or more disease clusters is defined as syndemic and the synergistic epidemic effect has a significant impact on biological and prognostic consequences and the whole disease burden, for almost all disorders and headache and related pain syndromes are not spared from this phenomenon [22].
Several data report how patients with migraine and co-infection from SARS-CoV-2 complain of more intense pain which is often less responsive to common analgesics [23]. Patients with a migraine history and a migraine-like phenotype can respond well to triptans, while those with a TTH-like phenotype can be improved by single doses of paracetamol [24]. A good response rate in term of pain relief has been obtained with indomethacin in patients with the migraine-like phenotype, however several side effects are associated with its long-term use (e.g. cardio and nephrotoxicity) limits significantly the prescription in the daily routine [25]. In long COVID, the use of prophylactic drugs such as amitriptyline has been associated with a significant reduction of migraine crises in 44% of cases, therefore its use has been recommended in those patients experiencing 4 or more headache days per month [26]. Few evidence is showing a good response rate to the sphenopalatine ganglion block in terms of headache days reduction however the very limited data does not recommend its use in the daily routine [27].
The recent introduction of migraine prevention drugs such as those targeting the Calcitonin Gene Related Peptide (CGRP), has given new options for the treatment of migraine. However, due to the high cost and low availability in all countries, their use is limited to the cases that are refractory to the other preventive treatments for at least 8 weeks of therapy and actually they are available only in high-income countries [28, 29]. CGRP mAbs treatment is not associated with the risk of severe COVID-19 outcomes or positive results at the SARS-CoV-2 test therefore its use is safe for migraine prevention also during the pandemic [30]. However, no studies have so far investigated to effectiveness of these drugs in long-term COVID headache, therefore actual evidence derives from the migraine prevention trials during the SARS-CoV-2 pandemic [30].
While it has been established that patients with a history of migraine do not have a significant risk increase of developing COVID-19, the biological and immunological mechanisms underlying the effective interaction between the two disorders and their differences according to genetic variability across different countries are largely unknown [31]. The SARS-CoV-2 binding to the angiotensin-converting enzyme 2 (ACE2) binding from SARS-CoV-2 is associated with a reduced anti-inflammatory effect due to enzyme activity reduction, in favor of inflammatory headache [32]. Less evidence argues in favor of hypoxia, hypercapnia and of the direct neuronal tissue invasion from SARS-CoV-2 [33]. Persistent immune system activation from cytokine hyperproduction, unresolved neuronal damage or meningeal inflammation may account for the persistent headache in long COVID, and other neurological manifestations such as cognitive deficits and brain fog may be related to an glutamate hyperproduction and upregulation of N-methyl-D-aspartate (NMDA) receptors [24].
Gut dysbiosis in combination with genetic predisposition seems to modulate migraine attacks, and some theories suggest that the microbiome-gut-brain axis can link not only to neurodegenerative and neurodevelopmental diseases [34,35,36] but also to other potentially reversible neurological diseases, such as migraine and long COVID headache [36,37,38].
Promotional measures of lifestyle changes, a balanced diet and regular physical activity can modulate effectively the gut microbiota composition, but are extremely difficult to reach in low-income countries, making even more clear the geographical difference [39, 40].
COVID-19 and vaccines
Another important aspect related to the COVID-19 pandemic which has changed the phenotype of migraine in recent years has been the introduction of vaccines. At the start of pandemic, the problem has been even more complex due to the different accessibility to vaccines from the various countries. The first vaccines were introduced in mid-2020 and several formulations based on different mechanisms of action were developed [41]. Traditional vaccines contained inactivated viruses or recombinant viral vectors and more advanced vaccines were based on mRNA or viral vectors. The vast majority of adverse effects (AE) after vaccination are mild and resolve within a few days. Severe adverse reactions such as anaphylaxis, thrombosis, carditis, and severe polyneuropathy have been observed rarely [42].
A meta-analysis based on 1.57 million people showed that headaches were the third most common AE and occurred up to 7 days after vaccination. They were observed in 22% and 29% of individuals after the 1st and 2nd doses of vaccination, respectively. There was no difference in the incidence of headaches depending on the type of vaccine and the percentage of headaches after 1 dose decreased with age [43]. The phenotype of vaccine-related headache resembled migraine-like in about 30%, and the headache was throbbing with sensory hypersensitivity and intensified during physical activity. It was shown that the incidence of headache after vaccination was higher in individuals with a history of headache [44]. In a group of 841 migraine patients, it was shown that more than 60% of both the first and second doses of the vaccine were followed by a migraine attack that lasted longer, was more severe and was more refractory to treatment [45]. It has also been described as a case series of patients with cluster headache who, after a long period of remission, developed a new cluster with frequent attacks early after vaccination. In addition, the new cluster episodes occurred in them at different times of the year than usual [46] Some reports of cluster headache occurring de novo immediately after vaccination have been described [47,48,49].
In most cases, acute headache following vaccination is associated with the immune response triggered by the vaccine, and in this regard, there are more similarities than differences with post-COVID headache [50]. However, post-vaccination headaches can also be associated with severe AEs and, in certain situations, should be a red flag that may suggest secondary headaches in the course of, for example, cerebral venous thrombosis (CVT) or other thrombotic complications in the background of immune thrombocytopenia [51]. Such situations can be particularly insidious in patients with chronic headaches in whom prolonged headache after vaccination may be trivialized [50]. The widespread vaccination against SARS-CoV-2 has radically improved the outcome of patients with COVID-19 and has been associated with a significant overall reduction in mortality. The majority of side effects are mild and transient, therefore periodic vaccination against the SARS-CoV-2 virus is strongly recommended, especially in some at-risk categories of unfavorable outcomes such as immunocompromised patients and older adults [52].
Long COVID
As mentioned above, another important consequence of the pandemic is the persistence of post-COVID-19 syndrome for which the term long COVID syndrome is commonly used [53]. Despite unclear diagnostic criteria, it implies the persistence of significant symptoms from 4 to 12 weeks after an infection. Neurological symptoms are frequently observed and the most common include headache, cognitive impairment, brain fog, fatigue syndrome and neuropsychiatric disorders like depression and sleep disturbances [54,55,56]. Other symptoms include cardiovascular, pulmonary/respiratory or musculoskeletal disorders [55]. The symptoms and course of long COVID vary depending on the viral variant that caused the infection [57, 58].
Long COVID headache may manifest as either a worsening of the course of a pre-existing headache or the appearance of a new headache, which is most often accompanied by other symptoms of infection such as hyposmia or anosmia [19]. Most frequently, it has a tension-type phenotype, less often a migraine-type. It manifests with bilateral, compressive pain without additional symptoms. The new headache may be daily and persistent and its phenotype may mimic new daily persistent headache (NDPH) [59]. The presence of headache during the acute phase of infection has been associated with a better prognosis and low mortality from COVID-19. This difference most likely indicates the activation of the immune response during acute viral infection [32, 60].
Patients with a history of previous headache usually report an increase in the frequency and intensity of headaches. Furthermore, patients with refractory headache in the acute phase of infection seem to have a higher incidence of long COVID headache [61].
Long COVID symptoms are still an object of observation and scientific research because most of them require observation over time. In addition to the long COVID headache described in this chapter, post COVID symptoms can involve many systems and organs. We do not have precise data on geographical differences between long-covid symptoms. Single studies have shown no differences in the distribution of these symptoms between residents of metropolitan-urban residences and regional-urban/rural residences. To date, a worse prognosis of long COVID symptoms, especially fatigue, has been shown to correlate with age, female gender and hospitalization associated with a more severe course of the disease [21, 22, 32, 58,59,60,61].
Stigma and social determinants
Stigma
Patients with migraine quite often have to lead with more than the impact promoted by the several symptoms of the recurrent migraine attack. Migraine stigma is a common problem that adds to the suffering of this condition. Stigma can be defined as the mark or condition or status that undergoes to social devaluation, and it is described from three different perspectives: public, structural, and internalized stigma [62].
Public stigma refers to the general idea of stereotypes that circulate in a determined society in a certain period. It is revealed by several labels commonly used to describe migraine, such as malingerer, pill popper, hysterical, drug-seeking, lazy or person incapable of handling stress [63]. The idea of an easily solved disorder, that happens predominantly to wealthy women “who can afford to lie in the bed” is nourished by several cultural manifestations, from literature to pharmaceutical advertisements, and media representations [64]. There is a public conviction that people with migraine “have very little resistance, or are using it as an excuse” [65]. One of the social consequences of this misrepresentation of migraine is that the population that does not correspond to this stereotype frequently will fail to recognize the migraine symptoms in themselves, and this might delay seeking for healthcare attention [64]. Public stigma is often rooted in a lack of awareness about the condition. Public stigma is not always overt, and it can be subtle. For example, people with migraine may feel uncomfortable talking about their condition at work, because they are worried about being judged.
Structural stigma refers to the consequences imposed by migraine stigma in the social structure, such as laws and health policies. It may manifest in different structures of society. One example is the relatively limited mean time dedicated to headache training observed worldwide in medical education, which is limited to no more than 4 hours in undergraduate education, and no more than 10 hours for medical specialists [66]. Another example is the discrepancy between the prevalence and impact of migraine and the rate of funding dedicated to migraine research. In 2009, if considered the burden related to headache diseases and compared to other conditions, the funding expected by National Institute of Health (NIH) would be more than $103 million/year, whereas the amount received was between $6.8 and $13 million/year [67]. One of the consequences of this discrepancy is the lack of opportunities to develop research, and a lowering status of headache medicine in medical departments, when compared to other areas of the neurological field [64]. Structural stigma is also revealed by the low rates of search for help by migraine patients. One study evaluating patients with chronic migraine, presenting with migraine attacks for more than 15 days per month for at least 3 months, showed that no more than 40.8% of patients have ever sought healthcare attention due to the headache [68]. The workplace is a common field of structural migraine stigma. In a survey from 2016 with 4024 adults, half of those who called out of work for a headache reported they did not reveal to their supervisors the reason for absenteeism. Furthermore, half of the managers surveyed did not consider headache as an acceptable reason to leave work, showing how clear is migraine stigma in the workplace [64].
Internalized stigma in migraine is the negative perception of oneself that is held by a person with migraine. It can lead to feelings of shame, guilt, and isolation. It is a consequence of the absorption by patients with migraine of the assumptions created about their condition. Internalized stigma may impose serious consequences on patients’ self-esteem and mental health [69]. In research by Young et al. that compared the stigma between patients with epilepsy, chronic migraine, and episodic migraine, those with chronic migraine presented the most severe scores, and impaired ability to work was the strongest predictor of stigma [70]. Migraine stigma might also affect patients’ family relationships. Over a third of patients with chronic migraine reported it affected their relationship with their partner, and 71% reported that they would be better parents if they did not have headaches [71]. One of the worst consequences of the internalized stigma is the impairment of the ability to recognize migraine as a disease and seek help.
Migraine stigma is also affected by the gender gap, imposing on women a disproportionately higher burden than men, and not only because of the higher prevalence. Often women are taken less seriously by healthcare providers, and headache might be “psychologized”. Women have less access to adequate treatment and are more likely to report medication overuse headache (MOH) [72].
In conclusion, the stigma of migraine is a complex and multifaceted problem that can have a significant impact on the lives of people with this condition. It can lead to discrimination in the workplace, healthcare settings, and personal relationships. It can also lead to feelings of shame, guilt, and isolation. It affects women more than men. Some promising approaches to chasing migraine stigma include raising awareness about migraine and their impact on people’s lives, challenging negative stereotypes, and providing support for people with migraine. Reducing the stigma of migraine is an important step towards improving the quality of life for people with this condition. By doing so we can create a more inclusive society where patients with migraine are treated with respect and dignity.
Social determinants
In recent years, a growing attention has been made to the social determinants (SD) of health i.e., the conditions in which people are born, live, grow up, and function, and which affect their access to health and outcome [73]. As early as 1848 Rudolph Virchow noted that “if medicine is to accomplish its great task, it must intervene in political and social life” [74]. The World Health Organization (WHO) currently divides SD into 5 core domains that affect human health: 1. access to and quality of health care, 2. access to and quality of education, 3. social context, 4. economic stability and 5. environment/neighborhood [75].
Despite significant advances in the diagnosis and treatment of headaches, many patient groups in the world are still marginalized for historical, social or economic reasons. These include communities of color, people experiencing poverty, the un- or under-employed, the un- and under-insured, immigrants, women, people with low levels of education. These groups are also underrepresented in migraine research [76, 77].
According to the analyses from the 2017 GBD, the disability-adjusted life years (DALYs) are significantly higher for headaches in women compared to men. In women, migraine is among the top five most common causes of disability [6, 78]. The course of migraine in women is undoubtedly influenced by the nature of the pain experience, involvement in multiple fulfilling roles, and different coping strategies [79]. On the other hand, men are less likely to seek medical care and access treatment, which is often due to a certain perception that men are the gender that must be strong. In addition, the higher prevalence of migraine in women has contributed to the classification of the condition as a “female disorder” which has negative consequences for both sexes [80].
In addition, migraine prevalence is higher (regardless of gender) among those with lower family income and the unemployed, as well as the elderly and disabled [81].
According to the study results from Loder et al., racial and ethnic minorities in the U.S. may not receive adequate medical care for headache treatment compared with whites [82]. Even after accounting for demographic and insurance differences, black people are 40% less likely to be treated by a neurologist than whites. On the other hand, they are more likely to end up in emergency departments due to undertreated migraine [83]. The role of structural racism has been raised during the COVID-19 pandemic where disproportionate morbidity and mortality has been reported in Latinos, Asian, African-American and black populations. The key factor was the impact not of race alone but of access to health care [84]. The literature is very sparse when it comes to pediatric populations, but it has been shown that white children are significantly more likely to have neuroimaging for headaches than children of other races [85]. However, the prevalence of headache in children from all latitudes remains underestimated [86].
Migraine disproportionately affects also those living in poorer social conditions in terms of prevalence and severity and result in higher stress due to exogenous factors such as personal and food insecurity, employment, poverty and poorer access to health care [87, 88]. U.S. studies show that low-income or uninsured individuals who lack opportunities for proper medical care are more likely to develop medication overuse including opiates [89].
The etiology of migraine is not well understood but it is hypothesized that is a multifactorial disease influenced by numerous factors including genetic, epigenetic but also lifestyle, personal history and environmental factors [76, 90]. People living in areas with high air pollution, exposure to toxins, lack of access to water, frequent changes in weather conditions, and poor nutrition experience greater psychosocial stress, which affects the course of the disease [91, 92].
All of the above social determinants affect specific areas of disparity and/or inequality in adult and pediatric headache. These are primarily the use of health care services for migraine treatment, more frequent misdiagnosis, lack of trust in health care professionals, inadequate treatment and increased risk of migraine progression and burden of the disease [5].
Analyzing social determinants and all the above aspects, it should be remembered that the primary factors for the limitations in resource-restricted settings are as political instability, ongoing wars, limited resources, and mass displacement of people.
Patients’ point of view
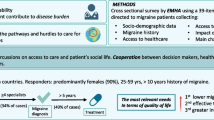
Patients are the individuals directly experiencing migraine and its associated stigma. By considering their perspective, physicians could gain a holistic understanding of the impact of stigma on their lives. This insight goes beyond clinical observations and provides a comprehensive view of the challenges they face in their daily lives, including social, emotional, and psychological aspects [65]. Understanding patients’ perspectives is fundamental to providing patient-centered care. It allows healthcare professionals and researchers to tailor interventions, support systems, and educational materials to better meet the needs of individuals living with migraines. This patient-centered approach can improve the effectiveness of interventions and ultimately enhance the quality of care. Patients’ organizations, such as the European Migraine and Headache Alliance (EMHA), are critical in shaping policies related to healthcare, disability accommodations, and anti-stigma initiatives.
During 2023, the EMHA ran a survey about the stigma of people with migraine in different areas, e.g., relationships with friends, family, workplace or doctor’s appointments (EHMA survey 2023, unpublished data). In total, 4.210 responders from 17 European Countries participated in the survey. The vast majority were women and most responders reported to have severe migraine with more than 8 attacks per month. Overall, 93% of survey participants believe that migraine is not understood by the general public and it is more stigmatized than dementia, Parkinson’s disease or stroke. One of the most frequently reported reasons for stigma is that migraine is often considered as “just a headache” and affected individuals are seen as weak, complaining people [65, 93].
Many of them feel stigmatized at their workplace, and 62% of them feel that migraine has affected how their employer assesses their value. They feel anger, loneliness and sadness at their workplace because of the stigma they experience. As a result, they feel uncomfortable disclosing their condition, they are afraid of being “punished” and they try to hide their disease at work. Even more worryingly, 35% of responders also felt stigmatized by their doctor, often avoiding or delaying seeking treatments due to concerns about what their doctor may think about them.
Similar topics emerged also from a US-American patients’ report in a focus group format [94]. Similar to their European counterparts, key topics from the patients’ point of view were the impact of migraine on family and work, misunderstanding by others, and issues related to medical care, such as feeling dismissed by the treating physicians [94].
Stigma in migraine often comes due to a lack of understanding of the condition and to its invisibility [95]. The debilitating nature of migraine cannot be immediately seen or recognized from the outside and patients often live with the fear of not being believed [95]. Among patients with chronic migraine, almost half had the feeling that even their spouse did not believe them about having headache attacks [71].
From the patient’s point of view, there is a strong need for a different way of speaking of migraine in order to reduce stigma and discrimination [96]. Migraine as every other disease has a large range of severities. The ones who are visible by the general public, by the policymakers or by the payers are often only the less severe ones that can nearly perform in a normal way. The most severe ones are hidden at home with a life completely conditioned by their pain and other symptoms and without any legal or social support [97]. One of the most important current goals is a society that recognizes the disease and the burden of its stigma at home, at the workplace but also in the healthcare systems. Access to innovative treatments should have to be also easier and with less complex protocols since while the affected ones are trying possible not specific treatments, days and days of their life are passing without letting them enjoy a normal life.
Secondary headaches
Secondary headache disorders are conditions in which headache is a symptom, that usually begins or worsens in parallel with the secondary cause, and improves or ceases when the secondary disorder does [1]. Not all secondary headache disorders are equally threatening, while some causes are relatively benign, others may threaten the patient’s life [98]. In the ICHD-3118 different causes of high-risk headache are listed [1]. If tension-type headache and migraine are the second and third most prevalent disorders worldwide [6], headache as a symptom of a secondary cause may be even more prevalent. The Table 1 depicts the incidence and prevalence of the main disorders listed under the secondary headache categories of the ICHD-3, and the estimated prevalence of headache, along with the 95% confidence intervals (CI).
The true prevalence of secondary headache disorders remains unknown. It varies depending on the region (some headache disorders may be more prevalent in low-and-middle income countries, such as malaria or dengue), the setting (urban versus rural) and the location where the study was conducted (emergency room, outpatient clinics or at a population level). In addition, epidemiological studies must ensure that patients are correctly diagnosed and classified, which may not always be the case.
In a study conducted in Türkiye, Ivory Coast, Chad, Senegal, Sudan, Ethiopia, Morocco, Egypt, Iran from Tatarstan, Turkish Republic of Northern Cyprus, Azerbaijan, and Mongolia 13,794 patients admitted to a hospital or an outpatient clinic were assessed, among which, 4144 (30%) reported headache as the main symptom. The prevalence of secondary headache disorders was 1249/3722 (33%), with no remarkable differences within the studied regions. The most prevalent headache disorders were medication overuse headache (9%), idiopathic intracranial hypertension (3%), and cervicogenic headache (3%) [108].
Due to the generally acute nature, most secondary headache disorders visit the Emergency Department as first contact with the healthcare system. In a study conducted in Colombia, in an Emergency Department during five consecutive weeks, all admissions were screened and in 244/10450 (2.3%), with a proportion of secondary headache disorders of 32% [109]. In another study conducted in an emergency department setting, the proportion of patients with secondary headache disorders corresponded to 11.2% of all headache patients, with 5% of them attributed to disorders with high morbidity and/or mortality [98]. This is particularly relevant, since the education of healthcare providers must be a priority. One study evaluated whether the diagnosis of TTH was accurate in the emergency department, and in 30% of cases, a secondary headache disorder had been misdiagnosed as TTH, reflecting that the need of continuous medical education and training in headache medicine [110,111,112]. Given the vast prevalence of primary and secondary headache disorders, most patients will be evaluated in primary care, or in secondary care, while tertiary centers should be reserved for difficult to treat or complicated cases, however, in some settings, the number of headache specialists may be insufficient, and most patients are treated by general practitioners or nurse practitioners [113]. In LMIC the lack of resources is even more evidence, and also there is a regional unbalance of health care centers and human resources (e.g. in Morocco far south is the poorest one regarding these elements, followed by east and center. Rural settings are the places most often affected) [113,114,115,116]. The differences among geographical regions regarding the prevalences of different secondary headaches is shown in Table 2.
Conclusion
Migraine is an extremely common and lifelong disorder. Migraine can affect every domain of life and is associated with a significant disability and poor quality of life, if it is not adequately treated. A correct management should include not only an optimal reduction of pain, in terms of monthly migraine days and intensity of crises, but also the improvement of quality of life, in terms of returning to an acceptable daily routine. These goals can be addressed not only with the relief of pain directly, but also with indirect measures aimed at raising awareness among general clinicians who can manage patients with migraine for the first time, but also among the general population. Social, geographical, and economic differences between the different ethnic groups should be mitigated, even more so after the recent COVID-19 pandemic which led to strong differences in health equity. The demonstration of specific pathophysiological mechanisms, and the use of tailored therapeutic agents, is a great achievement of the modern research of migraine because it could help to reduce the social stigma about this disorder. The recent introduction of new therapeutic targets addressing the CGRP is a significant breakthrough in the management of migraine, and there are interesting results in terms of pain improvement and disability reduction. The high costs of these novel therapeutic agents limit, actually, their routine use only in high-income countries. However, when analyzing the current global health situation in the context of headache medicine, we must also be aware that most likely that headache inequities are likely to persist and worsen due to various factors, including inflation reinforcing health inequities, inaccessible advancing technologies, and the lack of prioritization of academic headache research in resource-rich settings. The ongoing COVID-19 pandemic exacerbates these inequities. Future studies should evaluate the global feasibility of supporting their use in real-world settings and their long-term tolerability. Periodic awareness campaigns should be encouraged to reduce social factors that could stigmatize and underestimate the migraine as a psychosocial disorder and improve headache education at medical schools.
Availability of data and materials
No datasets were generated or analysed during the current study.
References
No authors listed (2018) Headache classification Committee of the International Headache Society (IHS) the international classification of headache disorders, 3rd edition. Cephalalgia 38(1):1–211
Sakai F, Igarashi H, Yokoyama M, Begasse de Dhaem O, Kato H, Azuma Y, Koh R, Phillips H, Singh N, Craven A, Dodick DW, Miyake H (2023) Diagnosis, knowledge, perception, and productivity impact of headache education and clinical evaluation program in the workplace at an information technology company of more than 70,000 employees. Cephalalgia 43(4):3331024231165682
Stovner LJ, Hagen K, Linde M, Steiner TJ (2022) The global prevalence of headache: an update, with analysis of the influences of methodological factors on prevalence estimates. J Headache Pain 23(1):34
García-Azorín D, Santana-López L, Lozano-Alonso JE, Ordax-Díez A, González-Osorio Y, Rojo-Rello S, Eiros JM, Sánchez-Martínez J, Recio-García A, Sierra-Mencía Á, Sanz-Muñoz I, Guerrero-Peral ÁL (2023) InfluenCEF study: clinical phenotype and duration of headache attributed to influenza infection. Cephalalgia 43(11):3331024231212900
Ashina M, Katsarava Z, Do TP, Buse DC, Pozo-Rosich P, Özge A, Krymchantowski AV, Lebedeva ER, Ravishankar K, Yu S, Sacco S, Ashina S, Younis S, Steiner TJ, Lipton RB (2021) Migraine: epidemiology and systems of care. Lancet 397(10283):1485–1495
GBD 2016 Headache Collaborators (2018) Global, regional, and national burden of migraine and tension-type headache, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 17(11):954–976
Manandhar K, Risal A, Steiner TJ, Holen A, Linde M (2015) The prevalence of primary headache disorders in Nepal: a nationwide populationbased study. J Headache Pain 16:95
Ravishankar K (2003) Migraine management in developing countries: barriers to care—a headache clinic study from India. Cephalalgia 23:577
Liu R, Yu S, He M, Zhao G, Yang X, Qiao X, Feng J, Fang Y, Cao X, Steiner TJ (2013) Health-care utilization for primary headache disorders in China: a population-based door-to-door survey. J Headache Pain 14(1):47
Linde M, Gustavsson A, Stovner LJ, Steiner TJ, Barré J, Katsarava Z, Lainez JM, Lampl C, Lantéri-Minet M, Rastenyte D, Ruiz de la Torre E, Tassorelli C, Andrée C (2012) The cost of headache disorders in Europe: the Eurolight project. Eur J Neurol 19(5):703–711
Stokes M, Becker WJ, Lipton RB, Sullivan SD, Wilcox TK, Wells L, Manack A, Proskorovsky I, Gladstone J, Buse DC, Varon SF, Goadsby PJ, Blumenfeld AM (2011) Cost of health care among patients with chronic and episodic migraine in Canada and the USA: results from the international Burden of migraine study (IBMS). Headache 51(7):1058–1077
Bonafede M, Sapra S, Shah N, Tepper S, Cappell K, Desai P (2018) Direct and indirect healthcare resource utilization and costs among migraine patients in the United States. Headache 58:700–714
Waliszewska-Prosół M, Straburzyński M, Czapińska-Ciepiela EK, Nowaczewska M, Gryglas-Dworak A, Budrewicz S (2023) Migraine symptoms, healthcare resources utilization and disease burden in a large polish migraine cohort : results from 'Migraine in Poland'-a nationwide cross-sectional survey. J Headache Pain 24(1):40
Ayzenberg I, Katsarava Z, Sborowski A, Chernysh M, Osipova V, Tabeeva G, Yakhno N, Steiner TJ, Lifting the Burden. (2012) The prevalence of primary headache disorders in Russia: a countrywide survey. Cephalalgia 32(5):373–381
Mbewe E, Zairemthiama P, Yeh H-H, Paul R, Birbeck GL, Steiner TJ (2015) The epidemiology of primary headache disorders in Zambia: a population-based door-to-door survey. J Headache Pain 16:515
Yu S, Liu R, Zhao G, Yang X, Qiao X, Feng J, Fang Y, Cao X, He M, Steiner T (2012) The prevalence and burden of primary headaches in China: a population-based door-to-door survey. Headache 52(4):582–591
Linde M, Steiner TJ, Chisholm D (2015) Cost-effectiveness analysis of interventions for migraine in four low and middle-income countries. J Headache Pain 16:15
Tana C, Azorin DG, Cinetto F, Mantini C, Tana M, Caulo M, Ricci F, Martelletti P, Cipollone F, Giamberardino MA (2023) Common clinical and molecular pathways between migraine and sarcoidosis. Int J Mol Sci 24(9):8304
Tana C, Bentivegna E, Cho SJ, Harriott AM, García-Azorín D, Labastida-Ramirez A, Ornello R, Raffaelli B, Beltrán ER, Ruscheweyh R, Martelletti P (2022) Long COVID headache. J Headache Pain 23(1):93
Affaitati G, Costantini R, Tana C, Cipollone F, Giamberardino MA (2020) Co-occurrence of pain syndromes. J Neural Transm (Vienna) 127(4):625–646
Gong Q, Liu S, Li R, Yao L, Xiao Z (2021) Overall trend towards headache remission during the COVID-19 pandemic among Chinese patients with pre-existing headache highlights the role of family support. BMC Neurol 21(1):224
Polverino F, Stern DA, Ruocco G, Balestro E, Bassetti M, Candelli M, Cirillo B, Contoli M, Corsico A, D'Amico F, D'Elia E, Falco G, Gasparini S, Guerra S, Harari S, Kraft M, Mennella L, Papi A, Parrella R, Pelosi P, Poletti V, Polverino M, Tana C, Terribile R, Woods JC, Di Marco F, Martinez FD, ItaliCO study group (2020) Comorbidities, Cardiovascular Therapies, and COVID-19 Mortality: A Nationwide, Italian Observational Study (ItaliCO). Front Cardiovasc Med 7:585866
Ebbesen BD, Giordano R, Valera-Calero JA, Hedegaard JN, Fernández-de-Las-Peñas C, Arendt-Nielsen L (2023) Prevalence and risk factors of de novo widespread post-COVID pain in non-hospitalized COVID-19 survivors: a nation-wide exploratory population-based survey. J Pain S1526-5900(23):00512–00516
Tana C, Giamberardino MA, Martelletti P (2023) Long COVID and especially headache syndromes. Curr Opin Neurol 36(3):168–174
Krymchantowski AV, Silva-Néto RP, Jevoux C, Krymchantowski AG (2022) Indomethacin for refractory COVID or post-COVID headache: a retrospective study. Acta Neurol Belg 122(2):465–469
Gonzalez-Martinez A, Guerrero-Peral ÁL, Arias-Rivas S, Silva L, Sierra Á, Gago-Veiga AB, García-Azorín D (2022) Amitriptyline for post-COVID headache: effectiveness, tolerability, and response predictors. J Neurol 269(11):5702–5709
Vinyes D, Muñoz-Sellart M, Caballero TG (2022) Local anesthetics as a therapeutic tool for post COVID-19 patients: a case report. Medicine (Baltimore) 101(28):e29358
Tana C, Cipollone F, Giamberardino MA (2023) New therapeutic options for migraine. Curr Pharm Des 29(25):1964–1966
Tana C, Cipollone F, Giamberardino MA, Martelletti P (2023) New drugs targeting calcitonin gene-related peptide for the management of migraines. Expert Opin Emerg Drugs 28(4):233–240.
Takizawa T, Ihara K, Uno S, Ohtani S, Watanabe N, Imai N, Nakahara J, Hori S, Garcia-Azorin D, Martelletti P (2023) Metabolic and toxicological considerations regarding CGRP mAbs and CGRP antagonists to treat migraine in COVID-19 patients: a narrative review. Expert Opin Drug Metab Toxicol 5:1–17
Rist PM, Buring JE, Manson JE, Sesso HD, Kurth T (2023) History of migraine and risk of COVID-19: a cohort study. Am J Med 136(11):1094–1098
Straburzyński M, Kuca-Warnawin E, Waliszewska-Prosół M (2023) COVID-19-related headache and innate immune response - a narrative review. Neurol Neurochir Pol 57(1):43–52
Aparisi Á, Ybarra-Falcón C, Iglesias-Echeverría C, García-Gómez M, Marcos-Mangas M, Valle-Peñacoba G, Carrasco-Moraleja M, Fernández-de-Las-Peñas C, Guerrero ÁL, García-Azorín D (2022) Cardio-pulmonary dysfunction evaluation in patients with persistent post-COVID-19 headache. Int J Environ Res Public Health 19(7):3961
Ticinesi A, Nouvenne A, Tana C, Prati B, Meschi T (2019) Gut microbiota and microbiota-related metabolites as possible biomarkers of cognitive aging. Adv Exp Med Biol 1178:129–154
Ticinesi A, Tana C, Nouvenne A, Prati B, Lauretani F, Meschi T (2018) Gut microbiota, cognitive frailty and dementia in older individuals: a systematic review. Clin Interv Aging 13:1497–1511
Ticinesi A, Nouvenne A, Tana C, Prati B, Cerundolo N, Miraglia C, De' Angelis GL, Di Mario F, Meschi T (2018) The impact of intestinal microbiota on bio-medical research: definitions, techniques and physiology of a "new frontier". Acta Biomed 89(9-S):52–59
Bicknell B, Liebert A, Borody T, Herkes G, McLachlan C, Kiat H (2023) Neurodegenerative and neurodevelopmental diseases and the gut-brain Axis: the potential of therapeutic targeting of the microbiome. Int J Mol Sci 24(11):9577
Di Lauro M, Guerriero C, Cornali K, Albanese M, Costacurta M, Mercuri NB, Di Daniele N, Noce A (2023) Linking migraine to gut Dysbiosis and chronic non-communicable diseases. Nutrients 15(20):4327
Ticinesi A, Tana C, Nouvenne A (2019) The intestinal microbiome and its relevance for functionality in older persons. Curr Opin Clin Nutr Metab Care 22(1):4–12
Ticinesi A, Lauretani F, Tana C, Nouvenne A, Ridolo E, Meschi T (2019) Exercise and immune system as modulators of intestinal microbiome: implications for the gut-muscle axis hypothesis. Exerc Immunol Rev 25:84–95
Li Y-D, Chi W-Y, Su J-H et al (2020) Coronavirus vaccine development: from SARS and MERS to COVID-19. J Biomed Sci 27:104
Meo SA, Bukhari IA, Akram J, Meo AS, Klonoff DC (2021) COVID-19 vaccines: comparison of biological, pharmacological characteristics and adverse effects of Pfizer/BioNTech and Moderna vaccines. Eur Rev Med Pharmacol Sci 25(3):1663–1669
Castaldo M, Waliszewska-Prosół M, Koutsokera M et al (2022) Headache onset after vaccination against SARS-CoV-2: a systematic literature review and meta-analysis. J Headache Pain 23(1):41
Sekiguchi K, Watanabe N, Miyazaki N, Ishizuchi K, Iba C, Tagashira Y, Uno S, Shibata M, Hasegawa N, Takemura R, Nakahara J, Takizawa T (2022) Incidence of headache after COVID-19 vaccination in patients with history of headache: a cross-sectional study. Cephalalgia 42(3):266–272
Silvestro M, Tessitore A, Orologio I, Sozio P, Napolitano G, Siciliano M, Tedeschi G, Russo A (2021) Headache worsening after COVID-19 vaccination: an online questionnaire-based study on 841 patients with migraine. J Clin Med 10:5914
Brandt RB, Ouwehand RH, Ferrari MD, Haan J, Fronczek R (2022) COVID-19 vaccination-triggered cluster headache episodes with frequent attacks. Cephalalgia 42(13):1420–1424
Chen SP, Takizawa T, Sekiguchi K, Nakahara J, Wang SJ (2023) COVID-19 vaccination elicited de novo and recurrence of cluster headache: a case series. Cephalalgia 43(5):3331024231173354
Suwanwela NC, Kijpaisalratana N, Tepmongkol S, Rattanawong W, Vorasayan P, Charnnarong C, Tantivattana J, Roongruang S, Ongphichetmetha T, Panjasriprakarn P, Chutinet A, Akarathanawat W, Saver JL (2022) Prolonged migraine aura resembling ischemic stroke following CoronaVac vaccination: an extended case series. J Headache Pain 23(1):13
Waliszewska-Prosół M, Budrewicz S (2021) The unusual course of a migraine attack during COVID-19 infection - case studies of three patients. J Infect Public Health 14(7):903–905
González-Celestino A, González-Osorio Y, García-Iglesias C, Echavarría-Iñiguez A, Sierra-Mencía A, Recio-García A, Trigo-López J, Planchuelo-Gómez A, Hurtado ML, Sierra-Martínez L, Ruiz M, Rojas-Hernández M, Pérez-Almendro C, Paniagua M, Núñez G, Mora M, Montilla C, Martínez-Badillo C, Lozano AG, Gil A, Cubero M, Cornejo A, Calcerrada I, Blanco M, Alberdí-Iglesias A, Fernández-de-Las-Peñas C, Guerrero-Peral AL, García-Azorín D (2023) Differences and similarities between COVID-19 related-headache and COVID-19 vaccine related-headache. A case-control study. Rev Neurol 77(10):229–239
García-Azorín D, Do TP, Gantenbein AR, Hansen JM, Souza MNP, Obermann M, Pohl H, Schankin CJ, Schytz HW, Sinclair A, Schoonman GG, Kristoffersen ES (2021) Delayed headache after COVID-19 vaccination: a red flag for vaccine induced cerebral venous thrombosis. J Headache Pain 22(1):108
Tana C, Moffa L, Falasca K, Vecchiet J, Tana M, Mantini C, Ricci F, Ticinesi A, Meschi T, Cipollone F, Giamberardino MA (2023) Approach to COVID-19 in older adults and indications for improving the outcomes. Ann Med 55(2):2265298
Munblit D, O'Hara ME, Akrami A, Perego E, Olliaro P, Needham DM (2022) Long COVID: aiming for a consensus. Lancet Respir Med 10(7):632–634
Sukocheva OA, Maksoud R, Beeraka NM, Madhunapantula SV, Sinelnikov M, Nikolenko VN, Neganova ME, Klochkov SG, Amjad Kamal M, Staines DR, Marshall-Gradisnik S (2022) Analysis of post COVID-19 condition and its overlap with myalgic encephalomyelitis/chronic fatigue syndrome. J Adv Res 40:179–196
Rodrigues AN, Dias ARN, Paranhos ACM, Silva CC, Bastos TDR, de Brito BB, da Silva NM, de Sousa EJS, Quaresma JAS, Falcão LFM (2023 Mar) Headache in long COVID as disabling condition: a clinical approach. Front Neurol 23(14):1149294
Venkataramani V, Winkler F (2022) Cognitive deficits in long Covid-19. N Engl J Med 387(19):1813–1815
Sampaio Rocha-Filho PA, Voss L (2020) Persistent headache and persistent anosmia associated with COVID-19. Headache 60(8):1797–1799
Straburzynski M, Nowaczewska M, Budrewicz S, Waliszewska-Prosół M (2022) COVID-19-related headache and sinonasal inflammation: a longitudinal study analyzing the role of acute rhinosinusitis and ICHD-3 classification difficulties in SARS-CoV-2 infection. Cephalalgia 42(3):218–228
Dono F, Consoli S, Evangelista G, D'Apolito M, Russo M, Carrarini C et al (2021) New daily persistent headache after SARS-CoV-2 infection: a report of two cases. Neurol Sci 42(10):3965–3968
Caronna E, Ballvé A, Llauradó A, Gallardo VJ, Ariton DM, Lallana S, López Maza S, Olivé Gadea M, Quibus L, Restrepo JL, Rodrigo-Gisbert M, Vilaseca A, Hernandez Gonzalez M, Martinez Gallo M, Alpuente A, Torres-Ferrus M, Pujol Borrell R, Alvarez-Sabin J, Pozo-Rosich P (2020) Headache: a striking prodromal and persistent symptom, predictive of COVID-19 clinical evolution. Cephalalgia 40(13):1410–1421
Garcia-Azorin D, Layos-Romero A, Porta-Etessam J, Membrilla JA, Caronna E, Gonzalez-Martinez A, Mencia ÁS, Segura T, Gonzalez-García N, Díaz-de-Terán J, Gallardo VJ, Gago-Veiga AB, Ballvé A, Trigo López J, Sastre-Real M, Llauradó A, Cornejo A, de Lorenzo Í, Guerrero-Peral Á, Pozo-Rosich P (2022) Post-COVID-19 persistent headache: a multicentric 9-months follow-up study of 905 patients. Cephalagia 42(8):804–809
Raffaelli B, Kull P, Mecklenburg J, Overeem LH, Storch E, Terhart M, Neeb L, Reuter U (2021) Patients' and Health care Workers' perception of migraine images on the internet: cross-sectional survey study. J Med Internet Res 23(11):e32707
Kempner J (2014) Not tonight: migraine and the politics of gender and health. The University of Chicago Press, Chicago
Parikh SK, Kempner J, Young WB (2021) Stigma and migraine: developing effective interventions. Curr Pain Headache Rep 25(11):75
Gross E, Ruiz de la Torre E, Martelletti P (2023) The migraine stigma kaleidoscope view. Neurol Ther 12(3):703–709
World Health Organization. Atlas of headache disorders and resources in the world.2011.https://www.who.int/mental_health/management/who_atlas_headache_disorders.pdf?ua=1
Schwedt TJ, Shapiro RE (2009) Funding of research on headache disorders by the National Institutes of Health. Headache: the journal of head and face. Pain 49(2):162–169
Dodick DW, Loder EW, Manack Adams A, Buse DC, Fanning KM, Reed ML, Lipton RB (2016) Assessing barriers to chronic migraine consultation, diagnosis, and treatment: results from the chronic migraine epidemiology and outcomes (CaMEO) study. Headache 56(5):821–834
Pescosolido BA, Martin JK (2015) The stigma complex. Annu Rev Sociol 41:87–116
Young WB, Park JE, Tian IX, Kempner J (2013) The stigma of migraine. PLoS One 8(1):e54074
Buse DC, Scher AI, Dodick DW, Reed ML, Fanning KM, Manack Adams A, Lipton RB (2016) Impact of migraine on the family: perspectives of people with migraine and their spouse/domestic partner in the CaMEO study. Mayo Clin Proc S0025-6196(16):00126–00129
Perugino F, De Angelis V, Pompili M, Martelletti P (2022) Stigma and chronic pain. Pain Ther 11(4):1085–1094. https://doi.org/10.1007/s40122-022-00418-5
Rosendale N (2022) Social determinants of Health in neurology. Neurol Clin 40(1):231–247
Ruffin J (2010) The science of eliminating health disparities: Embracing a new paradigm. Am J Public Health 100(Suppl 1):S8–S9
Centers for Disease Control and Prevention. About Social Determinants of Health (SDOH). 2021. available at: https://www.cdc.gov/socialdeterminants/about.html. Accessed March 30, 2021
Befus DR, Irby MB, Coeytaux RR, Penzien DB (2018) A critical exploration of migraine as a Health disparity: the imperative of an equity-oriented, intersectional approach. Curr Pain Headache Rep 22(12):79
Braveman PA, Kumanyika S, Fielding J, Laveist T, Borrell LN, Manderscheid R, Troutman A (2011) Health disparities and health equity: the issue is justice. Am J Public Health 101(Suppl 1(Suppl 1):S149–S155
Cislaghi B, Weber AM, Gupta GR, Darmstadt GL (2020) Gender equality and global health: intersecting political challenges. J Glob Health 10(1):010701
Smitherman TA, Ward TN (2011) Psychosocial factors of relevance to sex and gender studies in headache. Headache 51:923–931
Heise L, Greene ME, Opper N, Stavropoulou M, Harper C, Nascimento M, Zewdie D, Gender Equality, Norms, and Health Steering Committee (2019) Gender inequality and restrictive gender norms: framing the challenges to health. Lancet 393(10189):2440–2454
Burch R, Rizzoli P, Loder E (2018) The prevalence and impact of migraine and severe headache in the United States: figures and trends from government health studies. Headache 58(4):496–505
Loder S, Sheikh HU, Loder E (2015) The prevalence, burden, and treatment of severe, frequent, and migraine headaches in US minority populations: statistics from National Survey studies. Headache 55(2):214–228
Saadi A, Himmelstein DU, Woolhandler S et al (2017) Racial disparities in neurologic health care access and utilization in the United States. Neurology 88(24):2268–2275
Yehia BR, Winegar A, Fogel R, Fakih M, Ottenbacher A, Jesser C, Bufalino A, Huang RH, Cacchione J (2020) Association of Race With Mortality Among Patients Hospitalized With Coronavirus Disease 2019 (COVID-19) at 92 US Hospitals. JAMA Network Open 3(8):e2018039
Charleston L 4th (2021) Headache disparities in African-Americans in the United States: a narrative review. J Natl Med Assoc 113(2):223–229
Onofri A, Pensato U, Rosignoli C et al (2023) Primary headache epidemiology in children and adolescents: a systematic review and meta-analysis. J Headache Pain 24(1):8
Charleston L 4th, Royce J, Monteith TS, Broner SW, O'Brien HL, Manrriquez SL, Robbins MS (2018) Migraine care challenges and strategies in US uninsured and underinsured adults: a narrative review, part 1. Headache 58(4):506–511
Affatato O, Miguet M, Schiöth HB, Mwinyi J (2021) Major sex differences in migraine prevalence among occupational categories: a cross-sectional study using UK biobank. J Headache Pain 22(1):145
Atasoy HT, Unal AE, Atasoy N, Emre U, Sumer M (2005) Low income and education levels may cause medication overuse and chronicity in migraine patients. Headache 45(1):25–31
Grangeon L, Lange KS, Waliszewska-Prosół M et al (2023) Genetics of migraine: where are we now? J Headache Pain 24(1):12
Kurtses Gürsoy B, Köseoğlu TC (2023) Psychological resilience and stress coping styles in migraine patients. Neuropsychiatr Dis Treat 19:63–72
Chalmer MA, Rasmussen AH (2021) International headache genetics consortium; 23andme research team; Kogelman LJA, Olesen J, Hansen TF. Chronic migraine: genetics or environment? Eur J Neurol 28(5):1726–1736
Pearson C, Swindale R, Keighley P, McKinlay AR, Ridsdale L (2019) Not just a headache: qualitative study about web-based self-presentation and social media use by people with migraine. J Med Internet Res 21(6):e10479
Cottrell C, Drew J, Waller S, Holroyd K, Brose J, O'Donnell F (2003) Perceptions and needs of patients with migraine: a focus group study. Headache 43(4):428–428
Rutberg S, Kerstin Ö (2012) Migraine--more than a headache: women's experiences of living with migraine. Disabil Rehabil 34(4):329–336
Battista S, Lazzaretti A, Coppola I, Falsiroli Maistrello L, Rania N, Testa M (2023) Living with migraine: a meta-synthesis of qualitative studies. Front Psychol 14:1129926
Hamann T, Hong JB, Lange KS et al (2023) Perception of typical migraine images on the internet: comparison between a metropolis and a smaller rural city in Germany. PLoS One 18(8):e0290318
García-Azorín D, Abelaira-Freire J, Rodriguez-Adrada E, González-García N, Guerrero ÁL, Porta-Etessam J, Martín-Sánchez FJ (2020) Study about the Manchester triage system subtriage in patients that visited the emergency department due to headache. Neurologia (Engl Ed) S0213-4853(20):30275–30279
Lieba-Samal D, Platzer P, Seidel S, Klaschterka P, Knopf A, Wöber C (2011) Characteristics of acute posttraumatic headache following mild head injury. Cephalalgia 31(16):1618–1626
Ashina H, Dodick DW, Barber J, Temkin NR, Chong CD, Adler JS, Stein KS, Schwedt TJ, Manley GT, Investigators TRACK-TBI (2023) Prevalence of and risk factors for post-traumatic headache in civilian patients after mild traumatic brain injury: a TRACK-TBI study. Mayo Clin Proc S0025-6196(23):00113–00111
Suwanwela N, Phanthumchinda K, Kaoropthum S (1994) Headache in brain tumor: a cross-sectional study. Headache 34(7):435–438
Forsyth PA, Posner JB (1993) Headaches in patients with brain tumors: a study of 111 patients. Neurology 43(9):1678–1683. https://doi.org/10.1212/wnl.43.9.1678
van de Beek D, de Gans J, Spanjaard L, Weisfelt M, Reitsma JB, Vermeulen M (2004) Clinical features and prognostic factors in adults with bacterial meningitis. N Engl J Med 351(18):1849–1859
Monto AS, Gravenstein S, Elliott M, Colopy M, Schweinle J (2000) Clinical signs and symptoms predicting influenza infection. Arch Intern Med 160(21):3243–3247
Acray-Zengbé P, Ano MN, Toure B, Kouassi PR, Ané AB, Akani C, Dagnan S (2020) Gratuité de la prise en charge du paludisme simple dans un hôpital général, Côte d’Ivoire, 2017. Sante Publique 32(4):419–429
Guo C, Zhou Z, Wen Z et al (2017) Global epidemiology of dengue outbreaks in 1990-2015: a systematic review and Meta-analysis. Front Cell Infect Microbiol 7:317
Navarro-Pérez MP, Espinosa-Rueda J, Ballesta-Martínez S, Revilla-Martí P, Olesen J, Bellosta-Diago E, Santos-Lasaosa S (2023) Prevalence, clinical characteristics and associated factors of cardiac cephalalgia: a prospective study. Cephalalgia 43(4):3331024231160743. https://doi.org/10.1177/03331024231160743
Evlice A, Genç H, Uluduz D, Baykan B, Bolay H, Unal-Cevik I, Kissani N, Luvsannorov O, Togha M, Ozge A, Head-MENAA study group (2023) Secondary headache disorders in Turkey, the Middle East, Asia, and Africa: a cross-sectional, multicenter study. Cephalalgia 43(8):3331024231194024
Munoz-Ceron J, Marin-Careaga V, Peña L, Mutis J, Ortiz G (2019) Headache at the emergency room: etiologies, diagnostic usefulness of the ICHD 3 criteria, red and green flags. PLoS One 14(1):e0208728
García-Azorín D, Farid-Zahran M, Gutiérrez-Sánchez M, González-García MN, Guerrero AL, Porta-Etessam J (2020) Tension-type headache in the emergency department diagnosis and misdiagnosis: the TEDDi study. Sci Rep 10(1):2446
Saylor D, Steiner TJ (2018) The global Burden of headache. Semin Neurol 38(2):182–190
Błaszczyk B, Straburzyński M, Więckiewicz M, Budrewicz S, Niemiec P, Staszkiewicz M, Waliszewska-Prosół M (2023) Relationship between alcohol and primary headaches: a systematic review and meta-analysis. J Headache Pain 24(1):116
Steiner TJ, Göbel H, Jensen R et al (2019) European headache federation and Lifting the Burden: the global campaign against headache. Headache service quality: the role of specialized headache centres within structured headache services, and suggested standards and criteria as centres of excellence. J Headache Pain 20(1):24
García-Azorín D, Molina-Sánchez M, Gómez-Iglesias P, Delgado-Suárez C, García-Morales I, Kurtis-Urra M, Monje MHG (2022) Headache education and management in Cameroon: a healthcare provider study. Acta Neurol Belg 122(1):75–81
Rosignoli C, Ornello R, Onofri A, Caponnetto V, Grazzi L, Raggi A, Leonardi M, Sacco S (2022) Applying a biopsychosocial model to migraine: rationale and clinical implications. J Headache Pain 23(1):100. https://doi.org/10.1186/s10194-022-01471-3 Erratum in: J Headache Pain 2022 Sep 7;23(1):116
Raffaelli B, Rubio-Beltrán E, Cho SJ, De Icco R, Labastida-Ramirez A, Onan D, Ornello R, Ruscheweyh R, Waliszewska-Prosół M, Messina R, Puledda F (2023) Health equity, care access and quality in headache - part 2. J Headache Pain 24(1):167
Acknowledgements
None.
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
CT, BR, MN, DGA, MWP, conception and design; CT, BR, MN, ERT, DGM, DGA, MWP, analysis and interpretation of the data; CT, BR, MN, ERT, DGM, NK, DGA, MWP, drafting of the paper, revising it critically for intellectual content and final approval of the version to be published. All authors agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Competing interests
CT, BR, DGA, MWP are editorial board members of the Journal of Headache and Pain. BR reports personal fees from AbbVie, Eli Lilly, Lundbeck, Novartis and Teva for participating in advisory boards and/or speaker activities as well as research funding from Novartis. MNPS reports personal fees from AbbVie, Eli Lilly, Lundbeck, Pfizer, LIBBS and Teva for participating in advisory boards and/or speaker activities. DGA has received research funding from the Regional Health Administration (Gerencia Regional de Salud SACYL) in Castilla y Leon, Spain. Speaker/travel grants/ clinical trials from Teva, Abbvie, Amgen, Eli Lilly, Lundbeck, Novartis, Pfizer and Biohaven. MWP reports personal fees from AbbVie, Pfizer and Teva for speaker activities.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tana, C., Raffaelli, B., Souza, M.N.P. et al. Health equity, care access and quality in headache – part 1. J Headache Pain 25, 12 (2024). https://doi.org/10.1186/s10194-024-01712-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s10194-024-01712-7