
Abstract
Background
Post-traumatic headache (PTH) is a common symptom following mild traumatic brain injury (mTBI). Patients at risk to develop acute PTH (aPTH) and further persistent PTH (pPTH) need to be recognized.
Methods
This is a one-year follow-up of 127 patients with mTBI, aged 18 to 68, referred to outpatient clinic in the Helsinki University Hospital. Symptoms were assessed at the emergency department (ED), with structured interview at outpatient clinic visit and with Rivermead post-concussion symptom questionnaire at one, three, and 12 months after injury. Psychiatric disorders were assessed with Structured Clinical Interview for DSM-IV Axis I disorders at 3-4 months and return to work (RTW) from patient records.
Results
At one month, 77/127 patients (61%) had aPTH. According to multiple logistic regression analysis, risk factors for aPTH were headache at the emergency department (ED) (OR 5.43), other pain (OR 3.19), insomnia (OR 3.23), and vertigo (OR 5.98). At three months, 17 patients (22% of aPTH patients) had developed pPTH, and at one year, 4 patients (24% of pPTH patients) still presented with pPTH. Risk factors for pPTH at three months were older age (OR 1.06) and current insomnia (OR 12.3). The frequency of psychiatric disorders did not differ between the groups. pPTH patients performed worse on their RTW.
Conclusions
Risk factors for aPTH were insomnia, headache at ED, other pain, and vertigo and for pPTH, insomnia and older age. RTW rate was lower among pPTH patients.
Similar content being viewed by others


Introduction
Traumatic brain injury (TBI) is estimated to affect 69 million individuals per year [1]. Mild TBI (mTBI) represents 70-90% of all TBIs [2,3,4]. Post-traumatic headache (PTH) is one of the most common symptoms following TBI [5,6,7] and is more common after mTBI than moderate or severe TBI [8].
Typically patients with mTBI recover within days or weeks. However, a subgroup of patients experience prolonged post-traumatic symptoms including headache, which can cause long-term disability and delayed return to work [9,10,11].
By definition, the onset of PTH occurs within seven days following the head trauma, within seven days after recovering from unconsciousness, or within seven days after recovering the ability to report symptoms [12]. During the first three months from onset, PTH is defined as acute, and beyond that, persistent [12].
The nature of PTH varies. Some studies have discovered that most people with PTH have a migraine-like headache [5], whereas others have found a higher prevalence of tension-type headaches [13]; still others experience features of chronic migraine- or cluster-like phenotypes [14, 15].
The difference of migraine and pPTH has previously been studied. E.g. brain functional neuroimaging findings and calcitonin gene-related peptide (CGRP) levels differ in migraine compared with pPTH suggesting distinct pathophysiologies. On the other hand, there might also be shared pathophysiology, of which initial open label studies on CGRP monoclonal antibodies in the treatment of pPTH have shown preliminary evidence [16].
According to previous studies, female gender may be a risk factor for PTH [10, 17], although there is also conflicting evidence [5]. Additionally, younger age, previous headache, and headache immediately after the injury are risk factors for PTH [10, 17]. Individuals with PTH often report concomitant symptoms such as anxiety, depression, and sleep disturbance [10, 18]. Psychiatric comorbidities are complex and prevalent also in migraine and shared pathophysiology mechanisms may play a key role in headache chronification. These are important to consider in the diagnostic work up and treatment [19].
According to a prognostic model developed for clinicians, lower education, injury severity, and psychological factors such as maladaptive coping style and pre-injury mental health problems play a role for prolonged symptoms in mTBI [20]. However, specific risk factors for development of persistent PTH (pPTH) remain understudied.
We aimed to thoroughly identify potential risk factors for acute PTH (aPTH) and further pPTH in mTBI patients by utilizing the Rivermead Post Concussion Symptom Questionnaire (RPQ) [21], Structured Clinical Interview for DSM-IV Axis I disorders (SCID-I) [22], and patient records from the emergency department (ED) and clinical neurology outpatient visits within one year’s follow-up.
We hypothesized that previous primary headaches, other pain condition, sleep disorders, and psychiatric burden would act as a risk factors for acute- and persistent PTH. Further, we presumed that pPTH would have negative impact on RTW.
Methods
Study design and patients
This is a substudy of a prospective cohort study conducted at the Traumatic Brain Injury Outpatient Clinic in the Helsinki University Hospital from March 2015 until September 2018 [23] Inclusion criteria were consecutive patients with mild brain injury and post-traumatic headache according to International Classification of Headache Disorders (ICHD-3) criteria [12], Finnish as their native language, aged 18 to 68 years. Exclusion criteria were alcohol or drug dependence, previously diagnosed schizophrenia or schizoaffective disease, mental retardation, and vision or hearing disability. The study was approved by the local ethical board of the Helsinki University Hospital. All patients gave their written informed consent.
Patients underwent 3T magnetic resonance imaging (MRI) within approximately two weeks after incident TBI. A senior neuroradiologist evaluated all MRI scans.
World Health Organization (WHO) criteria of mild traumatic brain injury were used [24]. WHO criteria include (1) one or more of the following: confusion or disorientation, loss of consciousness for 30 min or less, post-traumatic amnesia for less than 24 h, or other transient neurological abnormalities, such as focal signs, seizure, and intracranial lesion not requiring surgery; and (2) Glasgow Coma Scale (GCS) score of 13-15 after 30 min post-injury or later upon presentation for health care. WHO criteria approve minor trauma findings in CT or MR imaging.
In the study aPTH and pPTH were assigned according to ICHD-3 criteria [12]. Presence of headache was documented first at the emergency department (ED); aPTH was defined as headache occurring within seven days from the TBI (based on documents from the ED and structured interview together with RPQ at one month). At three months (pPTH) and 12 months after the injury, headache and other symptoms were assessed with Rivermead Post-Concussion Symptoms Questionnaire (RPQ), a 16-item self-report questionnaire measuring the presence and severity of common post-concussion symptoms on a 5-point Likert Scale (0-4) [21]. In our analysis the total RPQ score also included scale 1 (no longer a problem). If patients had not reported headache at one month, but reported it at three months, it was not classified as pPTH. Characteristics of pPTH were collected from patient records from the clinical neurologist appointment.
Questions regarding insomnia (yes/no) and other pain (yes/no) were part of the structured interview at one month.
At three to four months after injury, psychiatric disorders were assessed with the Structured Clinical Interview for DSM-IV Axis I disorders (SCID-I) [22].
Return to work (RTW) data was collected retrospectively from the patient records and evaluated with one-day accuracy. Individuals who returned to part-time work were also taken into account. We regarded a return to studies for full-time students as RTW.
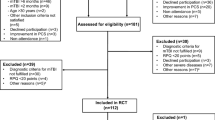
We recruited 131 patients with mTBI and 127 of them had filled in information about headache at one month. The study cohort consisted of 127 patients. At three months, information about headache was available for 100 patients and at 12 months, for 72 patients. The patient flow chart is illustrated in Fig. 1.

Distribution of patients according to presence of post-traumatic head-ache (PTH)
We named those patients who had acute PTH at one month aPTH and those patients who had acute PTH but not persistent PTH recovered-aPTH (r-aPTH).
Statistical analyses
Continuous variables are presented as mean (standard deviation, SD) if normally distributed and as median (interquartile range, IQR) if not normally distributed. Categorical variables are given as frequencies and percentages. For group comparisons, Pearson’s chi-square was used for binary categorical variables, one-way ANOVA for normally distributed continuous variables, and nonparametric Mann-Whitney U-tests for non-normally distributed continuous variables. Univariate and multiple logistic regression analysis were used to assess the possible risk factors for PTH. We considered p-values <0.05 as statistically significant. IBM SPSS Statistics 24 was used to perform the analysis.
Results
Demographics
The mean age of the 127 patients was 40 years (SD 12.9) and 46.5% were female. One hundred fifteen patients (90.6%) were employed or full-time students before trauma. Ground-level falls were the most frequent cause for TBI (33%); 24 patients (18.9%) were under influence of alcohol at the time of the trauma, according to patient records.
The following minor traumatic brain lesions were found in MRI: 48 patients (37.0%): any traumatic intracranial lesion, acute subdural hemorrhage in 20 patients (15.7%), small epidural hematoma in 1 patient, traumatic subarachnoidal hemorrhage in 19 patients (12.6%), traumatic intracerebral hemorrhage in 5 patients (3.1%), and microhemorrhages indicating diffuse axonal injury in 26 patients (20.5%), and minor cerebral contusion in 14 patients (11.0%). None of the patients with trauma findings needed surgery.
Patients with aPTH
At one month, 77/127 (61%) patients reported aPTH. Patient demographics for patients with aPTH and non-PTH are shown in Table 1.
Patients with aPTH had previous migraine (p = 0.033) and insomnia (p = 0.017) significantly more often than non-PTH patients. There was no difference in frequency of trauma findings between aPTH and non-PTH patients (Table 1).
Patients with aPTH reported headache significantly more often at the emergency department (ED) than non-PTH patients (p = 0.003). The median RPQ score at one month postinjury was significantly higher in aPTH than non-PTH patients (p < 0.001) (Table 1).
In multiple logistic regression analysis, headache at the ED (p = 0.029), other pain (p = 0.010), insomnia (p = 0.010), and vertigo (p < 0.001) were independent risk factors for aPTH (Table 2).
Patients with pPTH
17/77 of aPTH patients (22%) developed pPTH. The mean age of pPTH patients was 44.3 years (SD 12.8) with 47% women. Previous self-reported migraine was in 3/17 of pPHT patients (18%), previous other headache in 8/17 (47%), and previous insomnia in 7/17 (41%). Trauma findings in MRI were detected in 10/17 (59%) of pPTH patients.
In comparison between pPTH (n = 17) and r-aPTH (n = 43) patients, no statistically significant differences were found in demographic or clinical characteristics (Table 3) including insomnia after injury (77% vs. 51%, p = 0.073), trauma findings in MRI (59% vs. 33%, p = 0.061), and previous migraine (18% vs. 26%, p = 0.737).
When comparing pPTH with non-PTH (n = 40) patients, differences were more pronounced. Non-PTH patients were younger (mean age 36.5 years, p = 0.026), and pPTH patients reported insomnia after injury significantly more often than non-PTH patients (76.5% vs. 22.5%, p < 0.001).
In three-month follow-up RPQ scores, even when headache was excluded from the total score, pPTH patients had significantly more concomitant symptoms compared with r-aPTH and non-PTH patients. The median RPQ score of pPTH patients was 21 (IQR 12.00-26.5), which was significantly higher compared with r-aPTH and non-PTH patients, both of which had a median RPQ score of 2 (IQR 0.00-7.0), p <0.001.
In multiple logistic regression analysis comparing pPTH with non-PTH patients, older age (OR 1.06, 95% Cl 1.01-1.13, p = 0.034) and insomnia after injury (OR 12.3, 95% Cl 2.79-54.13, p = 0.001) were independent risk factors for pPTH.
At one year, 4 patients (24% of pPTH patients) still suffered from headache.
Psychiatric profile
In SCID-I interviews, psychiatric disorders were diagnosed in 7/17 (41%) of pPTH, 8/35 (22%) of aPTH, and 7/35 (20%) of non-PTH patients. The distribution of different psychiatric disorders did not differ between groups. The most common disorders were acute and current depression, panic disorder, and social anxiety disorder.
Return to work
RTW at three months was documented for all patients who were either employed or full-time students before trauma (n = 91, including 6 students).
At three months, pPTH and r-aPTH patients differed significantly in the rate of return to full-time work (69% vs. 94%, p = 0.025). Similar difference was found between pPTH and non-PTH patients (69% vs. 93%, p = 0.035) (Table 4). At 12 months follow-up, all except one patient with pPTH had returned to work.
Characteristics of headache in pPTH patients
Three out of 17 pPTH patients reported migraine-like headache: it was pulsating, severe, unilateral, and aggravated by physical activity, and rest eased the pain. In addition, concurrent nausea and sensitivity to light occurred. One pPTH patient with migraine-like headache also had tension-type headache. Four of 17 patients reported tension-type headache: the headache was blunt, pressure-type, waved, and rose from the neck to the whole head. There was no sensitivity to sound or light and no nausea or vomiting. One patient of 17 reported facial pain that resembled trigeminal neuralgia. 4/17 patients reported auditory symptoms such as tinnitus or buzz-like sounds and 8/17 patients reported sensitivity to light. For the remaining 5/17 patients, the neurologist had mentioned headache but not described the phenotypes, which thus remain unspecific.
Discussion
Insomnia after injury increased risk for both aPTH and pPTH in this cohort of mTBI patients. Other risk factors for aPTH were headache at ED, other pain, and vertigo. Older age was a risk factor for pPTH. At three months, pPTH patients had a lower full-RTW rate than non-PTH patients.
In our study, the frequency of PTH was comparable to that in a recent study by Yilmaz and colleagues [10], with over half of patients having aPTH and nearly a quarter of them developing pPTH. In previous studies, history of headache and headache at ED have been identified as risk factors for PTH [10, 17, 25] being in line with our findings. Female gender was not associated with risk for PTH in our study, which may be explained by the lower number of patients than in previous studies [10, 17].
Pain other than headache after TBI was detected to be a risk factor for aPTH in our study. Lieba-Samal and colleagues similarly showed that other comorbid chronic pain, which was mostly musculoskeletal pain, was more frequent in aPTH patients compared with non-PTH (p = 0.05) [25]. Ashina and colleagues showed in a recent study that mTBI patients with pPTH rarely suffered from prior chronic pain (11 out of 100 subjects), but in a further 12-month follow-up, a notable proportion of pPTH patients reported frequent occurrence of post-trauma neck pain (78%) and low back pain (37%) [14].
Poor sleep quality and fatigue are some of the most common complaints after TBI and even more frequent among mTBI patients than among those with more severe TBIs [26]. A recent review analyzed the interaction between post-traumatic sleep disturbances and PTH [18]. A bi-directional relation was found: PTH was a risk factor for disrupted sleep, and post-traumatic sleep disruption caused more headaches. Disturbances of sleep were also highlighted in our study population, with aPTH patients suffering significantly more from pre- and post-injury insomnia compared with non-PTH patients. Post-traumatic insomnia was identified as a risk factor for both aPTH and pPTH. The mechanisms by which disrupted sleep and insomnia may worsen PTH remain unclear and need more research in the future.
Voormoolen and colleagues found that post-concussion symptoms (including PTH) were slightly more often reported by those mTBI patients who had trauma findings in brain imaging, that is complicated mTBI [27]. The authors stated that complicated mTBI was eventually only a weak indicator for post-concussion symptoms. Further, in a recent cohort study by Nordhaug and colleagues, pathological imaging findings in brain CT or MRI predicted aPTH, but not pPTH [28]. In our study, trauma findings in brain MRI did not significantly differ between pPTH and aPTH patients. Previous studies and our findings indicate that pathological brain imaging findings are not likely an essential risk factor for PTH.
The negative impact of PTH to RTW was previously studied by Dumken et al. where PTH intensity was measured by using the 0-10 numeric rating scale (NRS) with 0 meaning no headache and 10 the worst imaginable headache pain intensity [29]. The authors reported that each unit increase in headache pain intensity on the NRS reduced the odds of RTW by more than 50%. In a study by Stulemeijer and colleagues, low levels of post-concussion symptoms indicated good recovery and RTW [30]. In line with these studies, we identified that our pPTH patients were less likely to return to full-time work at three months compared with aPTH- and non-PTH patients [9, 10].
Previous studies have indicated increased psychiatric burden in PTH patients [10]. A recent case-control study showed that frequency of depression and anxiety, measured by Beck’s Depression Inventory and the State-Trait Anxiety Inventory, was higher among PTH patients than among patients with migraine or healthy controls [31]. In the present study, the frequency of psychiatric disorders did not differ between the PTH groups. This association should, however, be restudied in a larger cohort of PTH patients.
The phenotype of pPTH is unspecific, but often resembles migraine headaches [14]. In our study, the headache phenotypes were diverse, mostly unclassified type, tension type, or migraine-like headaches. The treatment of pPTH is challenging and multidisciplinary approach is needed, including preventive medications. Novel treatments like CGRP monoclonal antibodies might be an option in the future [16].
Strengths of our study are a well-defined cohort with several follow-up time-points, comprehensive brain imaging, and headache data from the ED.
As a limitation, the cohort is fairly small with many dropouts. Thus, the cohort may not be representative of all PTH patients. A second limitation is a lack of a systematic interview of the headache features at clinical neurological outpatient visits, but we used all the headache data available from the patient records. Thirdly, we did not have questionnaires to evaluate psychological burden and quality of life. However, we performed an extensive SCID-I interview.
Conclusions
Insomnia after injury was associated with increased risk for both aPTH and pPTH in this cohort of mTBI patients. Further, other pain, headache at the ED and vertigo were risk factors for aPTH. With this we conclude that concomitant stress factors (e.g. insomnia and other pain) that are known to trigger also primary headache disorders play a key role in the development of PTH. pPTH and its negative impact to RTW was seen in our study population, highlighting the burden of this secondary headache disorder. Better understanding of the pathophysiology of pPTH is essential and multidisciplinary treatment approach is recommended.
Availability of data and materials
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- aPTH:
-
acute post traumatic headache
- CGRP:
-
calcitonin gene-related peptide
- CT:
-
computed tomography
- ED:
-
emergency department
- GCS:
-
Glasgow Coma Scale
- ICHD:
-
The International Classification of Headache Disorders
- IQR:
-
Interquartile range
- MRI:
-
Magnetic resonance imaging
- mTBI:
-
mild traumatic brain injury
- PTH:
-
post traumatic headache
- pPTH:
-
persistent post traumatic headache
- RPQ:
-
Rivermead post-concussion symptom questionnaire
- RTW:
-
return to work
- SCID-I:
-
Structured Clinical Interview for DSM-IV Axis I disorders
- SD:
-
standard deviation
- TBI:
-
traumatic brain injury
- WHO:
-
World Health Organization
References
Dewan MC, Rattani A, Gupta S et al (2018) Estimating the global incidence of traumatic brain injury. J. Neurosurg Epub ahead of print 1 April 2018. DOI: https://doi.org/10.3171/2017.10.JNS17352
Cassidy JD, Carroll LJ, Peloso PM et al (2004) Incidence, risk factors and prevention of mild traumatic brain injury: results of the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. J Rehabil Med Suppl 43:28–60
Levin HS, Diaz-Arrastia RR (2015) Diagnosis, prognosis and clinical management of mild traumatic brain injury. Lancet Neurol 14:506–517
Peeters W, van den Brande R, Polinder S et al (2015) Epidemiology of traumatic brain injury in Europe. Acta Neurochir 157:1683–1696
Lucas S, Hoffman JM, Bell KR et al (2014) A prospective study of prevalence and characterization of headache following mild traumatic brain injury. Cephalalgia 34(2):93–102
Nordhaug LH, Vik A, Hagen K et al (2016) Headaches in patients with previous head injuries: A population-based historical cohort study (HUNT). Cephalalgia 36(11):1009–1019
Stacey A, Lucas S, Dikmen S et al (2017) Natural history of headache five years after traumatic brain injury. J Neurotrauma 34:1558–1564
Nampiaparampil DE (2008) Prevalence of the chronic pain after traumatic brain injury: A systematic review. JAMA 300(6):711–719
Åhman S, Saveman BI, Styrke J et al (2013) Long-term follow-up of patients with mild traumatic brain injury: a mixed-method study. J Rehabil Med 45:758–764
Yilmaz T, Roks G, de Koning M et al (2017) Risk factors and outcomes associated with post-traumatic headache after mild traumatic brain injury. Emerg Med J 34:800–805
Kontos AP, Elbin RJ, Lau B et al (2013) Posttraumatic Migraine as a predictor of recovery and cognitive impairment after sport-related concussion. Am J Sports Med 41(7):1497–1504
Headache Classification Committee of the International Headache Society (IHS) (2018) ; 38(1):1-211
Kjeldgaard D, Forchhammer H, Teasdale T et al (2014) Chronic post-traumatic headache after mild head injury: A descriptive study. Cephalalgia 34(3):191–200
Ashina H, Iljazi A, Al-Khazali HM et al (2020) Persistent post-traumatic headache attributed to mild traumatic brain injury: Deep phenotyping and treatment patterns. Cephalalgia 40(6):554–564
Ashina H, Porreca F, Anderson T et al (2019) Post-traumatic headache: epidemiology and pathophysiological insights. Nat Rev Neurol 15(10):607–617
Lambru G, Benemei S, Andreou AP et al (2021) Position Paper on Post-Traumatic Headache: The Relationship Between Head Trauma, Stress Disorder, and Migraine. Pain Ther 10:1–13
Hoffman JM, Lucas S, Dikmen S et al (2011) Natural history of headache after traumatic brain injury. J Neurotrauma 28:1719–1725
Piantino J, Lim MM, Newgard CD et al (2019) Linking Traumatic Brain Injury, Sleep Disruption, and Post-Traumatic Headache: a Potential Role for Glymphatic Pathway Dysfunction. Curr Pain Headache Rep 23(62):1–11
Dresler T, Caratozzolo S, Guldolf K et al (2019) Understanding the nature of psychiatric comorbidity in migraine: a systematic review focused on interactions and treatment implications. J Headache Pain 20:51
Van der Naalt J, Timmerman ME, de Koning ME et al (2017) Early predictors of outcome after mild traumatic brain injury (UPFRONT): an observational cohort study. Lancet Neurol 16:532–540
King NS, Crawford S, Wenden FJ et al (1995) The Rivermead Post Concussion Symptoms Questionnaire: A measure of symptoms commonly experienced after head injury and its reliability. J Neurol 242(9):587–592
First BM, Spritzer RL, Gibbon M et al (1997) Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I), Clinician version (Administration booklet). Amer Psychiatric Pub Inc
Marinkovic I, Isokuortti H, Huovinen A et al (2020) Prognosis after Mild Traumatic Brain Injury: Influence of Psychiatric Disorders. Brain Sci 10:916
Holm L, Cassidy JD, Carroll LJ et al (2005) Summary of the WHO Collaborating Centre For Neurotrauma Task Force on Mild Traumatic Brain injury. J Rehabil Med 37(3):137–141
Lieba-Samal D, Platzer P, Seidel S et al (2011) Characteristics of acute posttraumatic headache following mild head injury. Cephalalgia 31(16):1618–1626
Ouellet MC, Beaulieu-Bonneau S, Morin CM (2006) Insomnia in patients with traumatic brain injury: frequency, characteristics, and risk factors. J Head Trauma Rehabil 21(3):199–212
Voormoolen DC, Haagsma JA, Polinder S et al (2019) Post-concussion Symptoms in Complicated vs Uncomplicated Mild Traumatic Brain Injury Patients at Three and Six-months Post-injury: Results from the CENTER-TBI Study. Journal of Clinical Medicine 8:1921
Nordhaug LH, Linde M, Follestad T et al (2019) Change in Headache Suffering and Predictors of Headache after Mild Traumatic Brain Injury: A Population-Based, Controlled, Longitudinal Study with Twelve- Month Follow-Up. J Neurotrauma 36(23):3244–3252
Dumke HA (2017) Posttraumatic Headache and Its Impact on Return to Work After Mild Traumatic Brain Injury. J Head Trauma Rehabil 32(2):E55–E65
Stulemeijer M, van der Werf S, Borm GF et al (2008) Early prediction of favourable recovery 6 months after mild traumatic brain injury. J Neurol Neurosurg Psychiatry 79:936–942
Schwedt TJ, Chong CD, Peplinski J et al (2017) Persistent post-traumatic headache vs. migraine: an MRI study demonstrating differences in brain structure. J Headache Pain 18(1):87
Funding
This study was funded by the grant of Helsinki and Uusimaa Hospital District. Open access funded by Helsinki University Library.
Author information
Authors and Affiliations
Contributions
Hanna Harno and Susanna Melkas designed the study. Kaisa Mäki, Ivan Marinkovic, Taina Nybo, Harri Isokuortti, Antti Korvenoja, Antti Huovinen and Susanna Melkas collected the data. Yvonn Kraemer analyzed the data and prepared figures and tables. Yvonn Kraemer wrote the first draft of the manuscript. All authors contributed to the interpretation of data and writing of the manuscript. All authors approved the submitted version and have agreed both to be personally accountable for the author’s own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the Helsinki University Hospital and conducted according to the Declaration of Helsinki. Informed consent was received from each subject.
Consent for publication
Consent for publication was received.
Competing interests
Hanna Harno has provided consultancy to TEVA, Allergan, and Lilly, unrelated to this work. None of the other co-authors have conflicts of interest to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kraemer, Y., Mäki, K., Marinkovic, I. et al. Post-traumatic headache after mild traumatic brain injury in a one-year follow up study – risk factors and return to work. J Headache Pain 23, 27 (2022). https://doi.org/10.1186/s10194-022-01398-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s10194-022-01398-9