
Abstract
Background
Present study describe the in vitro model of plasma oxidation of patients with different lipid profile, that can be correlated to their invivo plasma oxidizability in order to find the arterial diseases prone patient groups.
Method
The method applied here to measure the invitro plasma oxidizability, accounts a convenient way that can be well suited in any clinical laboratory settings. Un-fractionated plasma was exposed to CuSO4 (5.0 mmol/L), a pro-oxidant, and low frequency ultrasonic wave to induce oxidation, and finally oxidizability was calculated by TBARS and Conjugated Diene methods.
Result
In our study, plasma LDL greater than 150 mg/dL possess 1.75 times more risk to undergo oxidation (CI, 0.7774 to 3.94; p = 0.071) than the low LDL plasma, percent of oxidation increased from 38.3% to 67.1% for the LDL level upto 150 mg/dL and high. Lag phase, which is considered as the plasma antioxidative protection, was also influenced by the higher LDL concentration. The mean lag time was 65.27 ± 20.02 (p = 0.02 compared to healthy), where as for 94.71 ± 35.11 min for the normolipidemic subject. The plasma oxidizability was also changed drastically for total cholesterol level, oxidative susceptibility shown 35% and 55.02% for 200 mg/dL and high respectively, however it didn’t appear as risk factor. Patient samples were also stratified according to their age, gender, and blood glucose level. Older persons (≥40 years) were 1.096 times (95% CL, 0.5607 to 2.141, p = 0.396) than younger (≤39 years age), males are 1.071 (95% CI, 0.5072- 2.264) times than the females, and diabetic patients are 1.091 (CI, 0.6153 to 1.934, p = 0.391) times in more risk than the non-diabetic counterpart.
Conclusion
This method addressing its easy applicability in biomedical research. And by this we were able to show that patients with high LDL (≥150 mg/dL) are in alarming condition besides diabetic and elderly (≥40 years age) males are considered to be susceptible and more prone to develop vascular diseases.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The clinical importance of lipid oxidation, mainly low density lipoproteins (LDLs) is presumably associated with atherosclerosis formation [1]. Though in biological model it is not easy to show the pathological process of atherosclerosis, however the in vitro oxidizability of patients’ plasma could be extrapolated to assess the susceptible patient group [2]. Many studies has shown the Cu2+ mediated oxidation of isolated LDL and fatty acids [2–4], even in unfractionated plasma [2]. We have exercised here also the same protocol to study the unfractionated plasma in the presence of CuSO4, but there was not enough differences observed in plasma lipid oxidation between presence and absence of CuSO4 alone. We made a slight modification by exposing them in ultrasonic wave so that the lipid portion in the solution would be favorable in size to undergo the oxidative modification.
Several epidemiological investigations implicate the relationship between high cholesterol level with new onset of coronary heart disease (CHD) [5–8] in patients who were not previously affected, and newly appearance of coronary artery disease in recognized CHD patients [9–11]. From their results it appeared that the level above 100 mg/dL of LDL cholesterol is atherogenic. In contrast, it also shown that people with low level of cholesterol are less prone to develop atherosclerosis and CHD [12–14]. So there is a positive relationship observed between serum cholesterol level and CHD. But the threshold level for this relationship is not very much straightforward. Again some populations were free from CHD by maintaining below 150 the total cholesterol or below 100 mg/dL LDL cholesterol level [15–18]. In case of higher cholesterol level with young adults were found increased chances to develop CHD in later stage of their life [19, 20]. On the other hand, low HDL level also posses the risk of developing CHD, though it holds the independent relationship. In genetically modified animal model, it appears that the higher level of HDL protects it against atherogenesis [21–23] and deficiency of HDL exacerbates it [24, 25]. Moreover the antioxidant and anti-inflammatory effect of HDL can also impart the anti-atherogenic role [26, 27]. So, there is a lot of published work to support the role of lipoproteins on oxidative stress but the oxidative susceptibility status with different types of lipoproteins and cholesterol levels in patient’s plasma has not been studied in detail.
To address the susceptibility value of patients’ unfractionated plasma lipid in terms of their plasma lipid profile as a prototype for the ex vivo lipid oxidation, we have developed a very convenient and less equipped model to assess data in large scale. We hypothesized that plasma lipid oxidizability would be sensitive with the following parameters: level of lipoproteins, cholesterol, triglycerides, age, diabetes mellitus and sex. In order to test this hypothesis, we carried out three studies- firstly we examined the plasma lipid profile and then in vitro plasma lipid oxidation following conjugation diene formation and TBARS formation, in the presence of Cu++ ion with occasional exposure of ultrasonic wave.
Methods
Sample collection
Study subjects included 45 male and female (35 – 75 years old). Among them, 19 were with LDL level was higher than 100 mg/dL, 14 individuals with greater than 150 mg/dL level of total cholesterol, 18 individuals with lower than 35 mg/dL of HDL, number of young patients (age below 40 years) were 23 and older (above 40 years) 22, whereas patients with diabetes mellitus were 15. Peripheral venous blood samples of all patients’ were collected on heparin (5 U/ml) from subjects with 12 hours fasting. Plasma was separated by 5 min centrifugation at 4000 rpm immediately after collection. Data acquisition were completed on the same day, alternatively, the samples were stored at 4°C for 24 hours or at -20°C for not more than 2 days. Informed consent form was made and approved according to the recommendation of the University Medical Research Ethical Committee of the Faculty of Science, Primeasia University, Dhaka, Bangladesh, where the objective of this study and use of biological samples were clarified.
Biochemical analysis
Blood glucose, total cholesterol (TC), triglyceride (TG) and HDL level were estimated following the standard laboratory methods using 3000-Evolution analyzer (Italy). And Friedewald’s formula [28] was applied for LDL estimation.
Plasma oxidizability measurement following thiobarbituric acid reactive substance formation (TBARS) method
TBARS formation was measured following the method described by Adriana E Scoccia [3], malonaldihyde, a secondary metabolite and a marker of lipid peroxidation and oxidative stress, which reacts with Thiobarbituric Acid (TBA) to yield pink colored complex that can be measured spectophotometrically. Briefly, 50 μL plasma was diluted in 10 mL CuSO4 (5.0 mmol/L)solution and incubated at 37°C for 3 hours in ultrasonic waterbath with occasional exposure of ultrasonic wave (SonoSWISS SW6 H, Switzerland) to allow the oxidation process. Then 0.5 mL of 0.78% aqueous solution of thiobarbituric acid and 50 μL of acetic acid was added in 0.5 mL of the plasma-CuSO4 mixture. Control was prepared in the same way except CuSO4. The mixture was heated at 80°C for 40 min in a ultrasonic waterbath and absorbances were taken at 532 nm using a spectrophotometer (SHIMADZU UV 1650 pc, UV–vis. Spectrophotometer, Japan). Percentage of oxidation was calculated as follows-
Where Aps is the absorbance of plasma sample, Ac is absorbance of control.
Plasma oxidizability measurement following conjugated diene method
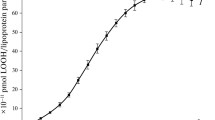
Conjugated diene was measured following a slight modification of the method described by Kontush and Beisiegel [29], where photometrical detection is employed for the conjugated diene. In brief, 50 μL plasma was diluted to 10 mL phosphate-buffered saline, to which CuSO4 was added to make the concentration 5.0 mmol/L. In another tube, 5.0 mmol/L CuSO4 in phosphate-buffered saline was served as a blank. Samples, in cuvettes, after a brief exposure of ultrasonic wave were incubated in spectrophotometer (SHIMADZU UV 1650 pc, UV–vis. Spectrophotometer, Japan) for 160 min, where sample absorbance was measured at 234 nm in every 2 min interval. Lag phase was considered for the time taken with no increment of absorbance before a rapid oxidation. The duration of lag phase indicate the resistance to oxidation. CDmax was calculated from the maximum absorbance value and the Beer-Lambert law, where the extinction coefficient for conjugated diene is 29500 L.mol/cm [4].
Statistical analysis
Results are presented as interquartile ranges or as means ± SDs. Statistical analysis between normal and test group was performed using Microsoft Excel 2007 and data were compared with unpaired two tailed t-test. Risk ratio within 95% confidence interval was calculated using Openepi_37V software (http://www.openepi.com). Mid p-exact was taken, where p value threshold was used ≤0.05 to indicate a statistical significant.
Result and discussion
In this in vitro Cu++ and ultrasonic wave mediated oxidative susceptibility assay, first we compared the TBARS level by incubating tube containing patients’ plasma with CuSO4 at 37°C in normal waterbath for 3 hours. Having not any comparable data between treated and untreated sample, we slightly modified the method by exposing ultrasonic wave during this incubation period and a comparable data was generated (Figure 1). This modified method for TBARS assay was exercised throughout the experiment. We observed the percent oxidizability in terms of plasma cholesterol level (Figure 2A) for the first two subgroups were fairly similar, 36.95% and 35.60% respectively for plasma below 150 and 150–200 mg/dL, but it jumped to 55.02% for the patients with higher than 200 mg/dL, although not significantly (p = 0.124) compared to the oxidative susceptibility of 150 mg/dL. However, the risk ratio appeared not so high, 1.003.

Comparative oxidation of unfractionated plasma by incubating in two different conditions at 37°C , here SSWB means Sono Swiss water bath with ultrasonic wave exposure, and NWB means normal water bath. Bars are presented; mean (absorbance) ± SD. Difference in oxidation of plasma between presence and absence of Cu2+ in ultrasonic bath was significant.

Plasma oxidizability with different plasma profile. (A) Plasma oxidizability in terms of total cholesterol level. (B) Plasma oxidizability in terms of different LDL concentration, which was significantly higher in plasma with highest LDL level than intermediate level (p = 0.0068) and lower level (p = 0.007). (C) Plasma oxidizability of different samples with different HDL level. Oxidizability is shown by mean (percent of basal) ± SD.
Similar trend was observed comparing the plasma LDL level, which appeared as 32.70 and 38.30% in case of 100 mg/dL and 100–150 mg/dL subgroup, respectively compared to the control. But it rose as high as 67.18 percent for LDL level ≥150 mg/dL, which was statistically significant compared to the other two subgroups (Figure 2B. p-values were 0.007 for both cases). This result was supported by the findings of other group’s reporting [3], where TBARS formation was linearly increased with increasing volume of LDL. And the risk ratio demonstrate that higher LDL level indulge patients in a condition which is 1.75 times more likely to occur arterial diseases than the low LDL level; the 95% confidence interval around this estimate is 0.7774, 3.94 (p = 0.071).
In Figure (2C) the bar chart compares the serum oxidative susceptibility in terms of their plasma HDL concentration. The mean susceptibility was 47.04 and 37.05% for the people with less than 35 and greater that 35 mg/dL of HDL level in their serum.
People with diabetes mellitus were shown to possess higher plasma oxidizability by both TBARS and CDmax result (Table 1), and are 1.091 time more in chance to develop arterial disease than the non-diabetic group, with a 95% confidence interval of 0.6153 to 1.934.
An analysis between male and female and between younger (age below 40) and older (above 40) (Table 1), not considering their diabetes status, showing that the risk ratio for males is 1.071 (95%, CI 0.5072- 2.264) and for older is 1.096 (0.5607 to 2.141). But none of these results were statistically significant.
There is not much differences are showing in plasma oxidizability between male and female in terms of their TBARS formation. However, it gave statistically significant difference in conjugated diene formation. Turning to the reasons for the higher value to CDmax, there were almost half of the women in the presented data were hyperlipidemic. A circuitous role of oxygen free radical formation from polymorphonuclear leukocytes and monocytes in hyperlipidemic subject have previously been described [30].
Mean lag phase are declined in patients with high LDL and total plasma cholesterol level (Figure 3). The downward shift, presented in lag phase with LDL and total cholesterol level higher than 100 and 150 mg /dL, are statistically significant (p = 0.02 and 0.05, respectively, compared to healthy volunteer who were normolipidemic). Antioxidant defense, attributed mainly by the lipophilic antioxidant vitamin E, and other vitamins play role in the lag phase, which is increased by the presence of these vitamins [2, 31]. Surprisingly, the mean lag phase of patients with low HDL level are shown to possess high values. The upward shift is present at even the higher (75th) percentile in case of HDL value ≤35 mg/dL. Thus, the upward shift of lag phase in ≤35 mg/dL HDL level is not solely attributed to the lower amount of HDL present in the plasma but must have resulted from the influence of other parameters.

Box plot of lag-time in conjugated diene assay. The boxplot shows variable range of Lag time in conjugated diene assay, median values were 86.00, 82.00, 72.00 and 62.00 for healthy, patient group with less than 35mg/dL HDL, greater than 150 mg/dL cholesterol and ≥100 mg/dL LDL level, with average values 94.71, 88.72, 71.25 and 65.27 respectively.
No doubt the lowering of LDL and total cholesterol should be the primary goal for patients with CHD, but it could be beneficial knowledge for general patients’ if their plasma lipid oxidizability values are explained in a simpler way. Unlike the other methods where fractioning LDL or HDL by ultracentrifugation, dialysis, electrophoresis etc. need much effort. Also the oxidation study with isolated lipoproteins may raise question about it’s in vivo comparability [2]. Again this method offers a easy alternative, and substantial data can be generated with less equipped and simple methodological approach like it which is clinically relevant. The increase in TBARS and reduction in CD indicating the less antioxdative protection and high oxidative stress. Data might be influenced by dietary and drug treatment, since the history were not taken. However, standardized experimental condition including randomization, minimum delaying in data acquisition and triplicate sampling outweigh possible obstacles. We conclude that patients with high LDL (≥150 mg/dL) are in alarming condition besides diabetic patients, and elderly (age above 40 years) males are considered to be susceptible and more prone to develop vascular diseases.
References
Steinbergt D: Low density lipoprotein oxidation and its pathobiological significance. J Biol Chem 1997, 272: 20963–20966. 10.1074/jbc.272.34.20963
Mark AA, Amy G, Raj U, Hilary JP: Oxidative susceptibility of unfractionated serum or plasma: response to antioxidants in vitro and to antioxidant supplementation. Clin Chem 2005, 51: 2138–2144. 10.1373/clinchem.2005.051078
Adriana ES, María SM, Antonio DM, Ana MC: A simple method to assess the oxidative susceptibility of low density lipoproteins. BMC Clin Pathol 2001, 1: 1. 10.1186/1472-6890-1-1
Kleinveld HA, Hak-Lemmers HLM, Stalenhoef AFH, Demacker PNM: Improve measurement of low-density lipoproteinsusceptibility to copper-induced oxidation: application of a short procedure for isolating low-density lipoprotein. Clin Chem 1992, 38: 2066–2072.
Wilson PWF, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB: Prediction of coronary heart disease using risk factor categories. Circulation 1998, 97: 1837–1847. 10.1161/01.CIR.97.18.1837
Stamler J, Wentworth D, Neaton JD: Is relationship between serum cholesterol and risk of premature death from coronary heart disease continuous and graded? Findings in 356 222 primary screenees of the Multiple Risk Factor Intervention Trial (MRFIT). JAMA 1986, 256: 2823–2828. 10.1001/jama.1986.03380200061022
Lipid Research Clinics Program: The lipid research clinics coronary primary prevention trial results. I. JAMA 1984, 251: 351–364.
Lipid Research Clinics Program: The lipid research clinics coronary primary prevention trial results. II. JAMA 1984, 251: 365–374.
Rossouw JE, Lewis B, Rifkind BM: The value of lowering cholesterol after myocardial infarction. N Engl J Med 1990, 323: 1112–1119. 10.1056/NEJM199010183231606
Pekkanen J, Linn S, Heiss G, Suchindran CM, Leon A, Rifkind BM, Tyroler HA: Ten-year mortality from cardiovascular disease in relation to cholesterol level among men with and without preexisting cardiovascular disease. N Engl J Med 1990, 322: 1700–1707. 10.1056/NEJM199006143222403
Wong ND, Wilson PWF, Kannel WB: Serum cholesterol as a prognostic factor after myocardial infarction: the Framingham Study. Ann Intern Med 1991, 115: 687–693. 10.7326/0003-4819-115-9-687
McGill HC Jr: Introduction to the geographic pathology of atherosclerosis. Lab Invest 1968, 18: 465–467.
Keys A, Arvanis C, Blackburn H: Seven Countries: A Multivariate Analysis of Death and Coronary Heart Disease. Cambridge, MA: Harvard University Press; 1980:381.
Keys A, Menotti A, Aravanis C, Blackburn H, Djordjevic BS, Buzina R, Dontas AS, Fidanza F, Karvonen MJ, Kimura N, Mohacek I, Nedeljkovic S, Puddu V, Punsar S, Taylor HL, Conti S, Kromhout D, Toshima H: The Seven Countries Study: 2,289 deaths in 15 years. Prev Med 1984, 13: 141–154. 10.1016/0091-7435(84)90047-1
Law MR, Wald NJ, Thompson SG: By how much and how quickly does reduction in serum cholesterol concentration lower risk of ischaemic heart disease? BMJ 1994, 308: 367–372. 10.1136/bmj.308.6925.367
Law MR: Lowering heart disease risk with cholesterol reduction: evidence from observational studies and clinical trials. Eur Heart J Suppl 1999, 1(suppl):S3-S8.
Grundy SM, Wilhelmsen L, Rose G, Campbell RWF, Assmann G: Coronary heart disease in high-risk populations: lessons from Finland. Eur Heart J 1990, 11: 462–471.
People’s Republic of China-United States Cardiovascular and Cardiopulmonary Epidemiology Research Group: An epidemiological study of cardiovascular and cardiopulmonary disease risk factors in four populations in the People’s Republic of China: baseline report from the P.R.C.-U.S.A. Collaborative Study. Circulation 1992, 85: 1083–1096.
Anderson KM, Castelli WP, Levy D: Cholesterol and mortality: 30 years of follow-up from the Framingham Study. JAMA 1987, 257: 2176–2180. 10.1001/jama.1987.03390160062027
Klag MJ, Ford DE, Mead LA, He J, Whelton PK, Liang KY, Levine DM: Serum cholesterol in young men and subsequent cardiovascular disease. N Engl J Med 1993, 328: 313–318. 10.1056/NEJM199302043280504
Rubin EM, Krauss RM, Spangler EA, Verstuyft JG, Clift SM: Inhibition of early atherogenesis in transgenic mice by human apolipoprotein AI. Nature 1991, 353: 265–267. 10.1038/353265a0
Plump AS, Scott CJ, Breslow JL: Human apolipoprotein A-I gene expression increases high density lipoprotein and suppresses atherosclerosis in apolipoprotein E-deficient mouse. Proc Natl Acad Sci U S A 1994, 91: 9607–9611. 10.1073/pnas.91.20.9607
Tangirala RK, Tsukamoto K, Chun SH, Usher D, Puré E, Rader DJ: Regression of atherosclerosis induced by liver-directed gene transfer of apolipoprotein A-I in mice. Circulation 1999, 100: 1816–1822. 10.1161/01.CIR.100.17.1816
Ng DS, Vezina C, Wolever TS, Kuksis A, Hegele RA, Connelly PW: Apolipoprotein A-I deficiency: biochemical and metabolic characteristics. Arterioscler Thromb Vasc Biol 1995, 15: 2157–2164. 10.1161/01.ATV.15.12.2157
Miller M, Aiello D, Pritchard H, Friel G, Zeller K: (Leu159 → Pro): HDL cholesterol deficiency in a kindred associated with premature coronary artery disease. Arterioscler Thromb Vasc Biol 1998, 18: 1242–1247. 10.1161/01.ATV.18.8.1242
van Lenten BJ, Hama SY, de Beer FC, Stafforini DM, McIntyre TM, Prescott SM, La Du BN, Fogelman AM, Navab M: Anti-inflammatory HDL becomes pro-inflammatory during the acute phase response: loss of protective effect of HDL against LDL oxidation in aortic wall cell cocultures. J Clin Invest 1995, 96: 2758–2767. 10.1172/JCI118345
Navab M, Hama SY, Anantharamaiah GM, Hassan K, Hough GP, Watson AD, Reddy ST, Sevanian A, Fonarow GC, Fogelman AM: Normal high density lipoprotein inhibits three steps in the formation of mildly oxidized low density lipoprotein: steps 2 and 3. J Lipid Res 2000, 41: 1495–1508.
Friedewald WI, Ley RI, Fradrickson DS: Estimation of concentration of low density lipoprotein cholesterol in plasma without the use of preparative ultracentrifuge. Clin Chem 1972, 18: 494.
Kontush A, Beisiegel U: Measurement of oxidizability of blood plasma. Methods Enzymol 1999, 299: 35–49.
Prasad K: Atherosclerosis, Hypocholesterolemic and antiatherosclerotic effect of flax lignan complex isolated from flaxseed. Atherosclerosis 2005, 179: 269–275. 10.1016/j.atherosclerosis.2004.11.012
Bruno P, Odile M, Raymond B, Jean B, Jacques C, Isaac M: Conjugated dienes: a critical trait of lipoprotein oxidizability in renal fibrosis. Nephrol Dial Transplant 2001, 16: 1598–1606. 10.1093/ndt/16.8.1598
Acknowledgements
We are grateful to the following institutions for this research support: Primeasia University and Exim Bank Hospital.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
Research concept, data analysis & writing: HI; Patient sample and data acquisition: AC NM and AH; Coordination: FBK and MBU; Oversaw the study design and helped in drafting the manuscript: MMRS; Instrumental support: AH. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Imam, H., Chowdhury, A., Mahbub, N.U. et al. Oxidizability assay of unfractionated plasma of patients’ with different plasma profile: a methodological study. J Diabetes Metab Disord 13, 54 (2014). https://doi.org/10.1186/2251-6581-13-54
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/2251-6581-13-54