
Abstract
Objectives
A public-private partnership in Tanzania launched the accredited drug dispensing outlet (ADDO) program to improve access to quality medicines and pharmaceutical services in rural areas. ADDO dispensers play a potentially important role in promoting the rational use of antimicrobials, which helps control antimicrobial resistance (AMR). The study objectives were to 1) improve dispensing practices of antimicrobials, 2) build ADDO dispensers’ awareness of the consequences of misusing antimicrobials, and 3) educate consumers on the correct use of antimicrobials through the use of printed materials and counseling.
Methods
Our intervention targeted ADDO dispensers and community members in Kilosa district. We promoted AMR awareness using posters hung in public places, health facilities, and ADDOs; sensitizing 84 health care providers on AMR issues; and providing training and on-site support for 124 ADDO dispensers to increase their AMR knowledge and dispensing skills. Baseline and endline assessments included direct observation of dispensers’ practices; interviews with ADDO dispensers (71 at baseline and 68 at endline) regarding dispensing experiences; 230 exit interviews with ADDO customers regarding use of antimicrobials during monitoring visits; and review of ADDO records. Indicators were based on product availability, dispensing practices, customers’ knowledge of how to take their medicines, and dispenser and public awareness of the AMR threat.
Results
Availability of tracer antimicrobials increased by 26% (p = 0.0088), and the proportion of ADDOs with unauthorized items decreased from 53% to 13% (p = 0.0001). The percentage of ADDO dispensers following good dispensing practices increased from an average of 67% in the first monitoring visit to an average of 91% during the last visit (p = 0.0001). After the intervention, more dispensers could name more factors contributing to AMR and negative consequences of inappropriate antimicrobial use, and over 95% of ADDO customers knew important information about the medicines they were dispensed.
Conclusions
Providing educational materials and equipping ADDO dispensers with knowledge and tools helps significantly improve community medicine use and possibly reduces AMR. The number of community members who learned about AMR from ADDO dispensers indicates that they are an important source of information on medicine use.
Similar content being viewed by others


Introduction
Many people in sub-Saharan Africa seek health care from the private sector for reasons such as convenience and better availability of medicines [1]. People who use drug shops and pharmacies come in requesting specific medicines for self-treatment or advice from the drug seller on treatment or with a prescription to fill from a health care provider [2–4]. Therefore, retail drug sellers may be first people’s contact regarding health care for themselves or their children if that is their primary medicine source [5].
Historically in Tanzania, the local retail drug shop called duka la dawa baridi was authorized by the Tanzania Pharmacy Board to provide nonprescription medicines in the private sector. However, a 2001 assessment showed that many shops sold prescription drugs illegally and that drug sellers were generally unqualified and untrained [6]. In response, the Strategies for Enhancing Access to Medicines Program, funded by the Bill & Melinda Gates Foundation, collaborated with the Tanzania Food and Drugs Authority (TFDA) to develop and launch the accredited drug dispensing outlet (ADDO) program in 2003. The program’s goal was to improve access to affordable, quality essential medicines and pharmaceutical services in the duka la dawa baridi, which were mainly located in areas where few or no registered pharmacies exist. To achieve this goal, the program took a holistic approach that combined training, accreditation, business incentives, and regulatory enforcement with efforts to increase consumer demand for quality products and services. A key incentive for owners to become accredited was to legally allow ADDO dispensers to sell a limited list of essential prescription-only antimicrobials [7].
Successful results of the pilot in Tanzania’s Ruvuma region provided proof that ADDOs could improve access to quality medicines and pharmaceutical services [8]. Based on program evaluations, the Ministry of Health and Social Welfare approved a plan to roll out the ADDO concept in mainland Tanzania. As the program has taken off, many have recognized the potential of ADDOs not only to increase access to essential medicines, but also to serve as a platform for community-based public health interventions, such as distributing subsidized antimalarials [9]. As a result, numerous organizations and programs have played a role in expanding both the services that ADDOs provide and their geographic reach—over 6,000 ADDOs currently serve all mainland regions in Tanzania [10].
As a major source of essential medicines and health services in the community, ADDO dispensers play a potentially important role in promoting rational use of antimicrobials, which helps control antimicrobial resistance (AMR). Poor antimicrobial use includes overuse, prescription of wrong antimicrobials, and not taking a full dose of the dispensed medicines [11, 12]. As part of an initiative to support advocacy and containment of AMR in the community, the U.S. Agency for International Development-funded Strengthening Pharmaceutical Systems Program focused on ADDOs. Our objectives were to improve ADDO dispensers’ antimicrobial dispensing and counseling practices by providing training, job aids, educational materials, and regular supervision and to increase awareness of AMR in the surrounding community.
Methods
Study sites
Our intervention targeted ADDO dispensers and community members in Kilosa district, which is in the western part of the Morogoro region with a population of 438,175 people [13]. Kilosa has 50 public health facilities, 18 private clinics, and 125 ADDOs. We promoted AMR awareness using posters hung in public places, health facilities, and ADDOs; sensitizing 84 health care providers on AMR issues; and providing training and on-site support for 124 ADDO dispensers to increase their AMR knowledge and dispensing skills.
Data collection and analysis
We performed baseline and endline assessments before and after the AMR intervention. In addition, as part of the on-site supervisory monitoring strategy, we collected data using a combination of review of dispensing records, in-person interviews with dispensers and ADDO customers, and observation of customer encounters. The data collected was used to help track progress during the intervention based on six indicators to measure the ADDO dispensers’ ability to:
-
(1)
Correctly interpret a prescription brought in by the client
-
(2)
Appropriately prepare needed medicines to dispense
-
(3)
Provide correct instructions to clients on how to use the dispensed medicines
-
(4)
Provide information on the medicine’s possible side effects
-
(5)
Provide other information if appropriate
-
(6)
Double-check the clients’ understanding of the information they received regarding correct medicine use
We used the same data collection instrument for the baseline and endline assessments, and a different instrument during the three monitoring visits. Pharmacy students collected baseline and endline data, and pharmacist or medical professionals conducted the three supervisory visits. A list of 14 tracer antimicrobials was used to assess availability of antimicrobials that ADDOs are legally allowed to stock. Table 1 summarizes the data gathering activities.
We analyzed the data using Excel. Prior to collecting data, we sought approval from the TFDA and Pharmacy Council. After being briefed on the purpose of the study, ADDO dispensers were asked to participate and upon consent were interviewed. Data collectors verbally assured participants of the confidentiality of information collected, their anonymity, and the freedom to withdraw at any time during the process. Additionally, prior to data collection, we held meetings with district officials to brief them about the study.
Baseline assessment
In August 2008, we did a baseline assessment of ADDO dispensing practices, dispensers’ knowledge of factors that contribute to the development of AMR and consequences of inappropriate use of antimicrobials. Using a structured questionnaire, we interviewed 71 ADDO dispensers from randomly chosen shops in the district. In addition, we reviewed ADDO dispensing records and observed dispensing practices. We used the information gathered during the baseline survey to design the intervention. An endline assessment in October 2010 determined if the intervention had changed behavior of ADDO dispensers and improved appropriate use of antimicrobials.
Job aids and educational materials
We developed job aids including an antimicrobial dispensing guide, counter-top cards with information for customers on one side and information for ADDO dispensers on the other, and rubber stamps to label medicine packages and help dispensers provide counseling on appropriate use of antimicrobials at home. The information on the stamp included the patient’s name, the medicine name, strength, and quantity dispensed, how to take the medicine, the date dispensed, and the ADDO name. A poster featured information in Kiswahili to increase awareness of AMR and appropriate medicine use among the public. The materials were pretested with both dispensers and community members. Two thousand public information posters were displayed in all ADDOs, all the district’s health facilities, and public gathering places, and 300 counter-top cards, 300 dispensing guides, lists of prescription medicines ADDOs are authorized to dispense, and rubber stamps were distributed to all the ADDOs in the district.
Sensitization seminars
We collaborated with TFDA and the Kilosa district pharmacist to launch and distribute the job aids and educational materials to 124 ADDO dispensers (99% of total), prescribers from all 84 health facilities in Kilosa, and 8 members of the district’s Council Health Management Team, who are responsible for supervising health facilities and ADDOs. During the December 2009 seminar, we shared the AMR baseline assessment results and presented the new materials for participants to discuss. At the end of the seminar, participants received printed materials to take to their work places. District health staff also received a supervision checklist to help support ADDO dispensers on issues related to AMR.
Follow-up monitoring visits
We conducted 3 visits in the 10 months after the intervention launch to provide on-site support to ADDO dispensers, to collect monitoring information from ADDOs, to interview ADDO customers, and to continue to distribute materials to health facilities and other public gathering places in the district. The visits to 81, 93, and 88 individual ADDOs were conducted in March, June, and October 2010, respectively; at those times, we provided on-site supervision to 93, 101, and 110 dispensers. During the visits, ADDO dispensers were reminded to follow good dispensing practices such as—
-
Reviewing customer’s prescription
-
Writing the correct information on medication labels
-
Packaging medications from containers using clean equipment and not hands
-
Providing accurate instructions on medicine use to customers
-
Checking customers’ understanding by asking for feedback
To assess whether ADDO dispensers used these good dispensing practices, we observed interactions with customers or checked dispensers’ knowledge using a structured checklist, which had been pretested. We also carried out exit interviews with 80, 92, and 58 ADDO customers after each monitoring visit to measure their awareness regarding AMR and to learn about their experiences with the dispenser.
Endline assessment
In October 2010, 10 months after the start of the intervention, we conducted an endline evaluation to determine the intervention’s results, to highlight challenges encountered during the implementation, and to provide recommendations that would help guide future intervention scale-up plans. The survey comprised assessment data from 65 ADDOs, including interviews with 68 dispensers, using a structured questionnaire to assess dispensers’ knowledge about AMR and its contributing factors and knowledge about the negative consequences of inappropriate antimicrobial use. We included all of the same 71 randomly selected ADDOs at the baseline assessment, but six shops were closed.
Dissemination workshop
After the endline data analysis, we organized a one-day dissemination workshop with 50 key stakeholders to share findings from the AMR activities. Stakeholders included ADDO dispensers and owners, health facility staff, and Kilosa district community members. Participants also included representatives from TFDA, National Malaria Control Program, Pharmacy Council, Ministry of Health and Social Welfare, other implementing partners, and the Muhimbili University School of Pharmacy. In addition to sharing the evaluation results, we used the meeting as a forum to discuss options and recommendations regarding a strategy for possible scale-up.
Results
To measure success or failure of the ADDO AMR initiative, throughout the implementation period we monitored changes based on the six indicators mentioned above. Indicators addressed product availability, dispensing practices, and dispenser and customer and public knowledge of AMR issues.
Availability of antimicrobials
Monitoring results showed an increase in availability of these antimicrobials from an average of 62% at the first monitoring visit to an average of 78% at the last monitoring visit (p = 0.0088). In addition, during monitoring visits, dispensers were reminded to stop stocking antimicrobials that are not allowed. As a result, availability of unauthorized medicines decreased significantly (p = 0.0001) (Table 2).
Dispensing practices
After the intervention, results showed that the percentage of ADDO dispensers using good dispensing practices increased from an average of 67% in the first follow-up visit to an average of 91% during the last follow-up visit (p = 0.0001). That means almost all dispensers met all six indicators of good dispensing practices as recommended in the dispensing guide, thereby ensuring that customers received the correct instructions for using medicines.
Correct labeling
A correct medicine label helps remind a customer of how to take the dispensed antimicrobials appropriately. During the baseline assessment, 18% of ADDO dispensers were using rubber stamps for labeling. However, the stamps were not uniform, and some lacked important information. Consequently, we distributed standardized rubber stamps for medicine labeling during the first follow-up visit and then assessed dispensers’ appropriate use of the stamps in the second and third follow-up visits. When we interviewed customers exiting ADDOs, we checked to see whether their medicine labels included the name of the medicine, strength, and instructions for use. At the second monitoring visit, 95% of the packages included the name of the medicine; 77% included the strength, and 93% included instructions for use; at the third visit, the proportions were 98%, 91%, and 98%, respectively.
Counseling information
The intervention focused on educating dispensers on the importance of providing adequate instructions for medicine use to customers and how these instructions and medicine use influence AMR. At endline, the majority of dispensers who were interviewed (an average of 89%) were aware of the important information to be covered when dispensing medicines to customers compared to 58% of dispensers during the baseline assessment (p = 0.0002) (Table 3).
Customers’ knowledge of how to take dispensed medicines
We then collected information on ADDO customers’ knowledge of how to properly take their medicines including dose (quantity), dosage (number per day), and course (duration) of the medicine that they had been dispensed. The results from data collected from ADDO customers during monitoring visits showed that ADDO dispensers improved the quality of their counseling, so that customers were able to understand how to properly take the antimicrobials they had been dispensed (Table 4).
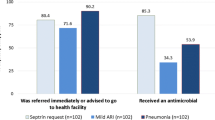
Appropriate treatment of common health conditions
Although ADDOs are allowed to sell and dispense select antibiotics used to treat common conditions, dispenser training emphasizes appropriate use, including not recommending antimicrobials to treat conditions such as acute upper respiratory infections and uncomplicated nonbloody diarrhea, which do not require antibiotics. Results from reviews of dispenser-managed treatment records during the three follow-up monitoring visits showed statistically significant improvements; for example, dispensing antibiotics for nonbloody diarrhea decreased from 37% at the first visit to 12% at the last visit (p = 0.0002), as indicated in Figure 1. Similar decreases in inappropriate treatment of acute upper respiratory infections occurred over the monitoring period (p = 0.0088).

Percentage of ADDO dispensers who appropriately did not dispense antibiotics for common conditions.
Dispensers’ awareness of consequences of inappropriate antimicrobial use and factors contributing to AMR
Overall, at endline, the dispensers included more negative effects in their lists of the consequences for inappropriate medicine use (five compared with three at baseline), and a higher percentage of dispensers mentioned each consequence (Figure 2).

Percentage of ADDO dispensers listing negative consequences of inappropriate antimicrobial use.
In addition, ADDO dispensers’ awareness of factors that contribute to AMR increased as a result of the sensitization and follow-up visits. After the intervention, a higher percentage of dispensers could name more AMR factors (Table 5).
Discussion
The ADDO program is an innovative public-private partnership that increases access to quality pharmaceuticals and services—especially in rural and periurban locations. This project demonstrated the feasibility of using the ADDO platform to translate the World Health Organization’s strategy to control AMR into practice at the community level and with a modest use of resources [14]. Although carrying out such interventions in the private sector is challenging [15–17], the ADDO platform facilitated this activity. For example, we were able to use the TFDA’s supervisory structure to implement the intervention, and we used the existing ADDO registers to assess the appropriateness of treatment over time and triangulate that data with an assessment of dispenser knowledge and other data collection.
Overall, the availability of authorized antimicrobials increased, while availability of unauthorized antimicrobials decreased. The availability of the unauthorized medicines may contribute to inappropriate use because dispensers have not been trained on how to dispense them. Although it is possible that dispensers hid those medicines from the supervisors, knowing that they were not allowed, we assume that would have occurred during all the visits uniformly, rather than showing the steady decrease that was observed.
At baseline, few ADDOs had rubber stamps to help them label medicine packages appropriately. Although using a standardized stamp is not required, clear and comprehensive labeling is a requirement, and the stamp was very effective at improving the quality of medicine labels, with almost 100% including the important information on the labels.
In terms of the quality of dispensing, many more dispensers knew by endline which instructions they should give customers and how these instructions and how customers’ inappropriate use of medicines can contribute to AMR; for example, whereas none of the dispensers mentioned AMR as a consequence of poor antimicrobial use at baseline, they all mentioned it at endline. Our interviews with customers exiting the shops also showed that the dispensers had explained how to take dispensed medicines correctly. By the third visit, almost all (over 95%) of customers interviewed could correctly report the dose, dosage, and duration of treatment of the medicines they received from ADDOs. In addition, significantly fewer customers were being dispensed unneeded antimicrobials for simple diarrhea and acute respiratory infections—decreasing their out-of-pocket expenditures as well as reflecting appropriate practices.
In the workshop to present the study results, stakeholders recommended that the AMR job aids developed for counseling and labeling should be made mandatory tools in ADDOs and that the AMR concept should be incorporated into the ongoing ADDO training curriculum or into continuing education for dispensers. However, despite the encouraging results achieved by this AMR pilot, ADDO customers still ask for and clinicians prescribe antimicrobials for common illnesses such as diarrhea and upper respiratory tract infections. Because containing AMR requires a multifaceted effort, strengthening collaboration and partnerships with different stakeholders will help leverage resources for consumer awareness activities.
Conclusions
Critics of private sector health care have argued that providers are motivated more by profit than by public health; however, we found that ADDO dispensers are anxious to have the correct knowledge regarding medicine use and are proud to be seen as a community resource on health. Providing educational materials and messages and equipping drug dispensers with knowledge and tools help improve community medicine use and possibly help reduce AMR. Using dispensers and health facility staff to distribute AMR educational materials promoted community awareness about the existence and consequences of the AMR threat and how improper self-medication can contribute to the threat.
References
Brieger W, Unwin A, Greer G, Meek S: Interventions to Improve the Role of Medicine Sellers in Malaria Case Management for Children in Africa. 2005, London, UK and Arlington, Va., USA: the Malaria Consortium and BASICS for the United States Agency for International Development; prepared for Roll Back Malaria’s Sub-group for Communication and Training and Malaria Case Management Working Group
Tumwikirize WA, Ekwaru PJ, Mohammed K, Ogwal-Okeng JW, Aupont O: Management of acute respiratory infections in drug shops and private pharmacies in Uganda: a study of counter attendants' knowledge and reported behaviour. East Afr Med J. 2004, S33-S40.
Rational Pharmaceutical Management (RPM) Plus Program, Centre for Enhancement of Effective Malaria Interventions (CEEMI) and Basic Support for Institutionalizing Child Survival (BASICS): Improving child health through the accredited drug dispensing outlet program: baseline from five districts in Tanzania. 2006, Arlington, VA: BASICS and RPM Plus/MSH
Kojo-Arhinful D, Kusi A, Eghan K, Owunna C, Embrey M: Assessment of malaria pharmaceutical management systems in Ghana. 2010, Arlington, VA: Management Sciences for Health
Goodman C, Kachur SP, Abdulla S, Bloland P, Mills A: Drug shop regulation and malaria treatment in Tanzania: why do shops break the rules, and does it matter?. Health Policy Plan. 2007, 22 (6): 393-403. 10.1093/heapol/czm033.
Center for Pharmaceutical Management (CPM): 2003. Access to essential medicines: Tanzania: Prepared for the Strategies for Enhancing Access to Medicines Program. 2001, Arlington, VA: Management Sciences for Health
Tanzania Food, Drugs & Cosmetics (Standards and Code of Ethics for Duka la Dawa Muhimu) Regulations, 2004 and its amendment of 2009.
Rutta E, Senauer K, Johnson K, Adeya G, Mbwasi R, Liana J, Kimatta S, Sigonda M, Alphonce E: Creating a new class of pharmaceutical services provider for underserved areas: the Tanzania accredited drug dispensing outlet experience. Prog Community Health Partnersh. 2009, 3 (2): 145-153. 10.1353/cpr.0.0063.
Rutta E, Kibassa B, McKinnon B, Liana J, Mbwasi R, Mlaki W, Embrey M, Gabra M, Shekalaghe E, Kimatta K, Sillo H: Increasing access to subsidized artemisinin-based combination therapy through accredited drug dispensing outlets in Tanzania. Health Res Policy Syst. 2011, 9: 22-10.1186/1478-4505-9-22.
Tanzania Pharmacy Council: Personal communication. 2014
Radyowijati A, Haak H: Improving antibiotic use in low-income countries: an overview of evidence on determinants. Soc Sci Med. 2003, 57 (4): 733-744. 10.1016/S0277-9536(02)00422-7.
World Health Organization: Medicines Use in Primary Care in Developing and Transitional Countries: Fact Book Summarizing Results from Studies Reported Between 1990 and 2006. 2009, Geneva: WHO
National Board of Statistics: Population and Housing Census Brief Results. 2012, Dar es Salaam: Government of Tanzania, http://www.ngs.go.tz .
World Health Organization: WHO Global Strategy for Containment of Antimicrobial Resistance. WHO/CDS/CSR/DRS/2001.2. 2001, Geneva: WHO
Abuya T, Fegan G, Rowa Y, Karisa B, Ochola S, Mutemi W, Marsh V: Impact of ministry of health interventions on private medicine retailer knowledge and practices on anti-malarial treatment in Kenya. Am J Trop Med Hyg. 2009, 80: 905-913.
Ahmed SM, Hossain MA, Chowdhury MR: Informal sector providers in Bangladesh: how equipped are they to provide rational health care?. Health Policy Plan. 2009, 24 (6): 467-478. 10.1093/heapol/czp037.
Bloom G, Standing H, Lucas H, Bhuiya A, Oladepo O, Peters DH: Making health markets work better for poor people: the case of informal providers. Health Policy Plan. 2011, 26 (26.Suppl): 1:i4-52.
Acknowledgements
This work was funded by a cooperative agreement to Management Sciences for Health from the U.S. Agency for International Development (#GHN-A-00-07-00002-00). The opinions expressed herein are those of the authors and do not necessarily reflect the views of USAID.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
RV and JL participated in the design of the study, led the coordination of the study at the local level, made field visits to collect and analyze data, and provided inputs to the draft manuscript. MPJ conceived the study, participated in designing and coordinating the implementation of the study, led the design of the baseline survey questionnaire, and reviewed the manuscript. ER participated in the design and coordination of the study, analysis of the data, and review of the manuscript. ME participated in the analysis and interpretation of data and took a lead role in drafting and revising the manuscript. MB and BK participated in the coordination of the study, field visits for data collection, analysis of the data, and review of the manuscript. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article

Cite this article
Valimba, R., Liana, J., Joshi, M.P. et al. Engaging the private sector to improve antimicrobial use in the community: experience from accredited drug dispensing outlets in Tanzania. J of Pharm Policy and Pract 7, 11 (2014). https://doi.org/10.1186/2052-3211-7-11
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/2052-3211-7-11