
Abstract
The (pre)school environment is an important setting to improve children’s health. Especially, the (pre)school playground provides a major opportunity to intervene. This review presents an overview of the existing evidence on the value of both school and preschool playgrounds on children’s health in terms of physical activity, cognitive and social outcomes. In addition, we aimed to identify which playground characteristics are the strongest correlates of beneficial effects and for which subgroups of children effects are most distinct. In total, 13 experimental and 17 observational studies have been summarized of which 10 (77%) and 16 (94%) demonstrated moderate to high methodological quality, respectively. Nearly all experimental studies (n = 11) evaluated intervention effects on time spent in different levels of physical activity during recess. Research on the effects of (pre)school playgrounds on cognitive and social outcomes is scarce (n = 2). The experimental studies generated moderate evidence for an effect of the provision of play equipment, inconclusive evidence for an effect of the use of playground markings, allocating play space and for multi-component interventions, and no evidence for an effect of decreasing playground density, the promotion of physical activity by staff and increasing recess duration on children’s health. In line with this, observational studies showed positive associations between play equipment and children’s physical activity level. In contrast to experimental studies, significant associations were also found between children’s physical activity and a decreased playground density and increased recess duration. To confirm the findings of this review, researchers are advised to conduct more experimental studies with a randomized controlled design and to incorporate the assessment of implementation strategies and process evaluations to reveal which intervention strategies and playground characteristics are most effective.
Similar content being viewed by others


Introduction
During childhood and adolescence, regular physical activity is associated with improvements in both physiological and psychological health [1–4]. Despite the growing awareness of these benefits, children’s physical activity level seems to be declining [5, 6]. Several studies have shown that many children are currently insufficiently active and do not meet the health-related physical activity guideline of ‘180 minutes or more of physical activity at any intensity spread throughout the day’ for preschool children [7, 8] or the guideline of ‘60 minutes or more of at least moderate intensity activity each day’ for school-aged children [9]. Therefore, the promotion of regular physical activity in youth has become a public health priority.
Physical activity is influenced by many factors. Several reviews have summarized the evidence on correlates of children’s physical activity [10–15]. There is extensive literature on the demographic, biological, and psychosocial determinants of physical activity among youth [10, 13–15]. In the last decade, a growing interest in the role of the built environment on physical activity can be observed. Ferreira et al. [11] conducted a semi-quantitative review of 150 studies on environmental correlates of youth physical activity published between 1980 and 2004, and found that particularly the school environment is associated with children’s physical activity level. This was subscribed in a similar, but smaller review of Davison & Lawson [12]. School is known as a suitable setting for the promotion of physical activity in youth, since children can be reached with minimal effort and children spent most of their time there [16]. School-based opportunities to engage in physical activity are during physical education classes, during recess and after school hours [17, 18]. In contrast to physical education, which only provides 8% to 11% of children’s daily physical activity on a weekday [19, 20], recess offers the potential to gather up to 40% of the daily amount of moderate to vigorous physical activity (MVPA) [21, 22]. In 2006, Ridgers et al. summarized the effects of the first recess-based interventions and showed that energy expenditure and physical activity levels of children aged 4 to 12 years old increased shortly after the implementation of playground-based interventions at schools [22]. However, not all intervention strategies seem to be as effective [23–25]. According to Escalante et al. [25] who summarized five experimental studies, interventions based on playground markings, game equipment, or a combination of the two do not increase the physical activity level of children aged 4–11 years, but interventions based on playgrounds markings plus physical structures can be effective in the short to medium term. This is in contrast with Parrish et al. who summarized six experimental studies [24]. In their review, they state that playgrounds markings and games equipment significantly increase children’s physical activity level. Studies that examined combined strategies showed mixed findings. They conclude that although there are some promising recess-based interventions, there is no conclusive evidence for an effect of any type of recess-based intervention on the physical activity level of children aged 5–11 years. So far, none of the reviews have examined the effects of playground-based interventions on preschool children. Preschool children may also benefit from playgrounds [15]. In addition, none of the reviews have looked for evidence on the beneficial effects of playgrounds on outcomes other than physical activity.
Therefore, the aim of this review paper is to present an overview of the existing evidence on the value of (pre)school playgrounds for children’s health in terms of physical activity, cognitive and social outcomes. Further, we aimed to identify which playground characteristics are most effective, and for which subgroups of children effects are most distinct. In contrast to previous reviews on this topic [22–25], both observational and experimental studies focusing on preschool children as well as older age groups will be included, allowing for comparison of the results.
Methods
Search strategy and data sources
Studies published from January 2000 to September 2012 were identified through a structured computerized search of PubMed, PsycINFO, and EMBASE. The search terms are shown per database in Additional file 1. According to the search terms, only studies conducted in children from 2 to 18 years old were selected. In addition to these terms, related and most recent thesaurus terms of the search engines were added. No limitations for study design were added. Based on the title, search results were checked for relevance and duplicates.
Selection of studies
Based on the title and the abstract, further study selection was performed by two independent researchers (KB and AMS). Studies had to examine the association between a (pre)school playground and physical, cognitive or social outcomes. (Pre)school playgrounds were defined as spaces located on (pre)school properties that were specifically designed for outdoor play and sports activities for children from 2 to 18 years old. Studies on other playgrounds, e.g., amusement parks or recreation areas that were not school-based were not included. Further, studies were included if published in a peer reviewed scientific journal and published in English. In addition, grey literature from January 2000 to September 2012 was identified through the Educational Resources Information Centre (ERIC) and the Dutch database ‘Grey Literature in the Netherlands’ (GLIN) using the search terms ‘schoolyard’ and ‘playground’. Grey literature formed a contextual background for the interpretation of the topic and results. Data from grey literature was not further extracted.
Data extraction
Based on the full-texts of the studies, the data of each study was extracted by two independent researchers (KB and AMS or KB and SdV). In case of disagreement, this was discussed until consensus was reached. The following study characteristics were extracted: design of the study, level of randomization, aim of the study, size and source of the study sample, country in which the study was performed, age range and/or mean age of the sample, socio-economic status of the sample, type of playground and characteristics, type of outcomes, measurement instruments of playgrounds and outcomes, and effects per outcome. If available, additional results per subgroup (e.g., according to sex) were extracted.
Methodological quality
Methodological quality was assessed by two independent researchers (KB and AMS or KB and SdV), based on the full-texts of the studies. Two scoring lists were developed for observational and experimental studies respectively. Items were derived from scoring lists of Prins et al. [26] and De Vries et al. [27]. The scoring list for observational studies contained 11 items: five items that indicated internal validity (reported validity and reliability of measurement instruments of the playground, reported validity and reliability of the outcomes, and report of statistical analytical procedure) and six items that indicated external validity (representativeness of the study sample, specification of the age range of the study sample, specification of in- and exclusion criteria, response rate or specification of non-response, specification of the study period, and specification of the sample characteristics).
The scoring list for experimental studies contained 14 items: nine items identical to those scored for observational studies, except for the reported validity and reliability of measurement instruments of the playground. Five items were specific for experimental studies, i.e., presence of a control group, randomization, blinding of study participants and interventionists, blinding of outcome assessors, and completeness of outcome data.
Each item was scored with ‘present’ (1), ‘partly present’ (0.5), or ‘absent’ (0), in accordance with De Vries et al. [27]. A total score was computed per publication by summing all unweighted scores. Each publication was then assigned a methodological quality rating. For experimental studies, methodological quality was high if 10 points or more were assigned, indicating that 72% of the quality criteria were met. The methodological quality of experimental studies was moderate if 7.0 – 9.5 points were assigned and low if 6.5 or less points were assigned. For observational studies, methodological quality was high if 8.5 points or more were assigned, indicating that 77% of the quality criteria were met. The methodological quality of observational studies was moderate if 5.5 – 8.0 points were assigned and low if 5.0 or less points were assigned. In case of disagreement between the two independent researchers, this was discussed until consensus was reached.
Data synthesis
Level of evidence for playground-based intervention strategies
In order to summarize the level of evidence of the findings from experimental studies, intervention strategies used in the experimental studies were labelled with a level of evidence, ranging from strong, moderate, limited, inconclusive to no evidence. This rating system was used in previous reviews of Van Sluijs et al. [16] and Parrish et al. [24] and takes into account: study design, sample size, methodological quality, and the intervention effect. The decision-making process underlying the rating system is available as a supplementary file by Van Sluijs and colleagues [16]. In short, intervention strategies were labelled with strong, moderate or limited level of evidence if at least two-third of the studies found significant positive results. In order to be labelled as a large study, more than 250 participants were required.
Associations of playground characteristics with physical activity
The results of the observational studies were summarized in a slightly different manner. For each playground characteristic a summary code was determined taking into account the outcome, the methodological quality of the studies, and the total number of studies that examined the playground characteristic. Playground characteristics were categorized as either hardware (i.e., permanent playground conditions, such as playground size, and surface type), software (i.e., the provided equipment and activities on playgrounds, such as fixed and portable play equipment), or orgware (i.e., the organization beyond playgrounds, such as the presence of supervision and the recess duration). First, all outcomes were weighted for the quality of the study as previously done by De Vries et al. [27]. Observational studies of poor quality (≤5.0 points) provide less evidence for the reported associations than studies of high quality (≥8.5 points). Next, the number of studies that found significant positive or negative associations between the playground characteristic and physical activity was divided by the total number of studies that examined that characteristic. This resulted in a percentage of studies that supported a significant positive or negative association with physical activity. This percentage was classified as no association (0), indeterminate/inconclusive association (?), positive (+) or negative association (−) using the model of Sallis [13]. When 0%-33% of the studies supported a positive or negative association, the result was classified as no association (0). An indeterminate/ inconclusive (?) classification was determined if 34%-59% of the studies supported an association. A positive (+) or negative (−) association was determined when 60%-100% of the studies supported the direction of the association. When the quality of the underlying studies was moderate or high one or two additional characters (− or +) were assigned to the summary code, respectively. In addition, if a playground characteristic was investigated four or more times an additional + or – was also assigned [13].
Results
Selection of studies
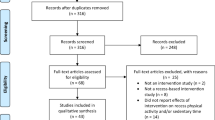
The initial cross-database search in PubMed, PsycINFO, and EMBASE resulted in 1073 publications. After eliminating duplicates, 931 publications remained. Titles and abstracts were reviewed for eligibility criteria, resulting in 35 publications that were fully considered. Based on the full-texts, 26 of them were included in the review. A backward search of the reference lists of these publications yielded another seven publications. Thus, 33 publications were finally included. A flowchart of the selection procedure is depicted in Figure 1.

Flowchart describing the number of articles retrieved, and included and excluded at each stage of the review process.
Study characteristics
Of the 33 included publications, 16 reported on experimental studies and 17 on observational studies. Their study characteristics are summarized in Table 1 and Table 2, respectively.
Experimental studies
The 16 publications reporting on experimental studies were based on 13 studies, since some publications were based on the same study sample. This was true for three publications of Ridgers and colleagues, in which the effects of incentives to change playgrounds on physical activity during recess were reported for different follow-up periods, i.e., six weeks, six months, and 12 months [28–30]. Further, Stratton and colleagues reported twice on the effects of painting markings on playgrounds of two early primary schools; once in 2000 and once again in a more recent publication in 2005. In the most recent publication, the sample size had increased through the inclusion of two additional late primary schools [31, 32].
Seven of the 13 experimental studies (54%) included a control group in the study design, and only three of them used a randomization procedure to allocate schools and/or children to an intervention or control condition [33–35]. Six of the 13 experimental studies were conducted in the United States [36–41]. The remaining seven studies were conducted in Belgium [33, 35, 42], United Kingdom [28–32], Cyprus [34], and Australia [43]. All study samples contained approximately 50 percent girls. Sample sizes ranged from one to 40 schools and from five to 5488 children. Five studies specifically targeted preschools with children from three to six years old [33, 36–38, 42], whereas eight studies described the effects of playground interventions on primary schools, with children aged four to 11 years old [28–32, 34, 35, 39–41, 43].
In preschools, the five interventions included the provision of play equipment [33, 36], the promotion of physical activity on playgrounds by teachers [37], variations in recess duration [38], and variations in playground density (m2/child) [42]. Two of the five experimental studies included a control group, i.e., Cardon et al. [33] and Brown et al. [37]. Cardon and colleagues [33] compared the effects of two intervention conditions (i.e., the provision of play equipment only and the provision of play equipment and painting of playground markings) with a no-intervention condition. Brown et al. [37] also tested two intervention conditions (i.e., the promotion of physical activity by teachers against the addition of group discussions and the provision of stickers when children showed sufficient physical activity) against a no-intervention condition.
In primary schools, all eight interventions included the provision of play equipment and/or the application of playground markings. Six of the eight experimental studies in primary schools included a no-intervention condition [28–32, 34, 35, 40, 44]. One study examined the isolated effect of playground markings with a no-intervention condition [31, 32]. Similarly, Bundy et al. [43] evaluated the effect of the provision of play materials, only without a control condition. In the other studies the interventions contained multiple components. Of these six studies, Hyberty et al. [39] was the only study without a control condition. Interventions in two studies contained both the provision of play equipment and the application of playground markings, complemented with the creation of space for team games, and staff training respectively [34, 39]. Ridgers et al. [28–30], Colabianchi et al. [40], and Brink et al. [41] combined the provision of play equipment and playground markings with playground improvements. Verstraete and colleagues provided both play equipment and activity cards which informed children on the activities that could be performed with different pieces of play equipment [35].
As is shown in Table 1, nearly all experimental studies (n = 11) evaluated intervention effects on time spent in different levels of physical activity during recess. The proportion of time spent in light, moderate and vigorous physical activity and sedentary activity was mostly assessed with the use of accelerometers, with the exception of three studies in which physical activity was assessed by observations [37, 40, 41], one study that used pedometers [34], and one study that used heart rate telemetry [31, 32]. Other observed outcomes were playfulness [43] and post-recess attention [38]. Intervention effects were assessed mostly directly during recess. In case of the provision of playground markings and structural playground improvements, outcomes were assessed with follow-up periods ranging from one month to 12 months.
Observational studies
Of the 33 included publications, 17 reported on observational studies. Their study characteristics are summarized in Table 2. Five of the 17 observational studies were conducted in the United States [44–48] and the remaining studies were conducted in the United Kingdom [49, 50], Australia [51, 52], Norway [53, 54], New Zealand [55, 56], Belgium [57], Sweden [58], Denmark [59], and the Netherlands [60]. Forty-three to 61 percent of the study samples were girls, and sample sizes ranged from seven to 130 schools and from 128 to 36.955 children. Five studies specifically reported on associations in preschools (age range: 2.6 to six years old), nine studies in primary schools (age range: five to 12 years old), and three in other types of schools, such as in secondary schools, middle schools or mixed schools (age range: eight to 15 years old). The study of Nielsen et al. [59] was exceptive, as in this study the association of playground characteristics with physical activity was examined at two time points: at preschool, and at primary school.
Many different playground characteristics were examined and categorized as either hardware, software, or orgware. With regard to software, some studies made a distinction between fixed and loose equipment [45, 49, 51, 60]. Playground characteristics were assessed through self-reports [53, 55] or observations [44–52, 54, 56–60], mostly with the use of validated instruments, such as the Environmental Assessment of Public Recreation Spaces Tool (EAPRS), Children Activity Scanning Tool (CAST), and Environment and Policy Assessment and Observation instrument (EPAO) [46, 52, 60]. In accordance with the experimental studies, the outcomes reported in observational studies were mainly in terms of time spent in different levels of physical activity during recess. Physical activity was mostly assessed through observational instruments [44, 46–49, 51, 52, 60], four studies used an accelerometer [45, 50, 56, 59], three studies used a self-report instrument [53–55], and two studies used a pedometer [57, 58]. In addition to physical activity, Colabianchi et al. [46] also assessed the utilization of the playground through observations.
Methodological quality
The methodological quality scores of the experimental studies ranged from 4.5 to 10 points on a 14-point scale. Two of the 13 studies (15%) demonstrated high methodological quality [33, 41], eight studies (62%) were of moderate quality [28–32, 34–36, 39, 40, 43], and three studies (23%) were of low quality [37, 38, 42]. None of the experimental studies reported on the use of blinding of study participants, personnel who implemented the intervention or outcome assessors. A summary of the methodological quality analysis per study can be found in Additional file 2. The methodological quality of the observational studies ranged from 5.0 to 9.5 points on an 11-point scale. Seven of the 17 observational studies (41%) demonstrated high methodological quality [46, 50, 52, 53, 55, 58, 60], nine studies (53%) were of moderate quality [30, 37, 44, 48, 51, 54, 56, 57],[59], and one study (6%) was of low quality [45]. Information on the reliability and validity of instruments for the measurement of playground characteristics was reported by only one and five studies respectively. Detailed information on the quality scores of the observational studies can be found in Additional file 2.
Study outcomes
Experimental studies
Although it was our intention to summarize the effects of (pre)school playgrounds on children’s health in terms of physical activity, cognitive, and social outcomes, nearly all experimental studies (n = 11) focused on physical activity as the primary outcome. Only one study examined the effect a playground-based intervention on cognitive outcomes (i.e., post-recess attention, Holmes et al. [38]) and social outcomes (i.e., playfulness, Bundy et al. [43]).
In preschools, the effect of decreased playground density was investigated by one study that showed a significant increase of physical activity levels (see Tables 1 and 3) [42]. The provision of play equipment showed mixed effects on physical activity levels of preschool children [33, 36]. No effects were found in the two studies that investigated the provision of playground markings and promotion of physical activity by teachers [33, 37]. Increase of recess duration was investigated by one single study that showed positive effects on post-recess attention of preschool children [38]. Further, two studies investigated the effects of a multi-component intervention, including a combination of promotion of physical activity by teachers and guided discussions in one study, and the provision of play equipment and playground markings in another study [33, 37]. Both studies showed no beneficial effects on preschool children. In summary, taking into account the study design, the sample size and the methodological quality of the experimental studies, there is inconclusive evidence for an effect of the provision of play equipment, playground markings or for multi-component interventions at preschools on children’s health (Table 3). No evidence was generated for the other intervention strategies at preschools.
In primary schools, the two interventions that targeted the provision of play equipment were effective with regard to physical activity levels during recess and playfulness (see Tables 1 and 3) [35, 43]. The two studies that investigated the effects of the provision of playground markings found mixed effects [31, 32]. Allocating play space for team games was investigated by one study that found a significant beneficial effect [34]. Seven studies investigated multi-component playground interventions, of which the majority showed beneficial effects on physical activity levels [29, 34, 39, 41]. Multi-component interventions that showed beneficial effects contained combinations of staff training, play equipment and playground markings [39], the allocation of play space, play equipment and playground markings [34], the provision of playground markings and physical structures [28–30] and the installation of play equipment and asphalt areas [41] respectively. When summarizing the effects into levels of evidence, one can conclude from Table 3 that there is inconclusive evidence for an effect of the provision of play equipment, playground markings and allocating play space in primary schools on children’s physical activity level. Moderate evidence is found for an effect of the use of multi-component intervention strategies. For the remaining separate intervention strategies no evidence is found.
When the evidence for different playground-based intervention strategies is summarized regardless of school type (preschool or primary school), studies generate moderate evidence for an effect of the provision of play equipment, inconclusive evidence for an effect of the use of playground markings, allocating play space or multi-component interventions, and no evidence for an effect of decreasing playground density, the promotion of physical activity by staff and increasing recess duration on children’s health in terms of physical activity, cognitive, and social outcomes.
Subgroups
With regard to subgroups in which playground interventions are most effective, four experimental studies found stronger effects on the physical activity level and on post-recess attention of girls compared to boys. These interventions entailed the decrease of playground density [42], the presentation and provision of game equipment and activity cards [35], and variations in recess duration [38]. Brink et al. [41] indicated that girls were more active on soft structured surfaces (with play equipment, fall zones and play fields with grass), in contrast to boys who were more active on hard unstructured surfaces (unprogrammed creative play, educational marking areas, sitting and social gathering areas, shade areas). Subgroup analyses in observational studies indicated a more pronounced association between less supervising teachers and physical activity levels in girls [57]. In boys, associations of physical activity levels with the presence of hopscotch and skipping rope areas [53], decreased playground density [57], and the presence of soccer fields [53] were more prominent.
Observational studies
In Table 4 the associations with physical activity are summarized per type of playground characteristic: hardware, software, and orgware. In preschools, summary codes of association indicate that there is evidence for a positive association between physical activity and playground size (++), the presence of an open field with no markings (++), a structured track (+++), decreased playground density (++), and increased recess duration (++). Negative associations were found for the presence of slides (- - -), a sandbox (- - -), swinging equipment (- - -), and supervision (−−).
In primary, secondary or mixed schools, summary codes of association indicate no associations of hardware playground characteristics with physical activity. Of the software characteristics, the provision of play equipment (++), balls (+++), portable (++) and fixed equipment (+++), and hopscotch/skipping rope area (+++) were positively associated with physical levels. With regard to the orgware playground characteristics, no organized activities (++) and decreased playground density (++) were positively associated with recess activities. Negative associations were found with physical activity for trash cans (- - -) and water and swimming facilities (- -).
When the associations between playground characteristics and physical activity are summarized regardless of school type (preschool or primary, secondary, or mixed school), there is no longer an association between hardware playground characteristics and children’s physical activity level. Decreased playground density and no organized activities are positively associated with children’s physical activity, as well as the provision of portable and fixed play equipment (including balls), the presence of a hopscotch/skipping rope area, an open field with no markings, and a structured track.
Discussion
Overall, this review found moderate evidence for an effect of the provision of playground equipment on physical activity levels of children at preschools and primary, secondary or mixed schools. There was inconclusive evidence for an effect of the allocation of playground markings and more play space and for multi-component interventions on children’s health in terms of physical activity, cognitive and social outcomes. These results are in accordance with previous reviews that also showed no conclusive evidence of playground interventions at primary schools [22, 24, 25]. Evidence for playground intervention effects was only slightly different for primary schools and preschools. At primary schools, there was moderate evidence for an effect of the use of multi-component interventions on children’s physical activity level, in contrast to inconclusive evidence at preschools. For the other intervention strategies no (conclusive) evidence was found nor in primary schools nor in preschools.
Boys versus girls
Four of the 13 experimental studies performed subgroup analyses and found stronger effects on the physical activity level and on post-recess attention of girls compared to boys. According to Verstraete et al. [35] this might be explained by the fact that boys are already very active at baseline level, making it difficult to find significant improvements due to an intervention. The fact that girls more often engage in social talk on playgrounds and choose sedentary play activities and games also make them more susceptible for improvements [49]. Lastly, it is known that boys often engage in ball games. Decreasing playground density, as performed in the study of Van Cauwenberghe et al. [42] may allow girls to increasingly engage in their own type of games/physical activities, without being dominated by e.g., boys or supervisors. Since the main reasons for the difference in playground physical activity levels between girls and boys are not yet known, future studies on this topic should contain subgroup analyses according to sex in their design.
Additional findings from the observational studies
Next to 13 experimental studies, 17 observational studies have been summarized in our review. The observational studies indicate that among preschoolers, mainly hardware and orgware playground characteristics (i.e., increased playground size, decreased playground density, and increased recess duration) are associated with an increase in physical activity level during recess. However, among children on primary, secondary or mixed schools, software characteristics (i.e., play equipment) are mainly positively associated with increased physical activity levels. It seems that for preschool children, having sufficient space to play and having optimal playground conditions (open field, no supervision, longer recess duration) may be sufficient to be physically active.
Observational studies versus experimental studies
Although randomized controlled trials remain a prominent study design in clinical research, they depend on plausibility and adequacy arguments from observational studies to make hypotheses about causal relationships credible [61, 62]. Overall, results from observational studies in our review indicate that particularly hardware and orgware playground characteristics (i.e. playground size, decreased playground density and increased recess duration) are associated with children’s physical activity levels at preschools. However, experimental studies found no evidence for this, mainly due to the small amount of studies that investigated the effects of these strategies. Second, observational studies also show that the provision of play equipment is associated with children’s physical activity levels, particularly in primary, secondary or mixed schools. Unfortunately, experimental studies were not able to generate conclusive evidence for the provision of play equipment at primary, secondary or mixed schools. However, regardless of school type, we found moderate evidence for the use of play equipment. Aiming for observational and experimental studies to be complementary, fellow researchers are advised to take results from observational studies into account when designing an experimental study and vice versa.
Limitations and recommendations
Based on study design, sample size, methodological quality and intervention effect, nearly all intervention strategies did not reach moderate or strong levels of evidence. At first sight, when looking at the percentage of studies that found positive effects, some playground interventions seemed to have significant beneficial effects in this review. However, because of a lack of large randomized controlled trials with high methodological quality in this review, levels of evidence did not reach moderate or strong levels. We realize that the application of a randomized study design in experimental studies is hampered by the nature of environmental interventions, and by the context of the study. For example, some interventions were based on governmental funding aiming to improve environmental facilities of deprived schools, and for this reason no randomization procedure could be carried out. However, we strongly advise researchers to conduct more large RCTs investigating environmental interventions, in order to draw conclusions that are more valid. The effects of the improvement of e.g., organizational factors in (pre)school playgrounds could be investigated by allocating a number of preschools to either an intervention or a control condition.
A second limitation is that the outcomes of this review do mainly account for physical activity and can therefore not be generalized to other types of outcomes. Investigation of the association of (pre)school playgrounds with cognitive, and social economic outcomes is highly relevant, and researchers are urgently invited to focus on these outcomes in future observational and experimental studies. With regard to generalizability, the results of this review are mainly limited to studies performed in preschools or primary schools. Only two studies explored associations of playground characteristics with physical activity during recess at secondary schools. Since many adolescents fail to achieve the requirements for sufficient physical activity [63], it is recommended to examine the value of playgrounds for this age group as well. Another limitation that should be kept in mind is the variability in the type of school playgrounds examined in this review. Although the majority of the studies were conducted in the United States or United Kingdom, playgrounds differ in e.g., their size, shape, vegetation, and climate, depending on their geographical location. These differences might have influenced the effects and associations found in the studies included in the review.
Conclusion
Overall, findings demonstrate inconclusive evidence for positive effects of playground interventions in a (pre)school setting on children’s physical activity levels. Looking at the evidence on the value of different playground-based intervention strategies, moderate evidence was generated for an effect of the provision of play equipment at all school types, and for an effect of multi-component interventions, including the provision of playground markings, play equipment and/or play space on the physical activity level of children at primary schools. No evidence was found for other health effects of playground-based interventions in terms of cognitive and social outcomes. For preschool children, having sufficient time and space to play seems to be sufficient to be physically active. In primary, secondary or mixed schools on the other hand, the presence of fixed play equipment appears to be a predictor of children’s physical activity level during recess. In order to strengthen the findings of this review, researchers are advised to conduct more high quality experimental studies with a large sample size and randomized controlled design. Further, future research should examine the effect of playground-based interventions on other outcomes than physical activity. In addition, future research should also focused on additional assessment of implementation strategies and process evaluations to reveal which intervention strategies and playground characteristics are most effective.
References
Andersen LB, Riddoch C, Kriemler S, Hills A: Physical activity and cardiovascular risk factors in children. Br J Sports Med. 2011, 45: 871-876. 10.1136/bjsports-2011-090333.
Biddle SJH, Asare M: Physical activity and mental health in children and adolescents: a review of reviews. Br J Sports Med. 2011, 45: 886-895. 10.1136/bjsports-2011-090185.
Strong WB, Malina RM, Blimkie CJ, Daniels SR, Dishman RK, Gutin B, Hergenroeder AC, Must A, Nixon PA, Pivarnik JM, Rowland T, Trost S, Trudeau F: Evidence based physical activity for school-age youth. J Pediatr. 2005, 146: 732-737. 10.1016/j.jpeds.2005.01.055.
Timmons BW, Leblanc AG, Carson V, Connor Gorber S, Dillman C, Janssen I, Kho ME, Spence JC, Stearns JA, Tremblay MS: Systematic review of physical activity and health in the early years (aged 0–4 years). Appl Physiol Nutr Metab. 2012, 37 (4): 773-792. 10.1139/h2012-070.
Dollman J, Norton K, Norton L: Evidence for secular trends in children’s physical activity behaviour. Br J Sports Med. 2005, 39: 892-897. 10.1136/bjsm.2004.016675.
McDonald NC, Austin L, Brown MRP, Marchetti LM, Pedroso MS, U.S. School Travel, 2009: An assessment of trends. Am J Prev Med. 2011, 41 (2): 146-10.1016/j.amepre.2011.04.006.
Pate RR, O’Neill JR: Physical activity guidelines for young children: an emerging consensus. Arch Pediatr Adolesc Med. 2012, 166 (12): 1095-1096. 10.1001/archpediatrics.2012.1458.
Tremblay MS, Leblanc AG, Carson V, Choquette L, Connor Gorber S, Dillman C, Duggan M, Gordon MJ, Hicks A, Janssen I, Kho ME, Latimer-Cheung AE, Leblanc C, Murumets K, Okely AD, Reilly JJ, Spence JC, Stearns JA, Timmons BW: Canadian society for exercise physiology: canadian physical activity guidelines for the early years (aged 0–4 years). Appl Physiol Nutr Metab. 2012, 37 (2): 345-369. 10.1139/h2012-018.
Ekelund U, Tomkinson G, Armstrong N: What proportion of youth are physically active? Measurement issues, levels and recent time trends. Br J Sports Med. 2011, 45: 859-865. 10.1136/bjsports-2011-090190.
Van der Horst K, Chin A, Paw MJ, Twisk JWR, van Mechelen W: A brief review on correlates of physical activity and sedentariness in youth. Med Sci Sports Exerc. 2007, 39 (8): 1241-1250. 10.1249/mss.0b013e318059bf35.
Ferreira I, van der Horst K, Wendel-Vos W, Kremers S, van Lenthe FJ, Brug J: Environmental correlates of physical activity in youth – a review and update. Obes Rev. 2006, 8: 129-154.
Davison KK, Lawson CT: Do attributes in the physical environment influence children's physical activity? a review of the literature. Int J Behav Nutr Phys Act. 2006, 27 (3): 19.
Sallis JF, Prochaska JJ, Taylor WC: A review of correlates of physical activity of children and adolescents. Med Sci Sports Exerc. 2000, 32: 963-975.
Stanley RM, Ridley K, Dollman J: Correlates of children’s time-specific physical activity: a review of the literature. Int J Behav Nutr Phys Act. 2012, 30 (9): 50.
Hinkley BA, Crawford D, Salmon J, Okely AD, Hesketh K: Preschool children and physical activity: a review of correlates. Am J Prev Med. 2008, 34 (5): 435-441. 10.1016/j.amepre.2008.02.001.
Van Sluijs EM, McMinn AM, Griffin SJ: Effectiveness of interventions to promote physical activity in children and adolescents: systematic review of controlled trials. Br J Sports Med. 2008, 42 (8): 653-657.
Jago R, Baranowski T: Non-curricular approaches for increasing physical activity in youth: a review. Prev Med. 2004, 39: 157-163. 10.1016/j.ypmed.2004.01.014.
Wechsler H, Devereaux RS, Davis M, Collins J: Using the school environment to promote physical activity and healthy eating. Prev Med. 2000, 31 (2): 121S-137S. 10.1006/pmed.2000.0649.
Tudor-Locke C, Lee SM, Morgan CF, Beighle A, Pangrazi RP: Children’s pedometer-determined physical activity during the segmented school day. Med Sci Sports Exerc. 2006, 38 (10): 1732-1738. 10.1249/01.mss.0000230212.55119.98.
Slingerland M, Borghouts LB, Hesselink MK: Physical activity energy expenditure in Dutch adolescents: contribution of active transport to school, physical education, and leisure time activities. J Sch Health. 2012, 82 (5): 225-232. 10.1111/j.1746-1561.2012.00691.x.
Dessing D, Pierik FH, Sterkenburg RP, Van Dommelen P, Maas J, De VSI: Schoolyard physical activity of 6–11 year old children assessed by GPS and accelerometry. Int J Behav Nutr Phys Act. 2013, 10: 97-10.1186/1479-5868-10-97.
Ridgers ND, Stratton G, Fairclough SJ: Physical activity levels of children during school playtime. Sports Med. 2006, 36 (4): 359-371. 10.2165/00007256-200636040-00005.
Ridgers ND, Salmon J, Parrish AM, Stanley RM, Okely AD: Physical activity during school recess: a systematic review. Am J Prev Med. 2012, 43 (3): 320-328. 10.1016/j.amepre.2012.05.019.
Parrish AM, Okely AD, Stanley RM, Ridgers ND: The effect of school recess interventions on physical activity: a systematic review. Sports Med. 2013, 43 (4): 287-299. 10.1007/s40279-013-0024-2.
Escalante Y, García-Hermoso A, Backx K, Saavedra JM: Playground designs to increase physical activity levels during school recess: a systematic review. Health Educ Behav. 2014, 41 (2): 138-144. 10.1177/1090198113490725.
Prins J, Blanker MH, Bohnen AM, Thomas S, Bosch JL: Prevalence of erectile dysfunction: a systematic review of population-based studies. Int J Impot Res. 2002, 14 (6): 422-10.1038/sj.ijir.3900905.
De Vries SI, Bakker I, Hopman-Rock M, Hirasing RA, Van Mechelen W: Clinimetric review of motion sensors in children and adolescents. J Clin Epidemiol. 2006, 59: 670-680. 10.1016/j.jclinepi.2005.11.020.
Ridgers N, Stratton G, Fairclough S, Twisk J: Children’s physical activity levels during school recess: a quasi-experimental intervention study. Int J Behav Nutr Phys Act. 2007, 4 (1): 19-10.1186/1479-5868-4-19.
Ridgers ND, Stratton G, Fairclough SJ, Twisk JW: Long-term effects of a playground markings and physical structures on children’s recess physical activity levels. Prev Med. 2007, 44 (5): 393-397. 10.1016/j.ypmed.2007.01.009.
Ridgers ND, Fairclough SJ, Stratton G: Twelve-month effects of a playground intervention on children’s morning and lunchtime recess physical activity levels. J Phys Activ Health. 2010, 7 (2): 167-175.
Stratton G: Promoting children’s physical activity in primary school: an intervention study using playground markings. Ergonomics. 2000, 43 (10): 1538-1546. 10.1080/001401300750003961.
Stratton G, Mullan E: The effect of multicolor playground markings on children’s physical activity level during recess. Prev Med. 2005, 41: 828-833. 10.1016/j.ypmed.2005.07.009.
Cardon G, Labarque V, Smits D, Bourdeaudhuij ID: Promoting physical activity at the pre-school playground: the effects of providing markings and play equipment. Prev Med. 2009, 48 (4): 335-340. 10.1016/j.ypmed.2009.02.013.
Loucaides CA, Jago R, Charalambous I: Promoting physical activity during school break times: piloting a simple, low cost intervention. Prev Med. 2009, 48 (4): 332-334. 10.1016/j.ypmed.2009.02.005.
Verstraete SJ, Cardon GM, De Clercq DL, De Bourdeaudhuij IM: Increasing children’s physical activity levels during recess periods in elementary schools: the effects of providing game equipment. The Eu J Public Health. 2006, 16 (4): 415-419. 10.1093/eurpub/ckl008.
Hannon JC, Brown BB: Increasing preschoolers’ physical activity intensities: an activity-friendly preschool playground intervention. Prev Med. 2008, 46 (6): 532-536. 10.1016/j.ypmed.2008.01.006.
Brown WH, Googe HS, McIver KL, Rathel JM: Effects of teacher-encouraged physical activity on preschool playgrounds. J Early Intervent. 2009, 31 (2): 126-145. 10.1177/1053815109331858.
Holmes RM, Pellegrini AD, Schmidt SL: The effects of different recess timing regimens on preschoolers’ classroom attention. Early Child Dev and Care. 2006, 176 (7): 735-743. 10.1080/03004430500207179.
Huberty JL, Siahpush M, Beighle A, Fuhrmeister E, Silva P, Welk G: Ready for recess: a pilot study to increase physical activity in elementary school children. J Sch Health. 2011, 81 (5): 251-257. 10.1111/j.1746-1561.2011.00591.x.
Colabianchi N, Kinsella AE, Coulton CJ, Moore SM: Utilization and physical activity levels at renovated and unrenovated school playgrounds. Prev Med. 2009, 48 (2): 140-143. 10.1016/j.ypmed.2008.11.005.
Brink LA, Nigg CR, Lampe SM, Kingston BA, Mootz AL, van Vliet W: Influence of schoolyard renovations on children’s physical activity: the learning landscapes program. Am J Public Health. 2010, 100 (9): 1672-1678. 10.2105/AJPH.2009.178939.
Van Cauwenberghe E, De Bourdeaudhuij I, Maes L, Cardon G: Efficacy and feasibility of lowering playground density to promote physical activity and to discourage sedentary time during recess at preschool: a pilot study. Prev Med. 2012, 55 (4): 319-321. 10.1016/j.ypmed.2012.07.014.
Bundy AC, Luckett T, Naughton GA, Tranter PJ, Wyver SR, Ragen J, Singleton E, Spies G: Playful interaction: occupational therapy for all children on the school playground. Am J Occup Ther. 2008, 62 (5): 522-527. 10.5014/ajot.62.5.522.
Sallis JF, Conway TL, Prochaska JJ, McKenzie TL, Marshall SJ, Brown M: The association of school environments with youth physical activity. Am J Public Health. 2001, 91 (4): 618.
Dowda M, Brown WH, McIver KL, Pfeiffer KA, O’Neill JR, Addy CL, Pate RR: Policies and characteristics of the preschool environment and physical activity of young children. Pediatrics. 2009, 123: e261-e266. 10.1542/peds.2008-2498.
Colabianchi N, Maslow A, Swayampakala K: Features and amenities of school playgrounds: a direct observation study of utilization and physical activity levels outside of school time. Int J Behav Nutr Phys Act. 2011, 8 (1): 32-10.1186/1479-5868-8-32.
Brown WH, Pfeiffer KA, McIver KL, Dowda M, Addy CL, Pate RR: Social and environmental factors associated with preschoolers’ nonsedentary physical activity. Child Dev. 2009, 80 (1): 45-58. 10.1111/j.1467-8624.2008.01245.x.
McKenzie TL, Crespo NC, Baquero B, Elder JP: Leisure time physical activity in elementary schools: analysis of contextual conditions. J Sch Health. 2010, 80 (10): 470-477. 10.1111/j.1746-1561.2010.00530.x.
Ridgers ND, Fairclough SJ, Stratton G: Variables associated with children’s physical activity levels during recess: the A-CLASS project. Int J Behav Nutr Phys Act. 2010, 7 (1): 74-10.1186/1479-5868-7-74.
Fairclough SJ, Ridgers ND, Welk G: Correlates of children’s moderate and vigorous physical activity during weekdays and weekends. J Phys Act Health. 2012, 9 (1): 129.
Willenberg LJ, Ashbolt R, Holland D, Gibbs L, MacDougall C, Garrard J, Green JB, Waters E: Increasing school playground physical activity: a mixed methods study combining environmental measures and children’s perspectives. J Sci Med Sport. 2010, 13 (2): 210-216. 10.1016/j.jsams.2009.02.011.
Zask A, Van Beurden E, Barnett LM, Brooks LO, Dietrich UC: Active school playgrounds-myth or reality? Results of the ‘Move It Groove It’ project. Prev Med. 2001, 33 (5): 402-408. 10.1006/pmed.2001.0905.
Haug E, Torsheim T, Sallis JF, Samdal O: The characteristics of the outdoor school environment associated with physical activity. Health Educ Res. 2010, 25 (2): 248-256. 10.1093/her/cyn050.
Haug E, Torsheim T, Samdal O: Physical environmental characteristics and individual interests as correlates of physical activity in Norwegian secondary schools: the health behaviour in school-aged children study. Int J Behav Nutr Phys Act. 2008, 5: 47-10.1186/1479-5868-5-47.
Nielsen G, Taylor R, Williams S, Mann J: Permanent play facilities in school playgrounds as a determinant of children’s activity. J Phyl Act Health. 2010, 7 (4): 490.
Taylor RW, Farmer VL, Cameron SL, Meredith-Jones K, Williams SM, Mann JI: School playgrounds and physical activity policies as predictors of school and home time activity. Int J Behav Nutr Phys Act. 2011, 8 (1): 38-10.1186/1479-5868-8-38.
Cardon G, Van Cauwenberghe E, Labarque V, Haerens L, De Bourdeaudhuij I: The contribution of preschool playground factors in explaining children’s physical activity during recess. Int J Behav Nutr Phys Act. 2008, 5 (1): 11-10.1186/1479-5868-5-11.
Boldemann C, Blennow M, Dal H, Mårtensson F, Raustorp A, Yuen K, Wester U: Impact of preschool environment upon children’s physical activity and sun exposure. Prev Med. 2006, 42 (4): 301-308. 10.1016/j.ypmed.2005.12.006.
Nielsen G, Bugge A, Hermansen B, Svensson J, Andersen LB: School playground facilities as a determinant of children’s daily activity: a cross-sectional study of Danish primary school children. J Phys Act Health. 2012, 9 (1): 104.
Gubbels JS, Van Kan DH, Jansen MW: Play equipment, physical activity opportunities, and Children’s activity levels at childcare. J Environ Public Health. 2012, 2012: 326520-doi: 10.1155/2012/326520. Epub 2012 Jun 28.
Black N: Why we need observational studies to evaluate the effectiveness of health care. Br Med J. 1996, 312 (7040): 1215-10.1136/bmj.312.7040.1215.
Victora CG, Habicht JP, Bryce J: Evidence-based public health: moving beyond randomized trials. J Inf. 2004, 3 (3): 3.
Troiano RP, Berrigan D, Dodd KW, Mâsse LC, Tilert T, McDowell M: Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc. 2008, 40 (1): 181-10.1249/mss.0b013e31815a51b3.
Acknowledgements
The preparation of the manuscript was financially supported by the Dutch Ministry of Health, Welfare and Sport (VWS).
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
SdV had the original idea for the study which she further developed with AMS. AMS conducted the literature search and selected the studies based on the title and the abstract together with KB. KB and AMS developed a review protocol that was used by all authors to extract the data. The study outcomes were summarized and reported by KB who drafted the manuscript. AMS and SdV helped to draft the manuscript. All authors read and approved the final manuscript.
Electronic supplementary material
12966_2013_887_MOESM2_ESM.pdf
Additional file 2: Table S1. Methodological quality of experimental experimental (n = 13) and Table S2. Methodological quality of observational studies (n=17). (PDF 104 KB)
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article

Cite this article
Broekhuizen, K., Scholten, AM. & de Vries, S.I. The value of (pre)school playgrounds for children’s physical activity level: a systematic review. Int J Behav Nutr Phys Act 11, 59 (2014). https://doi.org/10.1186/1479-5868-11-59
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1479-5868-11-59