
Abstract
Background
Chronic diseases, such as chronic kidney disease (CKD), are growing in incidence and prevalence, in part due to an aging population. Support provided through home care services may be useful in attaining a more efficient and higher quality care for CKD patients.
Methods
A systematic review was performed to identify studies examining home care interventions among adult CKD patients incorporating all outcomes. Studies examining home care services as an alternative to acute, post-acute or hospice care and those for long-term maintenance in patients’ homes were included. Studies with only a home training intervention and those without an applied research component were excluded.
Results
Seventeen studies (10 cohort, 4 non-comparative, 2 cross-sectional, 1 randomized) examined the support provided by home care services in 15,058 CKD patients. Fourteen studies included peritoneal dialysis (PD), two incorporated hemodialysis (HD) and one included both PD and HD patients in their treatment groups. Sixteen studies focused on the dialysis phase of care in their study samples and one study included information from both the dialysis and pre-dialysis phases of care. Study settings included nine single hospital/dialysis centers and three regional/metropolitan areas and five were at the national level. Studies primarily focused on nurse assisted home care patients and mostly examined PD related clinical outcomes. In PD studies with comparators, peritonitis risks and technique survival rates were similar across home care assisted patients and comparators. The risk of mortality, however, was higher for home care assisted PD patients. While most studies adjusted for age and comorbidities, information about multidimensional prognostic indices that take into account physical, psychological, cognitive, functional and social factors among CKD patients was not easily available.
Conclusions
Most studies focused on nurse assisted home care patients on dialysis. The majority were single site studies incorporating small patient populations. There are gaps in the literature regarding the utility of providing home care to CKD patients and the impact this has on healthcare resources.
Similar content being viewed by others


Background
The world population is aging and the segment of global population 60 years of age and over is increasing at the fastest pace ever seen in history [1]. The population trends are reflected in the demographic profiles of patients with diseases such as chronic kidney disease (CKD) that are common in the elderly. In Canada, over half of the patients initiating renal replacement therapy (RRT) in 2009 were 65 years of age and older [2]. In Europe, RRT patients 65 years of age and older had the highest rate of increase in prevalence over the 1992–2005 period [3].
CKD populations, especially elderly end-stage renal disease (ESRD) patients, are faced with multiple medical and social challenges such as having to cope with several comorbidities, physical disability, cognitive impairment and social isolation [4–11]. These medical and social challenges are significant in characterizing the impaired quality of life in CKD patients [12, 13]. Quality of life deteriorates as the severity of CKD increases [14]. Home care (HC) services may help CKD patients in coping with these challenges, maintaining their independence and fulfilling their preferences of receiving care at home [15, 16].
Current emphasis on active aging and independence represent a unique opportunity to examine HC services that are utilized to varying degrees by different patient groups but are considered beneficial especially in chronic conditions [17]. In the case of non-ESRD CKD, the utilization of HC may vary based on patient’s age and comorbidities and, in the case of ESRD, it may vary based on the severity of illness and therapy type. HC services may help in supporting ESRD patients who have chosen conservative care. The independent treatment modalities for ESRD (peritoneal dialysis, PD, and home hemodialysis, HHD), emphasized as viable alternatives to facility-based treatment modalities over the last decade, are less costly to direct service providers, with equivalent or superior patient outcomes and quality of life [18–21]. Patients with ESRD, who are on PD or HHD, however, may utilize more HC services compared to those who are on a facility-based hemodialysis (HD), partially offsetting cost saving [22, 23]. On the other hand, the intensity of HC services received may reduce the number of hospitalizations and subsequent health system costs [24–26] regardless of the stage of CKD and the type of therapy for ESRD.
In general, HC services provide support to patients and help them with the daily management of their diseases in their communities. However, a proper characterization and a systematic evaluation of these services within a high risk, resource intense group of patients such as those with CKD have not been undertaken. This systematic review (SR) provides a rigorous account of research evidence on HC use among those with CKD.
Methods
Eligibility criteria
Studies about adult patients with any CKD severity level and a HC intervention regarding services provided in patients’ homes were eligible. Our SR was not restricted to studies that incorporated a comparison group. Studies with interventions related to the market place and working conditions of HC professionals or organizational underpinnings of HC organizations were excluded.
In the case of RRT, assisted PD patients could get help from a family member, a friend or a HC worker. In this SR, studies that focused on assisted PD in general without providing subgroup results for HC assisted PD patients [27–32] and those that examined home visits for reasons other than direct HC provision [33–36] were excluded. Unlike assisted PD, HHD is rarely available in an assisted format. One recent study that focused on the feasibility of nocturnal assisted HHD did not provide subgroup results for HC assisted HHD patients and, therefore, was not included in our SR [37].
In the case of palliative care, support services for CKD patients could be provided in their home or at a hospice. This study focused on home-based end-of-life care. Studies that examined palliative care without providing information about the specific services patients received in their community and those that did not separately report on subgroups of patients who received home-based support services [38–42] were excluded from our SR.
The primary outcomes included hospitalizations, admissions to institutional settings, length of stay on independent dialysis modalities for ESRD patients, and outcomes specific to treatment type. As secondary outcomes, mortality, medication management, patient satisfaction, caregiver satisfaction, physical and psychological well-being, health status and quality of life were considered. Studies were not excluded based on outcomes studied.
In general, all types of studies including experimental and observational studies were included. The studies that did not contain an empirical component and those with only training/educational and referral/recommendations types of interventions were excluded.
Given the diversity of HC services and resource considerations, we concentrated on studies published in English. To balance this limitation, a comprehensive literature search was undertaken. The date range was 1990 (i.e., the early stages of profound changes in healthcare systems that started with shifts away from acute care settings towards home and community care [43]) to present.
Definitions
CKD was conceptualized as consisting of five stages following the Kidney Disease Outcomes Quality Initiative’s definition accepted during the Kidney Disease: Improving Global Outcomes (KDIGO) conference [44]. The definition accepted during the KDIGO conference suggests that CKD could also be classified by treatment type: kidney transplant recipient, CKD independent of dialysis and CKD on dialysis. These classifications guided the development phase of our SR.
The Federal/Provincial/Territorial Working Group on Home Care’s definition, as reported by Health Canada, emphasizes the manner with which HC helps patients: “An array of services which enables clients, incapacitated in whole or part, to live at home, often with the affect of preventing, delaying or substituting for long-term or acute care alternatives” [45]. The Canadian Home Care Association’s definition focuses on the breadth of services covered: “an array of services, provided in the home and community setting, that encompasses health promotion and teaching, curative intervention, end-of-life care, rehabilitation, support and maintenance, social adaptation and integration and support for the family caregiver” [46]. Initially, HC conceptualization for this SR was guided by these definitions. These conceptualizations were further refined during the course of this study as we attempted to standardize terminology for our SR based on HC services covered in the included studies.
Information sources
Studies were identified through electronic databases, web sites, hand searches and consultations with experts in the field. Electronic databases included MEDLINE, EMBASE, CINAHL, PsycINFO, EconLit, Cochrane CENTRAL, Cochrane Methodology Register, Cochrane Database of Systematic Reviews, Centre for Reviews and Dissemination (DARE, HTA and NHS EED), ACP Journal Club and Web of Science (final search for MEDLINE is incorporated in the Appendix; final searches for other databases are available from the corresponding author). The web sites included World Health Organization, Health Canada, Canadian Homecare Association, Canadian Health Research Collection and the health departments of Canadian provinces and territories. The electronic database and web site searches, conducted by a University of British Columbia librarian, were completed on May 24, 2012. Hand searches, completed on September 20, 2013, were coupled with consultations with experts in the field.
Study selection
We followed a layered approach in study selection. An initial elimination of irrelevant studies was carried out by study assistants independently based on title and abstract reviews using a pre-tested selection form. An author (SKA) checked the initial selection and reviewed the complete texts of potentially relevant studies. The remaining manuscripts were reviewed in full by two additional authors independently (AL and PK). Disagreements were resolved after discussions among authors. Each selected study was summarized using a pre-tested data extraction form and was evaluated using the Agency for Healthcare Research and Quality risk of bias and confounding form developed for observational studies [47].
Analysis
Due to the heterogeneity of patient populations considered, interventions examined and health outcomes reported in the studies included in our SR, a meta-analysis was not possible. We performed a narrative summary of studies focusing mainly on key outcomes of importance to the CKD community.
Results
Study selection
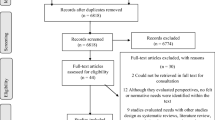
A total of 17 studies were identified for inclusion in the SR. The searches of electronic databases provided a total of 4354 citations (Figure 1) with 185 additional citations identified through hand-searches and author consultations. After adjustments for duplicates and title and abstract screening, a total of 521 full text articles were assessed and 17 were eligible for inclusion.

Chronic kidney disease & home care systematic review PRISMA flow diagram.
Study characteristics and patient populations
Of the 17 studies included in this study (overview of study characteristics in Table 1 and detail on patient populations, HC interventions and outcomes in Table 2), 14 focused on the impact HC has on PD patients. Ten of the PD studies were cohort studies [48–57], three were non-comparative [58–60] and one used cross sectional study design [61]. Five national level PD cohort studies [48, 51, 52, 55, 56] used information from the French Language Peritoneal Dialysis Registry (RDPLF). Two of these RDPLF studies [51, 52] used the same time period but applied different exclusion criteria based on the focus of the studies. Two PD cohort studies [53, 54] relied on data from regional dialysis units. The remaining three PD cohort studies [49, 50, 57] and all of the non-comparative and cross sectional PD studies [58–61] used data from a single hospital/dialysis unit. Of the 14 PD studies, 6 were from France [48, 50–52, 55, 56], 3 from Canada [53, 54, 58], 2 from the United States of America (USA) [60, 61] and one each from China [57], Taiwan [49] and Brazil [59].
Of the 17 studies included in this study, 2 studies examined the impact HC has on HD patients. One of these studies was a randomized trial [62] conducted in an Iranian hospital and the second one was a non-comparative study that used information from citywide dialysis units in the USA [63].
In contrast to the general trend of studies included in this SR where the focus was exclusively on the dialysis phase of care for patients, one study [64] included information from both the dialysis and pre-dialysis phases of care for PD and HD patients. This study explored the impact HC has on patients in one hospital in the United Kingdom.
The studies included in this SR examined HC in a total of 15,058 patients (Table 2). Patients on PD treatment (with a total of 14,954 patients) constituted the dialysis population that was most frequently studied. While most studies focused on general dialysis populations, two PD studies [58, 60] and one HD study [63] examined HC in special dialysis populations that had severe disability, terminal illness or complex comorbid conditions.
Of the 17 studies included in this review, 3 focused on elderly patients [48, 49, 53] with average age of the study samples ranging from 73 years [49] to 82 years [48]. In the remaining studies with pertinent information, average age ranged from 55 years [56, 61] to 69 years [63]. The PD studies with comparators and pertinent information revealed that HC assisted PD patients had a higher average age ranging from 71 years [57] to 83 years [48] when compared to the overall age of study samples.
Home care intervention
HC interventions primarily focused on the assistance provided during dialysis treatment (Table 2). The two studies that examined HC interventions for HD patients [62, 63] and most of the HC assisted PD studies [48, 50–53, 55, 56, 58, 60] focused on assistance dialysis patients received from a nurse. Two of the remaining studies [61, 64] considered the effects of HC teams and the rest focused on assistance received from either a home-assistant where a background in healthcare was not necessary [49, 57], a nurse assistant [59] or a nurse or a healthcare aid [54].
There are several factors, such as the severity of illness, the scope of HC provision and the requirements of dialysis technique used, that will influence the characteristics of a HC intervention. While patients on continuous cycling PD (CCPD) will mostly require two visits per day, those on continuous ambulatory PD (CAPD) may require one to four visits based on the severity of their disability [56, 58]. The time that a HC worker spends at a CAPD patient’s home is dependent on the CAPD system used. PD exchange help for a patient on an ultraviolet non-disconnect CAPD system will usually require less time (about 10–15 minutes) compared to the time (about 30–45 minutes) needed for a patient on a double-bag disconnect CAPD system [55].
Based on studies with pertinent information, patients in Canada [53, 54] were offered 14 visits per week for help with their PD exchanges and for the provision of clinical and social support. These patients received, on average, 5.8 visits per week during the first year of their dialysis [53]. In a USA program, a routine visit to a new PD patient was carried out to ensure proper installation of the cycler for an effective dialysis and non-routine visits were made only on an as-needed basis [61]. In this program, a visit took approximately four hours. Another USA program focused on ESRD patients with multiple medical and social problems [60]. In this program, a visit to help patients with their PD exchanges and to provide clinical and social support took, on average, 13 hours. In a HD study from Iran, the HC intervention was designed to conduct one visit per week before the HD schedule for clinical support and retraining [62].
Outcomes
Peritoneal dialysis
While most of the PD studies focused on outcomes related to PD treatment (Table 2), a few provided insights into how the availability of assisted PD offers a choice to patients who are unable to perform their RRT independently. A description of the PD population in France [55], where healthcare system supports nurse assisted PD, revealed that 45% of all PD patients and 87% of those over 90 years of age were assisted by a nurse. Studies have shown that the availability of nurse assisted PD increases the eligibility for PD among elderly patients [53] and improved the uptake of PD in general [50]. One study [54] emphasized the importance of the availability of family assistance for PD utilization even in regions where HC assisted PD is available.
In PD studies with comparators, outcomes such as peritonitis rate and technique and patient survival constituted the main areas of focus. In general PD populations, studies using information from RDPLF concluded that technique failure/transfer to HD was lower among HC (nurse) assisted PD patients when compared to self care PD patients only [51, 52] and to self care PD and family assisted PD patients as a group [51]. Another study in general PD populations [57], where home-assistants who were not required to have a background in healthcare helped PD patients, found that the probability of technique survival times were similar between HC assisted PD and family assisted PD patients. Studies that focused on elderly concluded that the probability of technique failure was similar between HC (nurse) assisted PD patients and comparators including patients on self care PD [48] and traditional modalities (i.e., self care PD and in-center HD) [53]. The probability of technique failure following an episode of peritonitis was also similar between home-assistant assisted PD and self care PD and family assisted PD patients [49].
Peritonitis rate was another outcome examined in PD studies with comparators. In almost all of these studies, HC assisted PD patients and the comparators (including family assisted PD among general PD populations [57], self care PD among elderly [48] and self care PD and family assisted PD among elderly [49]) had similar probabilities of being peritonitis free. In one study [52], HC assisted PD patients had lower peritonitis rates when compared to self care PD. In another study [56], HC assisted PD patients had higher peritonitis rates when compared to family assisted PD patients. However, the difference in peritonitis rates observed in the latter study disappeared when the effects of regular nurse visits from dialysis centers to the HC assisted PD patients were taken into consideration.
Most of the PD studies with comparators that examined patient survival found a higher probability of mortality among HC assisted PD patients. This result continued to hold across different comparators including self care PD among general PD populations [51, 52], self care PD and family assisted PD among general PD populations [51], family assisted PD among general PD populations [57], and self care PD among elderly PD populations [48]. Two studies about elderly populations were exceptions. In the first study, the risk of mortality did not differ between patients receiving nurse assisted PD and those on traditional modalities [53]. In the second study, peritonitis-related mortality was similar among home-assistant assisted PD and self care PD and family assisted PD patients [49].
The PD studies without comparators focused on varying outcomes such as identifying critical elements of a home visit [61] and exploring costs of RRTs [58]. The studies that considered PD patients with severe disability reported peritonitis rates that ranged from 1 episode per 13.0 patient-months [60] to 20.1 patient-months [58] and hospitalization rates that ranged from 1 admission per 6.0 patient-months [60] to15.3 patient-months [58]. A recent study from Brazil [59] found 1 peritonitis episode per 37.0 patient-months and 60% patient survival at one year among a general PD population.
Hemodialysis
The HD study with a comparator [62] concluded that patients in HC group had improved on 15 of the 19 outcomes considered (including decreases in nausea, vomiting, headache, bone pain, weakness and fatigue and itching and improvements in general condition and the levels of creatinine, potassium and phosphorus of the blood). The HD study without a comparator [63] focused on patients diagnosed with terminal illness and found that, on average, patients were hospitalized for 9.43 days.
Pre-dialysis and dialysis
Based on survey results, more than three-fourths of PD and HD patients were very satisfied with the pre-dialysis and dialysis phase of their care after the implementation of HC program [64]. The HC team consisting of three nurses and one renal care assistant provided continuous social support to patients. The HC team also collected information about patients’ life goals and provided information to them about their dialysis modalities.
Risk of bias and confounding
While most studies had low risk of bias in many domains (Table 3), apart from two studies [51, 52] that used imputations techniques for missing information, loss to follow-up was rarely discussed. Some of the studies [48, 49, 51–53, 56, 57] have taken into consideration confounding variables such as age and Charlson Comorbidity Index (CCI). The CCI summarizes the impact comorbid conditions have on survival by assigning higher weights to more severe coexisting conditions such as metastatic carcinoma and lower weights to less severe ones such as dementia [65–67]. While CCI is one of the most widely used risk adjustment techniques in observational studies, the characteristics of CKD populations may require multidimensional prognostic indices that take into account physical, psychological, cognitive, functional and social factors [68]. One of the studies included in this SR reported on the physical performance of patients using Karnofsky Scale in addition to providing information on their comorbidity scores [59]. Apart from the descriptive information incorporated in the latter study, there were no studies that incorporated multidimensional indices as another confounding variable in their analysis.
Discussion
Our SR revealed that most of the studies that examined the impact of HC services among CKD patients focused on dialysis patients, in general, and PD patients, in particular. Among RRTs, assisted PD provides an option for ESRD patients who prefer home-based dialysis therapies but have barriers to self care including physical disability and cognitive impairment. HC assisted PD becomes especially valuable for ESRD patients with additional barriers to self care such as social isolation. The current increases in the prevalence of elderly ESRD patients partly explain the greater emphasis placed on assisted PD in the CKD HC literature.
The HC assisted PD studies incorporated in this review mostly underscored clinically relevant outcomes for PD such as peritonitis rate and technique and patient survival. The findings show that technique survival and peritonitis rates for HC assisted PD patients were at least similar to or better than those for self care PD and family assisted PD patients. The studies that found better technique survival [51, 52] and peritonitis rates [52] for HC (nurse) assisted PD patients relied on national level French registry using the same time period. The availability of HC assisted PD may reduce the likelihood of adverse events by improving patient’s psycho-social status and supporting them in adhering to the basic principles of PD including peritonitis prevention. Further studies are needed to examine if favorable outcomes continue to hold for HC assisted PD patients in different regions across the world.
Most PD studies found a higher probability of mortality among HC assisted PD patients when compared to self care PD or family assisted PD. These studies indicated that patients in their HC assisted PD group were older and had higher levels of comorbidities as captured by the CCI. The higher probability of mortality among HC assisted PD patients persisted in studies that controlled for age and CCI differences across groups. The authors mostly attributed this finding to data insufficiencies in capturing disabilities among PD populations. Apart from one study [59] that described comorbidity and physical performance in their study population, there were no studies that incorporated multidimensional indices that take into account physical, psychological, cognitive, functional and social factors as another confounding variable in their analysis.
The studies included in this SR provided limited information about the characteristics of the HC interventions. In general, technical requirements imposed on HC intervention based on the dialysis type used are well known among the CKD community. Additional studies that consider HC interventions with varying scope and frequency and duration of visits in different CKD populations will provide helpful information to the CKD community, especially for those who are considering HC programs for their own clinic/practice.
One of the gaps in the literature that was identified by our SR is related to the provision of HC services among non-ESRD CKD populations. Apart from one study [64] that incorporated information about patient experiences with the implementation of a HC program that affected both the dialysis and pre-dialysis phases of their care, there were no studies that explored the impact HC has on non-ESRD CKD populations. It is well known that CKD is often accompanied by several comorbid conditions, is common among older people and its prevalence increases with age. As emphasized by the World Kidney Day 2014 Steering Committee [69], these characteristics of CKD coupled with increased life expectancy worldwide call for further explorations into ways of optimizing health for elderly populations. The impact different HC services might have in improving health among non-ESRD CKD patients is one such area that deserves further explorations.
The lack of studies on the impact home palliative care has on patients with CKD is another gap in the literature that was identified by our SR. The quality of life considerations for CKD patients who are at the advance stages of their disease require focus on several issues including the management of their physical and psycho-social symptoms and the development of an advanced care plan that sets the goals for their care [70–74]. Studies that examine the impact home palliative care has on patients with CKD who are at the advance stages of their disease will help further advance the integration of palliative and renal care.
Our SR identified other gaps in the literature. There were no studies about HC provision among kidney transplant patients. Studies related to HC provision among HD patients were limited to small samples.
The HC interventions incorporated in the CKD literature were mostly limited to nursing care for ESRD patients. There were no studies about the provision of home support for activities of daily living or respite care for caregivers of CKD patients. While HC may become more important as CKD severity increases and, in the case of ESRD, it may be most useful for patients on home-based dialysis modalities or for those who choose conservative care, further studies are needed to quantify these differing levels of HC use and its impact.
One of the strengths of our study is the comprehensive SR conducted on a topic where there were, to the best of our knowledge, no previous SR undertaken. The comprehensive electronic database searches coupled with hand searches and expert consultations resulted in the identification of several gaps in the literature.
Our study has several limitations. One of the limitations of our study is arising from the subject matter itself. HC, as encompassing a diverse set of medical and psycho-social services, is one of the health services research areas that are constantly evolving with limited standardization in terminology. Our study which focused on the intersection of home care with CKD faced additional challenges given the changes in CKD definition itself in the past years that is continuing through today [75]. We made an attempt to balance this fundamental limitation by conducting comprehensive database searches, extensive hand searches and expert consultations. Second limitation of our study is the layered approached followed in study selection. Third limitation is the focus on studies published in English. Given the diversity of HC services, resource and time considerations were crucial factors in our decision to follow a layered study selection approach and to focus on studies published in English. As indicated above, we made an attempt to balance these limitations by conducting comprehensive database searches, extensive hand searches and expert consultations. Another limitation is our inability to conduct a meta-analysis for our study. The diversity of patient populations, HC interventions and outcomes studied made it impossible to conduct a meta-analysis.
Conclusions
In this era of aging world population and medical and technical advances, chronic diseases, such as CKD, are growing in incidence and prevalence. HC may be useful in providing a more efficient and higher quality care for CKD patients. However, a synthesis of evidence on the effects of HC among CKD patients has not been undertaken. Our SR, which aimed at filling this void, revealed that extant studies almost exclusively focused on nurse assisted HC patients examining mostly PD related clinical outcomes. Our study concluded that there are several gaps in the literature. Specifically, there were no studies in areas such as home support for activities of daily living, palliative care at home or respite care for caregivers of CKD patients, in general, or for ESRD patients, in particular.
Appendix
MEDLINE Search Strategy:
-
1.
exp kidney diseases/
-
2.
exp renal replacement therapy/
-
3.
((kidney or renal) adj2 (disease* or failure or damage or insufficiency)).mp.
-
4.
((kidney or renal) adj2 (transplant*5 or dysfunction or therap*)).mp.
-
5.
(dialysis or dialyses or haemodialysis).mp.
-
6.
Kidney, Artificial/
-
7.
(kidney* adj artificial).mp.
-
8.
or/1-7 (540012)
-
9.
exp home care services/
-
10.
(domiciliary adj3 (care or service$ or nurs$)).mp.
-
11.
“home nurs$3”.mp.
-
12.
((home or care) adj3 (nonprofession$ or non-professional$)).mp.
-
13.
(homemaker adj3 service$).mp.
-
14.
(home adj3 service$).mp.
-
15.
“home care”.mp.
-
16.
(home adj3 (renal or dialys$3 or hemodialy$3 or peritoneal)).mp.
-
17.
((parenteral or nutrition or feeding) adj home).mp.
-
18.
(“hospital at home” or “hospital in the home” or “in-home care”).mp.
-
19.
“home health care”.mp.
-
20.
(Home adj3 (rehabilitation or occupational or physical or physiotherap$ or social worker$ or speech)).mp.
-
21.
Day Care/
-
22.
(palliative adj5 home).mp.
-
23.
((caregiver$ or care-giver$ or carer$) adj3 “respite care”).mp.
-
24.
((long-term or long term) adj3 (home care or home-care)).mp.
-
25.
activities of daily living.sh. and home.tw.
-
26.
(personal care adj3 home).mp.
-
27.
(self-care adj3 home).mp.
-
28.
(day adj3 care).mp.
-
29.
self care.sh. and home.tw.
-
30.
or/9-29
-
31.
8 and 30
-
32.
limit 31 to (english language and yr=“1990 -Current”)
-
33.
limit 32 to “all child (0 to 18 years)”
-
34.
32 not 33.
Abbreviations
- CKD:
-
Chronic kidney disease
- RRT:
-
Renal replacement therapy
- ESRD:
-
End-stage renal disease
- HC:
-
Home care
- PD:
-
Peritoneal dialysis
- HD:
-
Hemodialysis
- HHD:
-
Home hemodialysis
- SR:
-
Systematic review
- KDIGO:
-
Kidney Disease: Improving Global Outcomes
- RDPLF:
-
French Language Peritoneal Dialysis Registry
- CCI:
-
Charlson Comorbidity Index
- CCPD:
-
Continuous cycling PD
- CAPD:
-
Continuous ambulatory PD.
References
United Nations, Department of Economic and Social Affairs, Population Division: World Population Prospects: the 2010 Revision, Highlights and Advance Tables. 2011, Working Paper No. ESA/P/WP.220
Canadian Institute for Health Information: Canadian Organ Replacement Register Annual Report: Treatment of end-Stage Organ Failure in Canada, 2000 to 2009. 2011, Ottawa: Canadian Institute for Health Information
Zoccali C, Kramer A, Jager KJ: Chronic kidney disease and end-stage renal disease–a review produced to contribute to the report ‘Status of health in the European Union: towards a healthier Europe’. NDT Plus. 2010, 3: 213-224.
Davison SN: Pain in hemodialysis patients: prevalence, cause, severity, and management. Am J Kidney Dis. 2003, 42 (6): 1239-1247.
Brown EA: Epidemiology of renal palliative care. J Palliat Med. 2007, 10 (6): 1248-1252.
Fan SL, Sathick I, McKitty K, Punzalan S: Quality of life of caregivers and patients on peritoneal dialysis. Nephrol Dial Transplant. 2008, 23 (5): 1713-1719.
Kurella M, Covinsky KE, Collins AJ, Chertow GM: Octogenarians and nonagenarians starting dialysis in the United States. Ann Intern Med. 2007, 146 (3): 177-183.
Cook WL, Jassal SV: Functional dependencies among the elderly on hemodialysis. Kidney Int. 2008, 73 (11): 1289-1295.
Weiner DE, Scott TM, Giang LM, Agganis BT, Sorensen EP, Tighiouart H, Sarnak MJ: Cardiovascular disease and cognitive function in maintenance hemodialysis patients. Am J Kidney Dis. 2011, 58 (5): 773-781.
Brown EA: How to address barriers to peritoneal dialysis in the elderly. Perit Dial Int. 2011, 31 (Suppl 2): S83-S85.
Jager KJ, Korevaar JC, Dekker FW, Krediet RT, Boeschoten EW: The effect of contraindications and patient preference on dialysis modality selection in ESRD patients in the Netherlands. Am J Kidney Dis. 2004, 43 (5): 891-899.
Soni RK, Weisbord SD, Unruh ML: Health-related quality of life outcomes in chronic kidney disease. Curr Opin Nephrol Hypertens. 2010, 19 (2): 153-159.
Finkelstein FO, Arsenault KL, Taveras A, Awuah K, Finkelstein SH: Assessing and improving the health-related quality of life of patients with ESRD. Nat Rev Nephrol. 2012, 8 (12): 718-724.
Pagels AA, Soderkvist BK, Medin C, Hylander B, Heiwe S: Health-related quality of life in different stages of chronic kidney disease and at initiation of dialysis treatment. Health Qual Life Outcomes. 2012, 10: 71-
Canadian Healthcare Association: Home Care in Canada: From the Margins to the Mainstream. 2009, Ottawa, Ontario: CHCA
Prakash S, Perzynski AT, Austin PC, Wu CF, Lawless ME, Paterson JM, Quinn RR, Sehgal AR, Oliver MJ: Neighborhood socioeconomic status and barriers to peritoneal dialysis: a mixed methods study. Clin J Am Soc Nephrol. 2013, 8 (10): 1741-1749.
World Health Organization: Active Ageing: A Policy Framework. 2002, Geneva: World Health Organization
Lee H, Manns B, Taub K, Ghali WA, Dean S, Johnson D, Donaldson C: Cost analysis of ongoing care of patients with end-stage renal disease: the impact of dialysis modality and dialysis access. Am J Kidney Dis. 2002, 40 (3): 611-622.
McFarlane PH, Pierratos A, Redelmeier DA: Cost savings of home nocturnal versus conventional in-center hemodialysis. Kidney Int. 2002, 62: 2216-2222.
Kroeker A, Clark WF, Heidenheim AP, Kuenzig L, Leitch R, Meyette M, Muirhead N, Ryan H, Welch R, White S, Lindsay RM: An operating cost comparison between conventional and home quotidian hemodialysis. Am J Kidney Dis. 2003, 42 (Suppl 1): 49-55.
Komenda P, Chan C, Pauly RP, Levin A, Copland M, Pierratos A, Sood MM: The evaluation of a successful home hemodialysis program: establishing a prospective framework for quality. Clin Nephrol. 2009, 71 (5): 467-474.
Dratwa M: Costs of home assistance for peritoneal dialysis: results of a European survey. Kidney Int. 2008, 73 (Suppl 108s): S72-S75.
Grun RP, Constantinovici N, Normand C, Lamping DL: Costs of dialysis for elderly people in the UK. Nephrol Dial Transplant. 2003, 18 (10): 2122-2127.
De Vecchi AF, Dratwa M, Wiedemann ME: Healthcare systems and end-stage renal disease (ESRD) therapies–an international review: costs and reimbursement/funding of ESRD therapies. Nephrol Dial Transplant. 1999, 14 (Suppl 6): 31-41.
Li PK, Cheung WL, Lui SL, Blagg C, Cass A, Hooi LS, Lee HY, Locatelli F, Wang T, Yang CW, Canaud B, Cheng YL, Choong HL, de Francisco AL, Gura V, Kaizu K, Kerr PG, Kuok UI, Leung CB, Lo WK, Misra M, Szeto CC, Tong KL, Tungsanga K, Walker R, Wong AK, Yu AW: Increasing home based dialysis therapies to tackle dialysis burden around the world: a position statement on dialysis economics from the 2nd Congress of the International Society for Hemodialysis. Nephrology (Carlton). 2011, 16 (1): 53-56.
Collins AJ, Foley RN, Chavers B, Gilbertson D, Herzog C, Johansen K, Kasiske B, Kutner N, Liu J, Peter W, Guo H, Gustafson S: USRDS 2011 annual data report–atlas of chronic kidney disease and end-stage renal disease in the United States: costs of ESRD. Am J Kidney Dis. 2012, 59 (Suppl 1): e281-e290.
Povlsen JV, Ivarsen P: Assisted automated peritoneal dialysis (AAPD) for the functionally dependent and elderly patient. Perit Dial Int. 2005, 25 (Suppl 3): S60-S63.
Smyth A, McCann E, Redahan L, Lambert B, Mellotte GJ, Wall CA: Peritoneal dialysis in an ageing population: a 10-year experience. Int Urol Nephrol. 2012, 44 (1): 283-293.
Cheng CH, Shu KH, Chuang YW, Huang ST, Chou MC, Chang HR: Clinical outcome of elderly peritoneal dialysis patients with assisted care in a single medical center - a 25-year experience. Nephrology (Carlton). 2013, 18 (6): 468-473.
Jagose JT, Afthentopoulos IE, Shetty A, Oreopoulos DG: Successful use of continuous ambulatory peritoneal dialysis in octogenarians. Adv Perit Dial. 1996, 12: 126-131.
Szeto CC, Kwan BC, Chow KM: Peritonitis risk for older patients on peritoneal dialysis. Perit Dial Int. 2008, 28 (5): 457-460.
Sunder S, Taskapan H, Jojoa J, Krishnan M, Khandelwal M, Izatt S, Chu M, Subramanian P, Chinthalapalli H, Lobbedez T, Jassal SV, Bargman JM, Oreopoulos DG: Chronic peritoneal dialysis in the tenth decade of life. Int Urol Nephrol. 2004, 36 (4): 605-609.
Castro MJ, Celadilla O, Munoz I, Martinez V, Minguez M, Auxiliadora Bajo M, del Peso G: Home training experience in peritoneal dialysis patients. EDTNA ERCA J. 2002, 28 (1): 36-39.
Ozturk S, Yucel L, Guvenc S, Ekiz S, Kazancioglu R: Assessing and training patients on peritoneal dialysis in their own homes can influence better practice. J Ren Care. 2009, 35 (3): 141-146.
Russo R, Manili L, Tiraboschi G, Amar K, De Luca M, Alberghini E, Ghiringhelli P, De Vecchi A, Porri MT, Marinangeli G, Rocca R, Paris V, Ballerini L: Patient re-training in peritoneal dialysis: why and when it is needed. Kidney Int. 2006, 70 (Suppl 103s): S127-S132.
Bernardini J, Nagy M, Piraino B: Pattern of noncompliance with dialysis exchanges in peritoneal dialysis patients. Am J Kidney Dis. 2000, 35 (6): 1104-1110.
Tennankore KK, Kim SJ, Chan CT: The feasibility of caregiver-assisted home nocturnal hemodialysis. Nephron Clin Pract. 2012, 122 (1–2): 17-23.
Cohen LM, Germain M, Poppel DM, Woods A, Kjellstrand CM: Dialysis discontinuation and palliative care. Am J Kidney Dis. 2000, 36 (1): 140-144.
Smith C, Da Silva-Gane M, Chandna S, Warwicker P, Greenwood R, Farrington K: Choosing not to dialyse: evaluation of planned non-dialytic management in a cohort of patients with end-stage renal failure. Nephron Clin Pract. 2003, 95 (2): c40-c46.
Chandna SM, Da Silva-Gane M, Marshall C, Warwicker P, Greenwood RN, Farrington K: Survival of elderly patients with stage 5 CKD: comparison of conservative management and renal replacement therapy. Nephrol Dial Transplant. 2011, 26 (5): 1608-1614.
Chater S, Davison SN, Germain MJ, Cohen LM: Withdrawal from dialysis: a palliative care perspective. Clin Nephrol. 2006, 66 (5): 364-372.
Yong DS, Kwok AO, Wong DM, Suen MH, Chen WT, Tse DM: Symptom burden and quality of life in end-stage renal disease: a study of 179 patients on dialysis and palliative care. Palliat Med. 2009, 23 (2): 111-119.
Tully P, Saint-Pierre E: Downsizing Canada’s hospitals, 1986/87 to 1994/95. Health Rep. 1997, 8 (4): 33-39.
Levey AS, Eckardt KU, Tsukamoto Y, Levin A, Coresh J, Rossert J, De Zeeuw D, Hostetter TH, Lameire N, Eknoyan G: Definition and classification of chronic kidney disease: a position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2005, 67 (6): 2089-2100.
Health Canada: Home care in Canada 1999: an overview. [http://www.hc-sc.gc.ca/hcs-sss/pubs/home-domicile/1999-home-domicile/index-eng.php]
Canadian Home Care Association: Making Connections: Sharing Knowledge and Building Communities, 2009, a Year in Review. 2010, Mississauga, Ontario: CHCA
Viswanathan M, Berkman ND, Dryden DM, Hartling L: Assessing Risk of Bias and Confounding in Observational Studies of Interventions or Exposures: Further Development of the RTI Item Bank. Methods Research Report. (Prepared by RTI-UNC Evidence-Based Practice Center Under Contract No. 290-2007-10056-I). 2013/09/06 edn. 2013, Rockville, MD: Agency for Healthcare Research and Quality
Castrale C, Evans D, Verger C, Fabre E, Aguilera D, Ryckelynck JP, Lobbedez T: Peritoneal dialysis in elderly patients: report from the French Peritoneal Dialysis Registry (RDPLF). Nephrol Dial Transplant. 2010, 25 (1): 255-262.
Hsieh CY, Fang JT, Yang CW, Lai PC, Hu SA, Chen YM, Yu CC, Tian YC, Chien CC, Hung CC: The impact of type of assistance on characteristics of peritonitis in elderly peritoneal dialysis patients. Int Urol Nephrol. 2010, 42 (4): 1117-1124.
Lobbedez T, Moldovan R, Lecame M, Hurault de Ligny B, El Haggan W, Ryckelynck JP: Assisted peritoneal dialysis. Experience in a French renal department. Perit Dial Int. 2006, 26 (6): 671-676.
Lobbedez T, Verger C, Ryckelynck JP, Fabre E, Evans D: Is assisted peritoneal dialysis associated with technique survival when competing events are considered?. Clin J Am Soc Nephrol. 2012, 7 (4): 612-618.
Lobbedez T, Verger C, Ryckelynck JP, Fabre E, Evans D: Outcome of the sub-optimal dialysis starter on peritoneal dialysis. Report from the French Language Peritoneal Dialysis Registry (RDPLF). Nephrol Dial Transplant. 2013, 28 (5): 1276-1283.
Oliver MJ, Quinn RR, Richardson EP, Kiss AJ, Lamping DL, Manns BJ: Home care assistance and the utilization of peritoneal dialysis. Kidney Int. 2007, 71 (7): 673-678.
Oliver MJ, Garg AX, Blake PG, Johnson JF, Verrelli M, Zacharias JM, Pandeya S, Quinn RR: Impact of contraindications, barriers to self-care and support on incident peritoneal dialysis utilization. Nephrol Dial Transplant. 2010, 25 (8): 2737-2744.
Verger C, Ryckelynck JP, Duman M, Veniez G, Lobbedez T, Boulanger E, Moranne O: French peritoneal dialysis registry (RDPLF): outline and main results. Kidney Int. 2006, 70 (Suppl 103s): S12-S20.
Verger C, Duman M, Durand PY, Veniez G, Fabre E, Ryckelynck JP: Influence of autonomy and type of home assistance on the prevention of peritonitis in assisted automated peritoneal dialysis patients. An analysis of data from the French Language Peritoneal Dialysis Registry. Nephrol Dial Transplant. 2007, 22 (4): 1218-1223.
Xu R, Zhuo M, Yang Z, Dong J: Experiences with assisted peritoneal dialysis in China. Perit Dial Int. 2012, 32 (1): 94-101.
Brunier G, Gray B, Coulis N, Savage J, Manuel A, McConnell H, Mildon B, Sherlock AM: The use of community nurses for home peritoneal dialysis: is it cost-effective?. Perit Dial Int. 1996, 16 (Suppl 1): S479-S482.
Franco MR, Fernandes N, Ribeiro CA, Qureshi AR, Divino-Filho JC, da Gloria LM: A Brazilian experience in assisted automated peritoneal dialysis: a reliable and effective home care approach. Perit Dial Int. 2013, 33 (3): 252-258.
Wadhwa NK, Suh H, Cabralda T, Sokol E, Sokunbi D, Solomon M: Peritoneal dialysis with trained home nurses in elderly and disabled end-stage renal disease patients. Adv Perit Dial. 1993, 9: 130-133.
Ponferrada L, Prowant BF, Schmidt LM, Burrows LM, Satalowich RJ, Bartelt C: Home visit effectiveness for peritoneal dialysis patients. ANNA J. 1993, 20 (3): 333-336.
Babamohammadi H, Khalili H: Effect of a confined program of home-care on the health status of patients receiving hemodialysis. Acta Med Iran. 2006, 44 (1): 28-32.
Agraharkar M, Barclay C, Agraharkar A: Staff-assisted home hemodialysis in debilitated or terminally ill patients. Int Urol Nephrol. 2002, 33 (1): 139-144.
Wilde C, Macefield J: Improvement in care: a collaborative approach to rehabilitation. EDTNA ERCA J. 2001, 27 (2): 69-71.
Charlson ME, Pompei P, Ales KL, MacKenzie CR: A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987, 40 (5): 373-383.
Deyo RA, Cherkin DC, Ciol MA: Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992, 45 (6): 613-619.
Hemmelgarn BR, Manns BJ, Quan H, Ghali WA: Adapting the Charlson Comorbidity Index for use in patients with ESRD. Am J Kidney Dis. 2003, 42 (1): 125-132.
Pilotto A, Panza F, Sancarlo D, Paroni G, Maggi S, Ferrucci L: Usefulness of the multidimensional prognostic index (MPI) in the management of older patients with chronic kidney disease. J Nephrol. 2012, 25 (Suppl 19): S79-S84.
Tonelli M, Riella M: Chronic kidney disease and the ageing population. Intern Med J. 2014, 44 (3): 213-217.
Davison SN: Integrating palliative care for patients with advanced chronic kidney disease: recent advances, remaining challenges. J Palliat Care. 2011, 27 (1): 53-61.
Kurella Tamura M, Cohen LM: Should there be an expanded role for palliative care in end-stage renal disease?. Curr Opin Nephrol Hypertens. 2010, 19 (6): 556-560.
Hussain JA, Russon L: Supportive and palliative care for people with end-stage renal disease. Br J Hosp Med (Lond). 2012, 73 (11): 640-644.
Cohen LM, Moss AH, Weisbord SD, Germain MJ: Renal palliative care. J Palliat Med. 2006, 9 (4): 977-992.
Levy JB, Chambers EJ, Brown EA: Supportive care for the renal patient. Nephrol Dial Transplant. 2004, 19 (6): 1357-1360.
Pugliese G, Solini A, Bonora E, Orsi E, Zerbini G, Fondelli C, Gruden G, Cavalot F, Lamacchia O, Trevisan R, Vedovato M, Penno G: Distribution of cardiovascular disease and retinopathy in patients with type 2 diabetes according to different classification systems for chronic kidney disease: a cross-sectional analysis of the renal insufficiency and cardiovascular events (RIACE) Italian multicenter study. Cardiovasc Diabetol. 2014, 13 (1): 59-
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2369/15/118/prepub
Acknowledgements
This research is supported by an Allied Health Research grant (no.KFOC110022) from the Kidney Foundation of Canada. The authors thank Sharon Stevens for electronic searches. Research assistants Simon Tai, Mithila Makhijani, Thomas Ferguson and Michelle Wong provided excellent support in the earlier phases of this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
SKA contributed to the conception and design, analysis and interpretation of results, and drafted the manuscript. PK contributed to the conception and design, interpretation of results and provided input for manuscript revision. OD contributed to the interpretation of results and provided input for manuscript revision. AL contributed to the conception and design, interpretation of results and provided input for manuscript revision. All authors have read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Aydede, S.K., Komenda, P., Djurdjev, O. et al. Chronic kidney disease and support provided by home care services: a systematic review. BMC Nephrol 15, 118 (2014). https://doi.org/10.1186/1471-2369-15-118
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2369-15-118