
Abstract
Background
Saliva and urine have been used for arthropod-borne viruses molecular detection but not yet for chikungunya virus (CHIKV). We investigated the use of saliva and urine for molecular detection of CHIKV during the French Polynesian outbreak.
Methods
During the French Polynesian chikungunya outbreak (2014–2015), we collected the same day blood and saliva samples from 60 patients with probable chikungunya (47 during the 1st week post symptoms onset and 13 after), urine was available for 39 of them. All samples were tested using a CHIKV reverse-transcription PCR.
Results
Forty eight patients had confirmed chikungunya. For confirmed chikungunya presenting during the 1st week post symptoms onset, CHIKV RNA was detected from 86.1 % (31/36) of blood, 58.3 % (21/36) of saliva and 8.3 % (2/24) of urine. Detection rate of CHIKV RNA was significantly higher in blood compared to saliva. For confirmed chikungunya presenting after the 1st week post symptoms onset, CHIKV RNA was detected from 8.3 % (1/12) of blood, 8.3 % (1/12) of saliva and 0 % (0/8) of urine.
Conclusions
In contrast to Zika virus (ZIKV), saliva did not increased the detection rate of CHIKV RNA during the 1st week post symptoms onset. In contrast to ZIKV, dengue virus and West Nile virus, urine did not enlarged the window of detection of CHIKV RNA after the 1st week post symptoms onset. Saliva can be used for molecular detection of CHIKV during the 1st week post symptoms onset only if blood is impossible to collect but with a lower sensitivity compared to blood.
Similar content being viewed by others
Background
French Polynesia (FP), south Pacific, is a high endemic area for arthropod-borne viruses (arboviruses) [1]. Until 2013, dengue virus (DENV) (arbovirus of the genus Flavivirus) has been the only arbovirus detected in FP, causing multiple outbreaks from the 1960s [2]. Zika virus (ZIKV) (arbovirus of the genus Flavivirus), emerged in FP in 2013 causing an outbreak from October 2013 to April 2014 [3, 4]. Chikungunya virus (CHIKV) (arbovirus of the genus Alphavirus) [5], emerged in the Pacific in 2011 and subsequently spread throughout the region [6]. A CHIKV outbreak occurred in FP from October 2014 to March 2015 [7] with an estimate of 66,000 cases (about 25 % of the population) [6].
During the FP ZIKV outbreak, we developed molecular ZIKV detection on saliva as an alternative sample to blood [8]. The ability to detect ZIKV was higher in saliva compared to blood at the acute phase of the illness. This protocol was of particular interest when blood was difficult to collect, especially for children and neonates. For ZIKV [9–11], DENV [12, 13] or West Nile virus (WNV) [14, 15], the use of urine for molecular diagnosis can enlarge the window of detection of these arboviruses.
As alternative sample to blood have been reported to increase the detection rate or to enlarge the window of detection of arboviruses, we investigated the use of saliva and urine for CHIKV molecular detection during the FP CHIKV outbreak.
Methods
The study was conducted in FP over a 4 months period from November 2014 to February 2015, during the FP CHIKV outbreak.
Patients presenting in our laboratory with a medical prescription for chikungunya diagnosis were asked to provide, in addition to blood, saliva and urine sample. A standardized medical questionnaire form was available for all patients, it included the numbers of days after symptoms onset and the main clinical symptoms.
After informed written consent was obtained, blood was collected by venous puncture, saliva was collected with dry cotton swabs without transport media (N° 150C, Copan, Brescia, Italy), and urine was collected on sterile containers without additives. We included in the study patients with possible chikungunya infection with both blood and saliva, and if possible urine, samples collected at the same time.
Case definition for possible and confirmed CHIKV were defined according the World Health Organization [16] and European Center for Diseases Prevention and Control [17] criteria. Possible cases were patient with clinical criteria of chikungunya (acute onset of fever > 38.5 °C and severe arthralgia/arthritis) not explained by other medical conditions; confirmed cases were patient meeting the laboratory criteria [virus isolation or presence of viral RNA by Reverse Transcription (RT)-PCR] presence of virus specific IgM antibodies in single serum sample collected in acute or convalescent stage, four-fold increase in IgG values in sample collected at least 3 weeks apart), irrespective of the clinical presentation.
According to the French recommendations [18] blood samples were tested by RT-PCR for patients collected from days 1 to 4 post symptoms onset (PSO), by RT-PCR and serology for patients collected from days 5 to 7 PSO and by serology for patients collected after day 7 PSO. In order to compare the use of RT-PCR in saliva and urine to blood, all samples were tested by CHIKV RT-PCR, including blood samples collected after day 7 PSO.
For molecular detection of CHIKV, RNA extraction was performed using the NucliSENS® easyMAG® System (BioMérieux) according to manufacturer’s recommendations. Two hundred μl of serum or 500 μl of urine were added to 2 ml of lysis buffer, oral swabs were first vortexed in 2 ml of lysis buffer, then all were eluted by elution buffer and 5 μl of extracted RNA was used for amplification on a CFX96 Touch™ Real-Time PCR detection System (Biorad) using primers/probe amplification sets specific for CHIKV as previously reported [7, 19].
Immunoglobulin M (IgM) detection was performed using Novalisa Chikungunya IgG/IgM μ-capture ELISA kit (NovaTec Immundiagnostica GmbH, Germany) according to the recommendations of the supplier.
Results
Sixty patients were included in the study, of them 48 had confirmed chikungunya (36 presenting during the 1st week PSO and 12 after), 32 infections have been confirmed by detection of CHIKV RNA and 16 by detection of specific IgM antibodies against CHIKV (Table 1).
Blood and saliva were available from all patients. Urine was available from 39 patients (32 from confirmed chikungunya).
Saliva and urines RT-PCR results for patients with confirmed chikungunya are reported in Tables 2 and 3 respectively.
For confirmed chikungunya presenting during the 1st week PSO, CHIKV RNA was detected from 86.1 % (31/36) of blood, 58.3 % (21/36) of saliva and 8.3 % (2/24) of urine. Detection rate was significantly higher in blood compared to saliva (Fisher's exact test, p = 0.008), it was not significantly higher in blood compared to urine (Fisher's exact test, p = 1) but the number of patients was too small to observe a significant difference.
Samples testing positive in urine by RT-PCR were collected on days 3 and 5 PSO.
For confirmed chikungunya presenting after the 1st week PSO, CHIKV RNA was detected from 8.3 % (1/12) of blood, 8.3 % (1/12) of saliva and 0 % (0/8) of the urine. Detection rate was not significantly different when we compared blood to saliva (Fisher's exact test, p = 0.08) and urine (Fisher's exact test, p = 0.08).
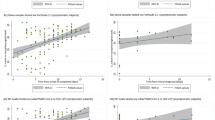
The proportion of positive RT-PCR saliva samples according to the number of days PSO is reported in Fig. 1.

Proportion of positive samples according to the number of days after symptoms onset for the 60 patients with both blood (blue) and saliva (red) samples tested by ZIKV RT-PCR
None of the 12 patients who tested negative by CHIKV-RT-PCR in blood was positive in saliva and/or urine.
Discussion
Urine and saliva as alternative samples to blood have been used successfully for molecular arbovirus detection [8–15, 20–26].
During the FP ZIKV outbreak, the use of saliva increased the detection rate of ZIKV RNA at the acute phase of the disease [8], saliva was also used to detect ZIKV from an Australian traveller returning from Indonesia [20]. Detection of dengue virus (DENV) RNA in saliva was reported [12, 21]. CHIKV RNA and infectious CHIKV in saliva were found only in patients with gingivorrhagia [22]. In our study, none of the 22 patients with saliva testing positive for CHIKV reported hemorrhagic manifestations, nevertheless we cannot exclude that subclinical gingivorrhagia were responsible of positivity of saliva due to contamination by viremic blood. In contrast to ZIKV [8], CHIKV detection in saliva did not increased the rate of molecular detection of CHIKV. As saliva was positive in 58.3 % of confirmed chikungunya presenting during the 1st week PSO, saliva can be of interest for molecular CHIKV detection only if blood samples are impossible to collect, especially if collected from the first 3 days PSO.
Arbovirus detection in urine was reported at the acute and late phase of dengue [12, 13, 23], WNV [14, 15], CHIKV [26] and ZIKV infection [9–11, 24, 25]; and during Japanese encephalitis [27] and yellow fever [28] infections. The main interest of urine was to enlarge the window of detection for DENV [12, 13], WNV [14, 15] and ZIKV [9–11, 25] after the acute phase. CHIKV was detected in urine of experimentally infected mice at day 30 post infection, after CHIKV clearance in blood [29]. In our study, the two urines samples testing positive for CHIKV were collected during the 1st week PSO and all samples collected after tested negative.
Conclusions
According to our results, saliva cannot replace blood for molecular detection of CHIKV. Saliva specimen can be used only during the 1st week PSO if blood is impossible to collect and with the restriction that the sensitivity is low. In contrast to DENV, WNV and ZIKV, urine does not enlarge the window of detection of CHIKV RNA. If saliva and urine are of great interest for the detection of ZIKV RNA, blood remains the sample of choice for CHIKV, DENV and WNV RNA detection.
These results should be confirmed on a larger study.
Abbreviations
CHKV, chikungunya virus; DENV, dengue virus; FP, French Polynesia; Ig, Immunoglobulin; PSO, Post symptoms onset; RT-PCR, reverse transcription-Polymerase chain reaction; WNV, West Nile virus; ZIKV, Zika virus.
References
Cao-Lormeau VM, Musso D. Emerging arboviruses in the pacific. Lancet. 2014;384:1571–2.
Laigret J, Rosen L, Scholammer G. On an epidemic of dengue occurring in Tahiti in 1964. Relations to the “hemorrhagic fevers” of southeast Asia. Bull Soc Pathol Exot Filiales. 1967;60:339–53.
Musso D, Nilles EJ, Cao-Lormeau VM. Rapid spread of emerging zika virus in the pacific area. Clin Microbiol Infect. 2014;20:O595–6.
Musso D, Cao-Lormeau VM, Gubler DJ. Zika virus: following the path of dengue and chikungunya? Lancet. 2015;386:243–4.
Powers AM, Brault AC, Shirako Y, Strauss EG, Kang W, Strauss JH, et al. Evolutionary relationships and systematics of the alphaviruses. J Virol. 2001;75:10118–31.
Nhan T, Musso D. The burden of chikungunya in the pacific. Clin Microbiol Infect. 2015;21:e47–8.
Aubry M, Teissier A, Roche C, Richard V, Shan Yan A, Zisou K, et al. Chikungunya outbreak, French Polynesia, October 2014. Emerg Infect Dis. 2015;21:724–6.
Musso D, Roche C, Nhan TX, Robin E, Teissier A, Cao-Lormeau VM. Detection of zika virus in saliva. J Clin Virol. 2015;68:53–5.
Gourinat AC, O’Connor O, Calvez E, Goarant C, Dupont-Rouzeyrol M. Detection of zika virus in urine. Emerg Infect Dis. 2015;21:84–6.
Musso D, Roche C, Robin E, Nhan T, Teissier A, Cao-Lormeau VM. Potenial sexual transmission of zika virus. Emerg Infect Dis. 2015;21:359–61.
Besnard M, Lastère S, Teissier A, Cao-Lormeau V, Musso D. Evidence of perinatal transmission of zika virus. Euro Surveill. 2014;19:20751.
Mizuno Y, Kotaki A, Harada F, Tajima S, Kurane I, Takasaki T. Confirmation of dengue virus infection by detection of dengue virus type 1 genome in urine and saliva but not in plasma. Trans R Soc Trop Med Hyg. 2007;101:738–9.
Mardekian SK, Roberts AL. Diagnostic options and challenges for dengue and chikungunya Viruses. Biomed Res Int. 2015;2015. doi: 10.1155/2015/834371.
Tonry JH, Brown CB, Cropp CB, Co JKG, Bennett SN, Nerurkar VR, et al. West Nile virus detection in urine. Emerg Infect Dis. 2005;11:1294–6. Centers for Disease Control and Prevention.
Barzon L, Pacenti M, Franchin E, Pagni S, Martello T, Cattai M, et al. Excretion of west Nile virus in urine during acute infection. J Infect Dis. 2013;208:1086–92.
World Health Organisation. Guidelines on clinical management of chikungunya fever. 2008. available at: http://www.wpro.who.int/mvp/topics/ntd/Clinical_Mgnt_Chikungunya_WHO_SEARO.pdf. 5 June 2016.
European Centre for Disease Prevention and Control. Information for health practitioners. Eur Cent Dis Prev Control. 2007. Available at: http://ecdc.europa.eu/en/healthtopics/Documents/Chikungunya_Fever_Factsheet_for_Health_Practitioners.pdf. 5 June 2016.
Haute Autorité de la Santé. Diagnostic biologique direct précoce du chikungunya par détection génomique du virus avec RT-PCR. HAS. 2013;95. Available at: http://www.has-sante.fr/portail/upload/docs/application/pdf/2013-02/rapport_chikungunya_vd.pdf. 5 June 2016.
Pastorino B, Bessaud M, Grandadam M, Murri S, Tolou HJ, Peyrefitte CN. Development of a TaqMan RT-PCR assay without RNA extraction step for the detection and quantification of African chikungunya viruses. J Virol Methods. 2005;124:65–71.
Leung GHY, Baird RW, Druce J, Anstey NM. Zika virus infection in Australia following a monkey bite in Indonesia. Southeast Asian J Trop Med Public Heal. 2015;46:460–4.
Poloni TR, Oliveira AS, Alfonso HL, Galvão LR, Amarilla AA, Poloni DF, et al. Detection of dengue virus in saliva and urine by real time RT-PCR. Virol J. 2010;7: doi: 10.1186/1743–422X-7–22.
Gardner J, Rudd PA, Prow NA, Belarbi E, Roques P, Larcher T, et al. Infectious chikungunya virus in the saliva of mice monkeys and humans. PLoS One. 2015;10, e0139481.
Hirayama T, Mizuno Y, Takeshita N, Kotaki A, Tajima S, Omatsu T, et al. Detection of dengue virus genome in urine by real-time reverse transcriptase PCR: a laboratory diagnostic method useful after disappearance of the genome in serum. J Clin Microbiol. 2012;50:2047–52.
Kutsuna S, Kato Y, Takasaki T, Moi ML, Kotaki A, Uemeru H, et al. Two cases of Zika fever imported from French Polynesia to Japan, December 2013 to January 2014. Euro Surveill. 2014;19(4). pii:20683.
de Campos RM, Cirne-Santos C, Meira GLS, Santos LLR, de Meneses MD, Friedrich J, et al. Prolonged detection of zika virus RNA in urine samples during the ongoing zika virus epidemic in brazil. J Clin Virol. 2016;77:69–70.
Kondo M, Akachi S, Ando K, Nomura T, Yamanaka K, Mizutani H. Two Japanese siblings affected with Chikungunya fever with different clinical courses: Imported infections from the Cook Islands. J Dermatol. 2016; doi: 10.1111/1346-8138.13253.
Mathur A, Khanna N, Kulshreshtha R, Maitra SC, Chaturvedi UC. Viruria during acute Japanese encephalitis virus infection. Int J Exp Pathol. 1995;76:103–9.
Domingo C, Yactayo S, Agbenu E, Demanou M, Schulz AR, Daskalow K, et al. Detection of yellow fever 17D genome in urine. J Clin Microbiol. 2011;49:760–2.
Jones PH, Okeoma CM. Detection of Chikungunya virus (CHIKV) in urine of infected mice: a potential non-invasive diagnostic tool for CHIKV. J Infect Dis Ther. 2015;3: doi:10.4172/2332-0877.1000226.
Acknowledgments
We are grateful to the technical team of the medical analysis laboratory of Institut Louis Malardé for their contribution in performing the Zika virus molecular testing.
Authors’ contributions
DM, JJ DP and TX N researched the literature, and helped to the drafts manuscript. AT and ER performed analyses. ST performed sample collection. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Written consent was obtained from the patients / family for publication.
Ethics approval and consent to participate
The study has been approved by the Ethics Committee of French Polynesia (reference 61/CEPF).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Musso, D., Teissier, A., Rouault, E. et al. Detection of chikungunya virus in saliva and urine. Virol J 13, 102 (2016). https://doi.org/10.1186/s12985-016-0556-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12985-016-0556-9