
Abstract
DNA-damaging agents are commonly used for first-line chemotherapy of advanced non-small cell lung cancer (NSCLC). As a G2/M checkpoint kinase, Wee1 can phosphorylate CDC2-tyr15 and induce G2/M cell cycle arrest in response to DNA damage. The correlation of WEE1 polymorphisms to the efficacy of chemotherapy was tested in 663 advanced NSCLC patients. WEE1 rs3910384 genotype correlated to overall survival (OS) and progress-free survival (PFS) of NSCLC patients treated with platinum-based chemotherapy. Sub-group analysis revealed that rs3910384 was particularly associated with the efficacy of doublet chemotherapy combining two DNA-damaging agents, i.e. platinum and gemcitabine. NSCLC patients with the WEE1 rs3910384 G/G homozygote genotype showed 13.5 months extended OS, 3.2 months extended PFS and a 274% relative increase in their 3-year survival rate (from 7.4% to 27.7%) compared to the A/A+A/G genotype after treatment with platinum-gemcitabine regimen. This finding was reproduced in the validation cohort. We utilized a luciferase reporter assay and Electrophoretic Mobility Shift Assay (EMSA) to demonstrate that rs3910384-linked WEE1 promoter haplotype can mediate allele-specific transcriptional binding and WEE1 expression in DNA damage response. In conclusion, the WEE1 rs3910384 G/G homozygote genotype can be used as a selective biomarker for NSCLC patients to indicate treatment with platinum and gemcitabine regimen.
Similar content being viewed by others


Introduction
Lung cancer remains the most dangerous malignant disease, with the highest incidence and mortality throughout the world as well as in China1,2. Non-small-cell lung cancer (NSCLC) accounts for approximately 80% of lung cancer cases and most patients are diagnosed at an advanced stage3. Targeted therapy is already being used for the treatment of advanced NSCLC harboring EGFR mutations, EML4-ALK fusion, etc4. However, the patients with EGFR mutations only account for 10–35 percent of NSCLC patients and the frequency of EML4-ALK fusion patients is just 5–7 percent5, meaning that the remaining patients still need to rely on platinum-based chemotherapy. Although the platinum-based doublet chemotherapy is the most common first-line treatment for patients with advanced NSCLC, the efficacy of the chemotherapy regimen remains far from ideal and patients usually experience severe adverse effects. As a result, fewer than 35% of patients show a positive response to platinum-based chemotherapy and the 3-year survival rate is less than 10% in unselected NSCLC patients6.
DNA-damaging agents, such as platinum, gemcitabine and 5-fluorouracil (5-FU), are the primary chemotherapy drugs used to treat many cancers. These drugs cause cell cycle arrest by impeding DNA synthesis, replication and transcription, to eventually induce cancer cell apoptosis or mitotic catastrophe7,8. For lung cancer, platinum agents are indispensable in the standard chemotherapy doublet regimens. Evidence-based clinical practice shows that two-drug combinations are an optimal chemotherapy regimen for the treatment of advanced NSCLC. The combinations of cisplatin or carboplatin with either one of the DNA-damaging agents (gemcitabine), tubulin-targeting drugs (paclitaxel, docetaxel, or vinorelbine), or DNA topoisomerase II inhibitors (VP-16), show almost similar response rates and survival time for unselected NSCLC9. Therefore, clinically applicable biomarkers for prediction of the efficacy of combination chemotherapy are urgently needed for personalized chemotherapy treatment of NSCLC.
Wee1, a crucial kinase of cell cycle progression, regulates the G2 checkpoint arrest in response to DNA damage. Wee1 can phosphorylate CDC2 (CDK1) on Tyr15, inactivating the CDC2-cyclin B complex to inhibit cell cycle progression from G2 into M phase10. DNA damage checkpoints can induce a transient increase of WEE1 expression to cause G2-arrest for premitotic DNA repair11. Wee1-induced G2-arrest plays a critical role in the sensitivity of DNA-damaging agents and/or radiation therapy12. The combination of DNA-damaging drugs or radiation therapy with WEE1 kinase inhibitors has shown therapeutic benefit14. In this study, we find that WEE1 polymorphism is strongly associated with the treatment efficacy of DNA-damaging agents in patients with advanced NSCLC and can be used as a valuable biomarker for predictions of efficacy followed by a platinum-gemcitabine regimen.
Materials and Methods
Ethics Statement
The study was approved by the Medical Ethics Committee of the Shanghai Chest Hospital, Shanghai Zhongshan Hospital, Shanghai Changhai Hospital and Shanghai Pulmonary Hospital. Written informed consent was obtained from all patients who participated in this study. In addition, the experiments in this study were conducted in accordance with approved guidelines and regulations.
Study subjects
The test cohort included 663 patients who had been diagnosed with either clinical stage IIIA or IV NSCLC and had received first-line platinum-based chemotherapy (no prior surgery, radiotherapy, or concurrent chemoradiotherapy) between March 2005 and January 2010. The association of the WEE1 tag SNP with the efficacy of chemotheraputic regimens was reviewed and evaluated. The validation cohort included 264 NSCLC patients who accepted the platinum-gemicitabine regimen in Shanghai Pulmonary Hospital between June 2010 and May 2013. All the patients had histologically confirmed NSCLC with the presence of at least one measurable and evaluable lesion. Eastern Cooperative Oncology Group performance status (ECOG PS) for the patients is 0–2 and the cardiovascular, hepatic, hematologic and renal functions of the patients have been reviewed to assess chemotherapy tolerance.
Treatment
All patients in the test cohort underwent first-line platinum-based chemotherapy for 2 to 6 cycles with one of the following chemotherapy doublet regimens: (1) DNA-damaging agents regimen: either cisplatin 75 mg/m2 or carboplatin AUC 5 administered on day 1 every 3 weeks, in combination with gemcitabine 1250 mg/m2 on days 1 and 8 every 3 weeks, (2) tubulin-targeting drugs regimens: Either cisplatin 75 mg/m2 or carboplatin AUC 5 administered on day 1 every 3 weeks, in combination with navelbine 25 mg/m2 on days 1 and 8 every 3 weeks, or paclitaxel 175 mg/m2 on day 1 every 3 weeks, or docetaxel 75 mg/m2 on day 1 every 3 weeks, (3) other combination: Either cisplatin 75 mg/m2 or carboplatin AUC 5 administered on day 1 every 3 weeks, in combination with etoposide or bevacizumab. For the patients in validation cohort, either cisplatin 75 mg/m2 or carboplatin AUC 5 was administered on day 1 every 3 weeks, in combination with gemcitabine 1250 mg/m2 on days 1 and 8.
Tumor response
According to the Response Evaluation Criteria in Solid Tumors (RECIST), the short-term responses to chemotherapy treatment were evaluated after the first 2 cycles. The disease control rate (DCR) included complete response (CR), partial response (RR) and stable disease (SD). The objective response rate (ORR) consisted of complete response (CR) and partial response (PR). The progression-free survival (PFS) was assessed as the date from the chemotherapy treatment to objective disease progression or death (whichever occurred first) or the last progression-free follow-up. The overall survival (OS) was defined as the first day to receive chemotherapy treatment to the day of death or to the final follow-up.
WEE1 tag SNPs genotyping and Linkage Disequilibrium Analysis
The four tag SNPs (rs3829254, rs3910384, rs4370932 and rs1049403) representing 50 SNPs of WEE1 were selected from the CHB data of the phase 2 HapMap SNP database (http://www.hapmap.org/) using a minor allele frequency (MAF) cutoff of 0.05 and a correlation coefficient (r2) threshold of 0.8. Genomic DNA was extracted from patients’ peripheral blood samples using the QIAamp DNA Maxi Kit (Qiagen GmbH, Hilden, Germany) according to the manufacturer’s instructions. The SNPs were genotyped using the iSelect HD Bead-Chip (Illumina, San Diego, CA, USA) with the following quality-control criteria: genotyping call rate >0.95; MAF >0.05; and GenCall score >0.2. The concordance among replicates was >99.9% and the GeneMap software was used to analyze the data and prepare reports.
Linkage disequilibrium was analyzed in Haploview Software (Broad Institute of Harvard and Massachusetts Institute of Technology, Cambridge, MA, USA). Three putative functional SNPs, i.e. rs6486433, rs3763869 and rs3763868 in the WEE1 promoter region which are closely linked with rs3910384 were selected using MAF >0.2 and D’ >0.8 cutoff. The function of SNPs was predicted with FuncPred tools (National Institute of Environmental Health Sciences, USA). Individual haplotype frequencies for the selected SNPs were evaluated using the Hyploview or PHASE 2.0 Program (version 2.0.2) based on the Bayesian algorithm.
Construction of PGL4 WEE1 luciferase reporter plasmids and luciferase reporter Assay
Genomic DNA was extracted from the peripheral blood lymphocytes of patients. The WEE1 haplotype promoter region (650 bp;−24 bp ∼+626 bp) containing the 3 putative functional SNPs was PCR-cloned into PGL4 luciferase reporter plasmid. Forward primer: 5’-CACGGTACCAGCCAGTGTCCAGCCTAAGCA-3’ (Kpn I); Reverse primer: 5’-CTAACGCGTAGGTCTCCTCAGGTCCAGTCTCA-3’ (Mlu I). The PCR reaction was carried out at 95 °C, 3 minutes followed by 35 cycles (95 °C 30 s, 68 °C 30 s, 72 °C 30 s) and an extension period of 5 minutes at 72°C. PCR products were ran on an agarose gel and purified from the bands (MiniBEST Agarose Gel DNA Extraction Kit, TaKaRa, China), ligated and transformed into DH5α. PGL4 WEE1 luciferase reporter plasmids containing two major promoter haplotypes, i.e. rs3910384 “A” allele-linked G/A/C (rs6486433/rs3763869/rs3763868) (termed “haplotype 1”) or rs3910384 “G” allele-linked T/G/G (rs6486433/rs3763869/rs3763868) (termed “haplotype 2”) were obtained by sequencing of the selected single clones.
The PGL4 WEE1 luciferase reporter and TK plasmid (DNA dosage PGL-4: TK = 9:1) were co-transfected into A549 or H1299 (human lung adenocarcinoma) cell lines using Lipo FiterTM liposomal Transfection regent (Hanbio, China). After the indicated time, the cells were lysed and relative luciferase units (RLU) were measured using the dual-luciferase reporter assay system (Promega, WI, USA) according to the manufacturer’s instructions. To determine the WEE1 RLU after DNA damaging agents treatment, the transfected cells were subjected to 8 μg/mL cisplatin (DDP) or 40 μg/mL gemcitabine (GEM) for two hours and RLU was measured at 12, 24 and 36 hours after drug removal. Each assay was repeated at least three times.
Electrophoretic Mobility Shift Assay
Nuclear extracts of lung cancer cell lines H1299 and A549 were prepared using the method described by Edmead et al15. The sequences of the biotin-labeled double-stranded oligonucleotide probes of rs6486433, rs3763869 and rs3763868 are listed in Table S1. EMSA was carried out according to the manufacturer’s protocol (EMSA Kit ES009, Beyotime, China). Briefly, 10 μg nuclear extract were incubated in 20 μl binding reaction buffer (10 mM Tris-HCl, pH7.5, 50 mM KCl, 1 mM DTT, 10% glycerol) with the 2.5 nM biotin-labeled probe and 0.5 μg poly dI:dC (Sigma) for 30 min at room temperature. DNA–protein complexes were subjected to electrophoresis on 5% polyacrylamide gel, transferred to nylon membrane and visualized by chemiluminescence imaging.
Statistical analysis
All statistical analyses were accomplished using SPSS® version 20.0 (SPSS Inc., Chicago, IL, USA). The association between OS or PFS of the NSCLC patients and the tag SNPs was evaluated by the Kaplan-Meier curves and verified by log-rank tests. Univariate and multivariate analyses were executed utilizing the Cox proportional hazard model to validate the significant factors related to the OS or PFS. Variables yielding P-values < 0.05 in the univariate analyses were used for the multivariate analyses, including gender (female vs. male), smoking status (ever vs. never), clinical stage (TNM IV vs. IIIb vs. IIIa), histology (adenocarcinoma, squamous, adenosquamous or others), the rs3910384 dominant model, the rs3829254 recessive model and the rs4370932 additive model. For the dominant, recessive and additive models of each SNP, the model with the smallest P-value in univariate analyses was used for multivariate analyses. The relationship between the significant SNPs and the clinical characteristics was determined using χ2 test. All statistical analyses were two-sided and the differences were considered as statistically significant at P < 0.05.
Results
Patients’ characteristics and genotype information
The details of the patients’ characteristics in the test cohort are listed in Table S2. All 663 patients were treated with first-line platinum-based doublet chemotherapy in this study. Among them, 152 patients received the platinum-DNA damaging drug combination regimen (gemcitabine), 472 patients received the platinum-tubulin-targeting drug combination regimen (paclitaxel, docetaxel or navelbine) and the rest received the other combination regimen, i.e. etoposide or bevacizumab. The patient population consisted of 465 males and 198 females with a median age of 58 years. The tumors were classified histologically as 64.9% adenocarcinomas, 21.3% squamous carcinomas, 2% adenosquamous carcinomas and 11.9% other histological types.
The genotype frequencies of the four WEE1 tag SNPs in current data, or in CHB (Han Chinese in Beijing, China), CEU (Utah residents with Northern and Western European ancestry from the CEPH collection) and YRI (Yoruban in Ibadan, Nigeria) from the HapMap (HapMap Genome Browser release #28; Phases 1, 2 & 3 - merged genotypes & frequencies) SNP database are shown in Table S3. No difference in allele frequency was found between the current data and CHB. Different rs3829254, rs3910384, rs4370932, rs1049403 allele frequencies were observed among the Chinese, Western and African population. The Rs3910384 MAF for Chinese, Western and African populations were 0.401 (A), 0.411 (G) and 0.417 (A), respectively.
WEE1 rs3910384 genotype is correlated with the efficacy of platinum-based chemotherapy
The association of patients’ characteristics and WEE1 polymorphisms with overall survival was explored by univariate Cox’s regression analysis in all 663 patients treated with platinum-based doublet chemotherapy (Table 1). The 4 WEE1 tag SNPs were classified by models including genotypic, dominant, recessive, or additive. Gender, smoking history, clinical stage and histology were significantly associated with OS but no correlation was found with age, ECOG PS, or chemotherapy regimens. Using WEE1 genotypes as categorical variables, only rs3910384 in the 4 tag SNPs presented a statistically significant association with OS (p = 0.022). The dominant model of rs3910384 (p = 0.006), recessive model of rs3829254 (p = 0.022) and additive model of rs3910384 (p = 0.009), rs3829254 (p = 0.023), or rs4370932 (p = 0.028) showed statistically significant association. Furthermore, we included gender, smoking, clinical stage, histology, the rs3910384 dominant model, the rs3829254 recessive model and the rs4370932 additive model in the multivariate Cox’s regression analysis. The results suggested that clinical stage (p = 8.0E-3), histology (p = 4.3E-4) and the rs3910384 dominant model (p = 4.0E-3) were independent predictive factors for OS (Table 2).Patients with the rs3910384 G/G genotype (mOS, 20.4; 95%CI, 17.6–23.2) had higher median OS (mOS) than A/G+A/A (mOS, 16.9; 95%CI, 15.1–18.7; p = 4.0E-3) in all 663 patients treated with platinum-based doublet regimens. The Kaplan-Meier curves of OS according to polymorphisms of the WEE1 tag SNPs are shown in Fig. 1 & S1. (Fig. 1A for rs3910384; Figure S1A, B & C for other tag SNPs; Table S9).

Kaplan-Meier overall survival curves of NSCLC patients with various rs3910384 genotypes treated with standard chemotherapy doublet regimens
A: Overall survival for all the patients. B: Overall survival for patients treated with platinum-gemcitabine regimen. C: Overall survival for patients treated with platinum-tubulin-targeting drugs regimen. D: Overall survival for patients treated with other combination regimens.
The WEE1 rs3910384 dominant model (adjusted HR, 0.68; 95% CI, 0.55–0.84; p = 3.2E-4), as well as ECOG PS (adjusted HR, 1.49; 95% CI, 1.09–2.05; p = 0.012) were also found to be independent factors for the progression free survival (PFS) of all the enrolled NSCLC patients by univariate and multivariate Cox’s regression analysis (Table S4, Fig. 2A for rs3910384, Figure S2A, B & C for other tag SNPs).

Kaplan-Meier progression free survival curves of NSCLC patients with variousrs 3910384 genotypes treated with standard chemotherapy doublet regimens
A: Progression free survival for all the patients. B: Progression free survival for patients treated with platinum-gemcitabine regimen. C: Progression free survival for patients treated with platinum-tubulin-targeting drugs regimen. D: Progression free survival for patients treated with other combination regimens.
WEE1 rs3910384 genotype predominantly contributes to the efficacy of platinum-gemcitabine regimen
To better define the contribution of WEE1 rs3910384 to the efficacy of platinum-based chemotherapy, we performed a subgroup analysis stratified on different standard chemotherapy regimens and found that the rs3910384 genotype predominantly contributed towards the efficiency of platinum-gemcitabine regimen, which consists of two DNA- damaging agents, but contributed little to the efficacy of the other doublet regimens (tubulin-targeting agents or DNA topoisomerase inhibitors) used in the study (Fig. 1B–D; Table S5). The patients with WEE1 rs3910384 G/G homozygote gained 32.2% (from 22.1% to 54.3%), 24.1% (from 14.7% to 38.8%) or 20.3% (from 7.4% to 27.7%) absolute increase in 1-, 2- and 3-year-survival rates, respectively, compared to the A/A+A/G genotype (p = 3.5E-4) (Table S6). Subgroup multivariate Cox regression analysis revealed that WEE1 rs3910384 dominate model and histology are independent factors for the OS of the 152 patients who received platinum-gemcitabine regimen (Table 3). The patients with G/G homozygote (mOS, 28.2; 95%CI, 20.5–35.9) had 13.5 months longer OS than A/A+A/G genotype (median OS, 14.7; 95%CI, 12.8–16.6; p = 6.9E-5). Adenocarcinoma patients were more sensitive than the squamous carcinoma, adenosquamous carcinoma, or other histological types when treated with platinum-gemcitabine regimen (p = 0.037). When evaluated with PFS as endpoint, a similar association in platinum-gemcitabine group was also observed, but not in the other platinum-based combination regimens (Fig. 2, Table S7).
For short-term response, NSCLC patients with the rs3910384 G/G genotype exhibited a higher disease control rate (DCR) following platinum-gemcitabine doublet treatment compared to A/A+A/G genotype patients with a marginal statistical significance (p = 0.058) (Table 4).
The results suggest that WEE1 rs3910384 G/G genotype as a potential biomarker to predict the chemotherapeutic efficacy for the platinum-gemcitabine regimen of DNA-damaging agents and is valuable for personalized chemotherapy for advanced NSCLC patients.
Validation of WEE1 rs3910384 G/G to predict the efficacy of platinum-gemcitabine chemotherapy
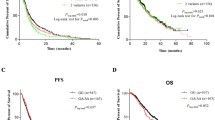
To validate the association of WEE1 rs3910384 G/G with the efficacy of DNA-damaging agents, 264 patients with advanced NSCLC who received platinum-gemcitabine chemotherapy were subjected to WEE1 rs3829254, rs3910384, rs4370932 and rs1049403 genotyping. The Kaplan-Meier analysis showed that WEE1 rs3910384 was still significantly correlated with OS in the 264 patients (p = 0.018) rather than the other three tagSNPs, rs3829254, rs4370932 and rs1049403 (Fig. 3). Multivariant Cox regression analysis also suggested that WEE1 rs3910384 dominate model was an independent factor for OS (p = 3.9E-4), which were consistent with findings in the test cohort (Table S8).

Validation of WEE1 tag SNPs polymorphisms associated with the efficacy of DNA-damaging agents in 264 patients with advanced NSCLC
A: Kaplan-Meier curve of OS for rs3910384 in patients with NSCLC. B: Kaplan-Meier curve of OS for rs3829254 in patients with NSCLC. C: Kaplan-Meier curve of OS for r4370932 in patients with NSCLC. D: Kaplan-Meier curve of OS for 1049403 in patients with NSCLC.
Rs3910384 is closely linked with WEE1 haplotype promoter with putative functional SNPs which can regulate WEE1 transcription in DNA damage response
In an analysis of linkage disequilibrium using the data from Hapmap database, WEE1 rs3910384 was found to be closely linked with the putative functional WEE1 promoter at SNPs rs6486433, rs3763869 and rs3763868 (Fig. 4A). All 3 putative functional SNPs are located at the allele-specific transcriptional binding sites of the WEE1 promoter region. The two major haplotypes of linked rs6486433/rs3763869/rs3763868/rs3910384 were G/A/C/A (44.8%) and T/G/G/G (43.4%) with the other haplotypes G/A/C/G (3.8%), G/G/G/G (3.0%) and T/G/G/A (1.6%) accounting for a small proportion of the total population (Fig. 4B). Thus the WEE1 rs3910384 “A” allele is strongly linked to the putative functional rs6486433/rs3763869/rs3763868 (G/A/C) WEE1 promoter and the rs3910384 “G” allele is strongly linked to rs6486433/rs3763869/rs3763868 (T/G/G).

The allele-specific transcription regulation of WEE1 in NSCLC cell lines in DNA damage response by cisplatin and gemcitabine
A: Linkage disequilibrium analysis of WEE1 rs3910384 and putative functional SNPs in WEE1 promoter region. B: WEE1 promoter haplotypes containing the indicated putative functional SNPs. C: Dual luciferase reporter assay of WEE1 haplotype promoters in A549 and H1299 cells following treatment with cisplatin or gemcitabine (*p < 0.05: repeated measures ANOVA; p < 0.05: t-test). D: EMSA for the 3 rs3910384-linked putative functional SNPs in WEE1 promoter region.(F: free probe; N: nuclear extraction plus the indicated probe. Red frame indicates the emerged bands in contrast to the counterpart allele).
Lower expression or functional loss of WEE1 leads to higher sensitivity toward DNA-damaging agents16,17. Using the PGL4 WEE1 haplotype promoter luciferase reporter assay, we confirmed that WEE1 haplotype promoters can mediate allele-specific transcription of WEE1 in lung cancer cell lines H1299 and A549 after treatment with the DNA-damaging chemotherapy agents cisplatin and gemcitabine (Fig. 4C). The WEE1 promoter haplotype 2 with rs3910384 “G” allele-linked T/G/G (rs6486433/rs3763869/rs3763868) had lower RLU (relative luciferase activity) than the WEE1 promoter haplotype 1 with rs3910384 “A” allele-linked G/A/C (rs6486433/rs3763869/rs3763868) at baseline levels in both A549 and H1299 cells (p < 0.05). Following DNA damage induced by cisplatin, gemcitabine, or the combination, the WEE1 promoter haplotype 2 showed a much lower increase of RLU compared to the WEE1 promoter haplotype 1 in A549 and H1299 lung cancer cell lines (p < 0.05). The results demonstrated that the WEE1 promoter strength is weaker in haplotype 2 and stronger in haplotype 1 in the transcription and de novo synthesis of WEE1 induced by the DNA damage response. The higher WEE1 expression driven by promoter haplotype 1 (rs3910384 “A” allele-linked G/A/C) can result in resistance towards the DNA-damaging agents and the lower WEE1 expression driven by promoter haplotype 2 (rs3910384 “G” allele-linked T/G/G) can result in sensitivity to DNA-damaging agents.
To examine the binding of SNP allele-specific transcriptional factors to Wee1 promoter haplotypes, we synthesized biotin-labeled probe pairs with the reference and allele genotypes of rs6486433, rs3763869, or rs3763868 and performed an electrophoretic mobility shift assay (EMSA) with the nuclear extract of A549 and H1299 cell lines. The results demonstrated that the probes with the “T” allele of rs6486433 and the “A” allele of rs3763869 yielded additional shift bands by contrast to the “G” allele of rs6486433 and “G” allele of rs3763869, respectively. This suggests that rs6486433 and rs3763869 in the WEE1 promoter region can mediate allele-specific transcriptional factor binding in vitro, which is the molecular basis for the differential transcriptional strength of WEE1 promoter haplotypes (Fig. 4D).
Discussion
DNA-damaging agents are the most commonly used anti-cancer drugs for the treatment of NSCLC patients. In cancer cells, DNA damage and repair pathway activation plays a critical role in the sensitivity of DNA-damaging agents18. Numerous studies have revealed that DNA damage response pathways can activate cell cycle checkpoints to arrest the cell either temporarily or permanently (senescence). It is well established that p53 is responsible for G1 checkpoint regulation19 and that WEE1 tyrosine kinase is the major regulator for the G2 checkpoint20. The majority of tumors in NSCLC patients are found to be p53-mutated or p53-deficient and rely only on the WEE1 G2 checkpoint for cell cycle arrest after treatment with DNA-damaging agents. Although WEE1 somatic variation is seldom present in NSCLC, we find that germline variation in WEE1 has great impact on the efficacy of DNA-damaging agents in the treatment of advanced NSCLC.
DNA-damaging drugs will induce G1- or G2-arrest for the DNA repair process, which is a major determinant of the sensitivity towards cisplatin21. Abrogation of cell cycle arrest will force cells into mitosis with unrepaired DNA and eventually lead to apoptosis or mitotic catastrophe22,23. Nurse et al. first demonstrated that WEE1 is involved in the regulation of G2 checkpoints24 while Rowley et al. found that Schizosaccharomyces pombe strains with defective or abolished WEE1 function failed to arrest cells in G2 following treatment with cisplatin and were hypersensitive to cisplatin treatment25. Expression of WEE1 delays the mitotic entry of cells with radiation-induced DNA damage and the lengthening of the G2 phase depends on the expression of WEE126. Inhibition of WEE1 by siRNA, small molecule inhibitors, or other proteins exposed human cancer cells to DNA-damaging agents, resulting in abrogation of the G2 arrest, premature termination of DNA repair and cell death, leading to increased sensitivity towards DNA-damaging agents in different types of carcinomas27,28,29. To the best of our knowledge, the current study demonstrates for the first time that WEE1 kinase rs3910384 “G/G” allele is strongly associated with the therapeutic efficacy of platinum-gemcitabine doublet regimen, consisting of both DNA-damaging agents.
According to the NCCN (National Comprehensive Cancer Network) guidelines, platinum-based doublet chemotherapy is the most common first-line treatment for patients with advanced NSCLC30. At present, choosing a drug combination for NSCLC chemotherapy is equivocal because all of the combinations provide almost similar efficacy; a physician’s selection of a particular chemotherapy regimen depends on the patient’s tolerance for the adverse side effects, not the efficacy of the regimen. Platinum-based chemotherapy provides a slightly longer OS of only 1.5 months (from 4.5 months to 6 months) and a 9% absolute increase of 1-year-survival (from 20% to 29%) than the best supportive care in unselected NSCLC patients31. Our data indicate that WEE1 rs3910384 G/G can be used as a predictive biomarker for platinum-gemcitabine regimen with the benefit of 13.5 months longer median OS, 144% relative increase in 1-year survival rate (from 22.1% to 54.3%), 163% relative increase in 2-year survival rate (from 14.7% to 38.8%) and 274% relative increase in 3-year survival rate (from 7.4% to 27.7%) following treatment with platinum-gemcitabine regimen. The validation in the other 264 patients also shows that WEE1 rs3910384 is significantly associated with the efficacy of platinum-gemcitabine regimen. WEE1 rs3910384 G/G genotype accounts for 33.6% in Chinese, 13.4% in Western and 17.5% in African patients (Table S3). We postulate that WEE1 rs3910384 G/G is a potential biomarker for indicating the platinum-gemcitabine regimen in Chinese NSCLC patients. Whether it can be used as a biomarker in other populations needs to be further validated.
Among the four WEE1 tag SNPs we examined, rs3910384 is near the WEE1 core promoter. Although the direct function of rs3910384 is still unknown, linkage disequilibrium analysis demonstrated that rs3910384 was closely linked with the 3 predicted regulatory SNPs rs6486433 (D’ = 0.91), rs3763868 (D’ = 0.88) and rs3763869 (D’ = 0.89) within the transcription-factor-binding sites of the WEE1 promoter. The MAF of rs6486433 (MAF = 0.462), rs3763868 (MAF = 0.499) and rs3763869 (MAF = 0.493) are also similar to rs3910384 (0.486) in the HapMap population. Nearly ninety percent of the patients harbor one of the two major haplotypes of the WEE1 promoter, i.e. rs3910384 “G” allele-linked T/G/G (rs6486433/rs3763869/rs3763868, 43.4%) or rs3910384 “A” allele-linked G/A/C (44.8%). After cloning the two major WEE1 haplotype promoters into PGL4 luciferase reporter plasmids, we confirmed the allele-specific transcription regulation of WEE1 expression in A549 and H1299 cells after treatment with DNA-damaging chemotherapy agents. The WEE1 haplotype promoter with rs3910384 “A” allele-linked G/A/C can drive much higher RLU than the counterpart with rs3910384 “G” allele-linked T/G/G after DNA damage induced by cisplatin, gemcitabine, or a combination. According to SNPINFO website (http://snpinfo.niehs.nih.gov/snpinfo/snpfunc.htm), the WEE1 promoter allele-specific TFBS (transcription factor binding sites) include C/EBP, ETS, or SPZ1 for rs3763869, MAZ for rs3763868 and C/EBP, ETS, GCNF, or HNF4α for rs6486433. To validate the allele-specific transcription factor binding in the WEE1 promoter, we performed EMSA using nuclear extracts from lung cancer cell lines H1299 and A549 and found that rs6486433 and rs3763869, but not rs3763868, can mediate allele-specific transcription factor binding in vitro. The exact mechanism of the WEE1 promoter allele-specific transcription factors and its regulation of WEE1 expression needs to be further studied in detail.
As reported, Wee1 kinase is a gatekeeper molecule and regulates the G2-cell-cycle checkpoint arrest for pre-mitotic DNA repair27. Wee1-induced G2-arrest plays a critical role in sensitivity to DNA-damaging agents or radiation12,32. The Wee1 concentration in human cells is highly regulated during the cell cycle. Wee1 total protein (mRNA) is synthesized de novo at S and G2 phases, then phosphorylated, ubiquitinated and eliminated through proteasome-dependent degradation during M phase33,34,35. The activity of Wee1 increases during S and G2 phases in parallel with the increase in the protein level36. Wee1 protein is significantly increased and induces G2 arrest following DNA damage by drugs or radiation11. Although Wee1 expression can be regulated in many ways, the de novo synthesis of Wee1 is the major event that occurs as a response to DNA damage. The discrepancy of the strength of the WEE1 promoter haplotypes determines the level of Wee1 expression in the DNA damage response. This SNP allele-specific transcription of Wee1 provides the molecular explanation for the association of rs3910384 “G” allele with the increased sensitivity to DNA-damaging drugs.
Several efficacy-predicting biomarkers for chemotherapy in lung cancer patients have been reported. ERCC1 for platinum37,38, RRM1 for gemcitabine39,40 and TUBB3 for paclitaxel41 have been investigated in preclinical and/or in clinical studies involving small numbers of patients; however, their predictive roles are still debated. Crucially, these biomarkers cannot be validated in other studies or in multicenter clinical trials42,43,44, possibly due to either the instability of the mRNA or protein expression or unreproducible quantitative methods. Detection of germline or somatic mutations can provide highly reproducible results and is more suitable as a biomarker in clinical practice. WEE1 rs3910384 G/G genotype detection can be a valuable biomarker for the platinum-gemcitabine chemotherapy regimen.
Currently, WEE1 inhibitors MK-1775 and PD-166285 are being tested in preclinical and clinical studies of human carcinoma14,45. Synergy between WEE1 inhibitors (MK-1775 or PD-166285) and DNA-damaging agents has been reported14,46,47. MK-1775 achieved favorable phase I pharmacokinetic and pharmacodynamic endpoints in combination with carboplatin, cisplatin and gemcitabine and is under further investigation as a chemosensitizer in a phase II trial48. Our finding suggests that a population of NSCLC patients with WEE1 rs3910384 G/G genotype is much more sensitive to the platinum-gemcitabine chemotherapy regimen. This novel biomarker, the WEE1 rs3910384 G/G genotype, can provide 13.5 months longer overall survival and 374% relative increase (from 7.4% to 27.7%) of the 3-year-survival rate for advanced NSCLC patients treated with platinum-gemcitabine chemotherapy regimen. As such, it is a potential tool for deciding on combination chemotherapy options to facilitate personalized chemotherapy for NSCLC. However, this conclusion was derived from unselected NSCLC patients regardless of somatic variation of EGFR and ALK. For NSCLC patients without EGFR mutation or ALK rearrangement, platinum-based chemotherapy is still the first-line option of treatment. Determining whether the WEE1 rs3910384 G/G genotype can be used a biomarker for the option of platinum-gemcitabine regimen in NSCLC patients harboring no EGFR mutation and ALK rearrangement will better define this biomarker for the platinum-gemcitabine regimen and it is worth further validation in the future.
Additional Information
How to cite this article: Liu, D. et al. WEE1 kinase polymorphism as a predictive biomarker for efficacy of platinum-gemcitabine doublet chemotherapy in advanced non-small cell lung cancer patients. Sci. Rep. 5, 11114; doi: 10.1038/srep11114 (2015).
References
Jemal, A. et al. Global cancer statistics. CA Cancer J Clin 61, 69–90 (2011).
Chen, W. et al. Report of incidence and mortality in China cancer registries, 2009. Chin J Cancer Res 25, 10–21 (2013).
Ferlay, J. et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 127, 2893–2917 (2010).
Janku, F., Stewart, D. J. & Kurzrock, R. Targeted therapy in non-small-cell lung cancer–is it becoming a reality? Nat Rev Clin Oncol 7, 401–414 (2010).
Ma, P. C. Personalized targeted therapy in advanced non-small cell lung cancer. Cleve Clin J Med 79 Electronic Suppl 1, eS56–60 (2012).
Ozkaya, S., Findik, S., Dirican, A. & Atici, A. G. Long-term survival rates of patients with stage IIIB and IV non-small cell lung cancer treated with cisplatin plus vinorelbine or gemcitabine. Exp Ther Med 4, 1035–1038 (2012).
Boulikas, T. & Vougiouka, M. Cisplatin and platinum drugs at the molecular level. (Review). Oncol Rep 10, 1663–1682 (2003).
Plunkett, W. et al. Gemcitabine: metabolism, mechanisms of action and self-potentiation. Semin Oncol 22, 3–10 (1995).
Schiller, J. H. et al. Comparison of four chemotherapy regimens for advanced non-small-cell lung cancer. N Engl J Med 346, 92–98 (2002).
McGowan, C. H. & Russell, P. Cell cycle regulation of human WEE1. EMBO J 14, 2166–2175 (1995).
Raleigh, J. M. & O’Connell, M. J. The G(2) DNA damage checkpoint targets both Wee1 and Cdc25. J Cell Sci 113 (Pt 10) 1727–1736 (2000).
Wang, Y., Decker, S. J. & Sebolt-Leopold, J. Knockdown of Chk1, Wee1 and Myt1 by RNA interference abrogates G2 checkpoint and induces apoptosis. Cancer Biol Ther 3, 305–313 (2004).
PosthumaDeBoer, J. et al. WEE1 inhibition sensitizes osteosarcoma to radiotherapy. BMC Cancer 11, 156 (2011).
De Witt Hamer, P. C., Mir, S. E., Noske, D., Van Noorden, C. J. & Wurdinger, T. WEE1 kinase targeting combined with DNA-damaging cancer therapy catalyzes mitotic catastrophe. Clin Cancer Res 17, 4200–4207 (2011).
Edmead, C., Kanthou, C. & Benzakour, O. Thrombin activates transcription factors sp1, NF-kappaB and CREB: importance of the use of phosphatase inhibitors during nuclear protein extraction for the assessment of transcription factor DNA-binding activities. Anal Biochem 275, 180–186 (1999).
Hirai, H. et al. Small-molecule inhibition of Wee1 kinase by MK-1775 selectively sensitizes p53-deficient tumor cells to DNA-damaging agents. Mol Cancer Ther 8, 2992–3000 (2009).
Stathis, A. & Oza, A. Targeting Wee1-like protein kinase to treat cancer. Drug News Perspect 23, 425–429 (2010).
Cheung-Ong, K., Giaever, G. & Nislow, C. DNA-damaging agents in cancer chemotherapy: serendipity and chemical biology. Chem Biol 20, 648–659 (2013).
el-Deiry, W. S. et al. WAF1/CIP1 is induced in p53-mediated G1 arrest and apoptosis. Cancer Res 54, 1169–1174 (1994).
Masuda, H., Fong, C. S., Ohtsuki, C., Haraguchi, T. & Hiraoka, Y. Spatiotemporal regulations of Wee1 at the G2/M transition. Mol Biol Cell 22, 555–569 (2011).
Brozovic, A. et al. Cisplatin sensitivity is related to late DNA damage processing and checkpoint control rather than to the early DNA damage response. Mutat Res 670, 32–41 (2009).
Leijen, S., Beijnen, J. H. & Schellens, J. H. Abrogation of the G2 checkpoint by inhibition of Wee-1 kinase results in sensitization of p53-deficient tumor cells to DNA-damaging agents. Curr Clin Pharmacol 5, 186–191 (2010).
Al-Ejeh, F. et al. Harnessing the complexity of DNA-damage response pathways to improve cancer treatment outcomes. Oncogene 29, 6085–6098 (2010).
Russell, P. & Nurse, P. Negative regulation of mitosis by wee1+, a gene encoding a protein kinase homolog. Cell 49, 559–567 (1987).
Thiebaut, F., Enns, R. & Howell, S. B. Cisplatin sensitivity correlates with its ability to cause cell cycle arrest via a wee1 kinase-dependent pathway in Schizosaccharomyces pombe. J Cell Physiol 159, 506–514 (1994).
Rowley, R., Hudson, J. & Young, P. G. The wee1 protein kinase is required for radiation-induced mitotic delay. Nature 356, 353–355 (1992).
Mir, S. E. et al. In silico analysis of kinase expression identifies WEE1 as a gatekeeper against mitotic catastrophe in glioblastoma. Cancer Cell 18, 244–257 (2010).
Pouliot, L. M. et al. Cisplatin sensitivity mediated by WEE1 and CHK1 is mediated by miR-155 and the miR-15 family. Cancer Res 72, 5945–5955 (2012).
Wang, F. et al. Transcriptional repression of WEE1 by Kruppel-like factor 2 is involved in DNA damage-induced apoptosis. Oncogene 24, 3875–3885 (2005).
Ettinger, D. S. et al. Non-small cell lung cancer, version 2.2013. J Natl Compr Canc Netw 11, 645–653; quiz 653 (2013).
Non-Small Cell Lung Cancer Collaborative, G. Chemotherapy and supportive care versus supportive care alone for advanced non-small cell lung cancer. Cochrane Database Syst Rev12, CD007309,doi: 007310.001002/14651858.CD14007309.pub14651852. (2010).
Sarcar, B. et al. Targeting radiation-induced G(2) checkpoint activation with the Wee-1 inhibitor MK-1775 in glioblastoma cell lines. Mol Cancer Ther 10, 2405–2414 (2011).
O’Connell, M. J., Raleigh, J. M., Verkade, H. M. & Nurse, P. Chk1 is a wee1 kinase in the G2 DNA damage checkpoint inhibiting cdc2 by Y15 phosphorylation. The EMBO journal 16, 545–554 (1997).
Watanabe, N. et al. M-phase kinases induce phospho-dependent ubiquitination of somatic Wee1 by SCFbeta-TrCP. Proc Natl Acad Sci USA 101, 4419–4424 (2004).
Dai, Y. & Grant, S. New insights into checkpoint kinase 1 in the DNA damage response signaling network. Clin Cancer Res 16, 376–383 (2010).
Watanabe, N., Broome, M. & Hunter, T. Regulation of the human WEE1Hu CDK tyrosine 15-kinase during the cell cycle. EMBO J 14, 1878–1891 (1995).
Lord, R. V. et al. Low ERCC1 expression correlates with prolonged survival after cisplatin plus gemcitabine chemotherapy in non-small cell lung cancer. Clin Cancer Res 8, 2286–2291 (2002).
Tantraworasin, A. et al. The prognostic value of ERCC1 and RRM1 gene expression in completely resected non-small cell lung cancer: tumor recurrence and overall survival. Cancer Manag Res 5, 327–336 (2013).
Olaussen, K. A. et al. DNA repair by ERCC1 in non-small-cell lung cancer and cisplatin-based adjuvant chemotherapy. N Engl J Med 355, 983–991 (2006).
Zheng, Z. et al. DNA synthesis and repair genes RRM1 and ERCC1 in lung cancer. N Engl J Med 356, 800–808 (2007).
Zhang, H. L. et al. Association between class III beta-tubulin expression and response to paclitaxel/vinorebine-based chemotherapy for non-small cell lung cancer: a meta-analysis. Lung Cancer 77, 9–15 (2012).
Reiman, T. et al. Cross-validation study of class III beta-tubulin as a predictive marker for benefit from adjuvant chemotherapy in resected non-small-cell lung cancer: analysis of four randomized trials. Ann Oncol 23, 86–93 (2012).
Yamashita, F. et al. Prognostic value of EGFR mutation and ERCC1 in patients with non-small cell lung cancer undergoing platinum-based chemotherapy. PLoS One 8, e71356 (2013).
Bepler, G. et al. Randomized international phase III trial of ERCC1 and RRM1 expression-based chemotherapy versus gemcitabine/carboplatin in advanced non-small-cell lung cancer. J Clin Oncol 31, 2404–2412 (2013).
Guertin, A. D. et al. Preclinical evaluation of the WEE1 inhibitor MK-1775 as single-agent anticancer therapy. Mol Cancer Ther 12, 1442–1452 (2013).
Rajeshkumar, N. V. et al. MK-1775, a potent Wee1 inhibitor, synergizes with gemcitabine to achieve tumor regressions, selectively in p53-deficient pancreatic cancer xenografts. Clin Cancer Res 17, 2799–2806 (2011).
Indovina, P. et al. Abrogating G(2)/M checkpoint through WEE1 inhibition in combination with chemotherapy as a promising therapeutic approach for mesothelioma. Cancer Biol Ther 15, 380–388 (2014).
Guertin, A. D. et al. Unique functions of CHK1 and WEE1 underlie synergistic anti-tumor activity upon pharmacologic inhibition. Cancer Cell Int 12, 45 (2012).
Acknowledgements
This work was supported by the Science and Technology Commission of Shanghai Municipality (No. 12DZ2295107, No. 10411956100, No. 12NM0500800, No. 12ZR1426100, No. 09411960500, No. 10411967600, No. 2010Y094, No. 134119A3400) and Shanghai Health Bureau Foundation (No. 201440397).
Author information
Authors and Affiliations
Contributions
B.S., K.F. and J.Q. contributed study concept and design. D.L. and B.S. drafted the manuscript. D.L., C.W., Y.J., L.H. and H.Z. acquired and analyzed data. D.L. and C.C. contributed technical support.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Liu, D., Wu, C., Jiao, Y. et al. WEE1 kinase polymorphism as a predictive biomarker for efficacy of platinum-gemcitabine doublet chemotherapy in advanced non-small cell lung cancer patients. Sci Rep 5, 11114 (2015). https://doi.org/10.1038/srep11114
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep11114
- Springer Nature Limited
This article is cited by
-
An update of predictive biomarkers related to WEE1 inhibition in cancer therapy
Journal of Cancer Research and Clinical Oncology (2024)
-
Clinical-pharmacogenetic models for personalized cancer treatment: application to malignant mesothelioma
Scientific Reports (2017)