
Abstract
Chronic obstructive pulmonary disease (COPD) is the third leading cause of death and is associated with multiple medical and psychological comorbidities. Therefore, future strategies to improve COPD management and outcomes are needed for the betterment of patient care. Wearable technology interventions offer considerable promise in improving outcomes, but prior reviews fall short of assessing their role in the COPD population. In this systematic review and meta-analysis we searched ovid-MEDLINE, ovid-EMBASE, CINAHL, CENTRAL, and IEEE databases from inception to April 2023 to identify studies investigating wearable technology interventions in an adult COPD population with prespecified outcomes of interest including physical activity promotion, increasing exercise capacity, exacerbation detection, and quality-of-life. We identified 7396 studies, of which 37 were included in our review. Meta-analysis showed wearable technology interventions significantly increased: the mean daily step count (mean difference (MD) 850 (494–1205) steps/day) and the six-minute walk distance (MD 5.81 m (1.02–10.61 m). However, the impact was short-lived. Furthermore, wearable technology coupled with another facet (such as health coaching or pulmonary rehabilitation) had a greater impact that wearable technology alone. Wearable technology had little impact on quality-of-life measures and had mixed results for exacerbation avoidance and prediction. It is clear that wearable technology interventions may have the potential to form a core part of future COPD management plans, but further work is required to translate this into meaningful clinical benefit.
Similar content being viewed by others


Introduction
Chronic obstructive pulmonary disease (COPD) is the third leading cause of death worldwide and is characterised by poorly reversible airflow obstruction secondary to a significant exposure to noxious gases or particles, accompanied by respiratory symptoms1,2. Patients with COPD have an underlying chronic inflammatory state that contributes to multiple medical and psychological comorbidities. These comorbidities add to the individual burden of disease, contribute to frequent hospitalisations, and add to an ever-growing healthcare cost. Furthermore, the natural history of COPD is punctuated by exacerbations which accelerate lung decline, and lead to a decreased physical reserve, impaired quality of life and increased mortality3,4. Given the significant individual and global burden of COPD, there is an urgent need to find future strategies to improve COPD diagnosis, management, and outcomes to improve patient care and quality of life.
Wearable health technology can be defined as any electronic device that is worn close to or on the skin’s surface that detects and collects data with a means for retrieval. In recent years, the wearable health market has grown exponentially with an estimated market value of $29 billion in 2019, which is predicted to rise to nearly $ 200 billion by 20275,6. Over the last two decades there have been several advancements in the use of wearables in the COPD population. In the main the focus has been on physical activity improvement by the use of activity trackers (pedometers and accelerometers). Wearables, such as continuous pulse oximetry devices have also been studied for their role in COPD monitoring. However, the reliability, accuracy and utility of the devices are still debated and few have made it into mainstream use7.
There have been several previous systematic reviews investigating the role of step-counters in promoting the mean daily step count in a COPD population. Both Qui et al.8 (n = 15 studies) and Armstrong et al.9 (n = 12 studies) found that step counter use increased physical activity compared to controls (standardised mean difference (SMD) = 0.57 (95%CI 0.31–0.84) and 0.53 (0.29–0.77) respectively). However, both reviews may be biased by including studies that did not mandate gold-standard spirometric diagnostic criteria for COPD and were limited by only including studies investigating step counters. Han et al. only focused on studies that lasted at least 12 weeks (n = 9) and showed a significant increase in physical activity of ≥793 steps/day10. Finally, Reilly et al.11 recently reviewed interventions to promote physical activity as assessed by step-count in chronic airways disease, but did not split the results by different disease groups. Only Quiet al.8 looked at physical capacity as assessed by the six-minute walk distance (6MWD) and no prior studies have investigated the role of wearables on other measures of physical activity or capacity such as time spent at various intensity levels and muscle strength. Moreover, no prior reviews have looked at whether wearable devices impact patient quality of life using standardised questionnaires.
In terms of other aspects of COPD management, a prior review by Al Rajeh and Hurst looked at whether monitoring physical parameters can predict COPD exacerbations. This review (n = 16) included a mix of wearable technology but only looked at intermittent rather than continuous monitoring. While the data was heterogenous, the authors concluded that monitoring physiological variables does have the potential to detect exacerbations12. Recent advances in this field have not yet been subject to systematic review.
To date, reviews have only focused on the role of wearables in physical activity improvement in the COPD population. However, the management of COPD includes other facets, such as smoking cessation, exacerbation prevention and quality of life improvement. It is still not clear whether wearable devices benefit COPD patients in all facets of their care. We therefore aimed to conduct a systematic review and meta-analysis, using gold standard diagnostic criteria for COPD, to assess the impact of wearable technology interventions on physical activity promotion, exercise capacity, exacerbation detection, smoking cessation, home self-management, disease progression, and quality of life.
Results
Literature search
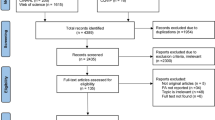
The initial search generated 7396 studies. After the removal of duplicates and screening of titles and abstracts, 96 studies were sought for retrieval, but one study could not be accessed, and the author was not reachable. Therefore, 95 studies were assessed in full for eligibility according to the inclusion criteria. An additional 58 papers were excluded following full-text review and a total of 37 studies met all the inclusion criteria. Figure 1 shows the PRISMA flow chart and a full list of the excluded studies at full-text review, with reasons, which can be seen in Supplementary Methods.

PRISMA flow chart for included studies.
A summary of the included studies is reported in Table 1. Thirty studies13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42 investigated the role of wearable technology (with or without other components) in improving physical activity outcomes (27 randomised controlled trials (RCTs)14,15,16,17,18,20,21,22,23,24,25,26,27,28,30,31,32,33,35,36,37,38,39,40,41,42 and three observational studies19,29,34). The studies included a total of 2955 patients, 69% male, with a median (IQR) sample size of 53 (32–143), mean (SD) age of 67 (6) years and a median (IQR) FEV1% predicted of 54 (45–59)%. For the RCTs the median (IQR) drop-out rate in the intervention group was 20% (10−29%), similar to 17% (10−28%) in the control group. Most RCTs used a per-protocol analysis (80%).
Physical activity and exercise capacity
The physical activity and exercise capacity metrics measured varied among studies (step counts, six-minute walk distance (6MWD), sedentary time, moderate-to-vigorous physical activity (MVPA) and quadricep strength). Meta-analysis showed that wearable technology interventions significantly increased the mean daily step count (21 studies15,16,17,18,20,21,22,23,24,27,28,30,31,32,33,36,37,38,39,40,41, 2025 participants, median (IQR) duration 3months (2.3−6 months)) with a standardised mean difference (SMD) of 0.42 (0.25–0.60), equating to a mean difference (95%CI) of 850 (494–1205) steps/day. This is illustrated in Fig. 2.

Meta-analysis results for mean daily step count reported.
Multivariable meta-regression analysis with year of publication, participant age, baseline FEV1 (% predicted), type of pedometer used in the intervention and outcome measurement device (type of pedometer or accelerometer) explained 21% of the heterogeneity but was non-significant (residual I2 = 57%, R2 = 21%, p = 0.61). The full model results can be seen in Supplementary Table 1.
Subgroup analysis showed that studies where wearable technology was combined with additional health coaching (e.g., motivational interviewing or counselling) had a higher mean difference compared to studies where wearable technology was the only intervention (MD 998 (539–1456) steps/day vs. 243 (−341 – 801) steps/day). Moreover, studies that were of shorter duration (≤3 months) and those that used pedometers to measure their outcome variable had a higher overall mean difference. This is illustrated in Table 2.
Meta-analysis showed that wearable technology interventions significantly increased the 6MWD (17 studies15,16,18,21,23,24,25,26,28,30,32,33,36,38,39,40,42, 1485 participants) with a mean difference (95%CI) of 5.81 m (1.02–10.61 m). This is illustrated in Fig. 3.

Meta-analysis results for the six-minute walk distance (m).
Subgroup analysis showed studies which were multi-component (wearable technology with health coaching) had a higher mean difference (11.75 m (3.93–19.56 m)). Studies of shorter duration (≤3 months) also had a higher mean difference compared to longer studies (10.13 m (3.97–16.30 m) vs. −0.80 m (−8.43 – 6.82 m)). (Table 2)
Wearable devices did not significantly impact sedentary time (4 studies16,17,22,41, 537 participants, SMD −0.07 (−0.24 −0.10)), MVPA time (7 studies16,17,21,22,31,36,41, 1010 participants, SMD 0.22 (−0.02–0.46)) and quadricep strength (5 studies16,21,23,26,36, 463 participants, SMD 0.15 (−0.03–0.33). The pooled effects of these can be seen in Supplementary Figs. 1 and 2. None of the observational studies19,29,34 found any difference in step count.
Quality of life measures
Secondary outcome measures in 24 studies15,16,17,18,20,21,22,23,24,25,26,27,28,29,30,31,32,33,35,36,37,39,40,42 looked at changes in quality-of-life measures using validated questionnaires. The median duration (IQR) of these studies was 5.4 months (2.9–6 months). The primary outcome of all these studies was to determine the impact of wearables on physical activity. Meta-analysis showed that wearables were associated with a significant reduction in the COPD Assessment Tool (CAT) score (11 studies15,16,18,21,22,25,27,28,35,36,40, 1306 participants, median duration 3 months (2.31–6 months) by a mean difference (95%CI) of −0.99 (−1.59 to −0.40). This is illustrated in Fig. 4.

Meta-analysis results for the COPD Assessment Tool score.
Subgroup analysis looking at study duration and type of intervention found no difference in the CAT score. (Table 2).
No significant differences were seen with the St George’s Respiratory Questionnaire (SGRQ) score (8 studies20,24,25,30,33,37,39,42, 469 participants, mean difference −1.73 (−4.90 to 1.44)); modified medical research council (mMRC) score (5 studies18,28,33,37,39, 418 participants, mean difference −0.10 (−0.30 to 0.11)). Two studies15,16 used the Clinical PROactive C-PPAC instrument that has previously been validated in COPD patients which requires both questionnaire and accelerometer data. Meta-analysis showed a significant improvement in the total score (mean difference 5.74 (1.85–9.62)). The pooled effects can be seen in Supplementary Figures 3-5.
COPD self-management
Two studies investigated the role of wearables in COPD self-management through different scoring systems. Benzo et al.17, showed that the wearable intervention significantly increased the self-management ability scale (SMAS) with a mean difference of 4.10 (1.68–6.52); while Park et al.32, showed no significant difference when using the self-efficacy for managing chronic diseases (SEMCD) score with a mean difference of −0.04 (−0.87–0.73).
COPD exacerbations
Ten studies15,32,33,43,44,45,46,47,48,49 investigated the role of wearable technology and COPD exacerbations. The studies included a total of 3660 patients, 69% male, a median (IQR) sample size of 78 (46–143), mean (SD) age of 69 (2) years and median (IQR) FEV1% predicted of 57 (53–61%). For the RCTs the median (IQR) drop-out rate in the intervention group was 36% (9–56%) and was 17% (4–30%) in the control group.
Five RCTs15,32,33,47,48 assessed the association of pedometers and the rate of exacerbations needing hospitalisation. Meta-analysis of four studies15,32,33,47 (median follow-up duration 9 months) found no significant difference in the risk of hospitalisation from a COPD exacerbation (pooled OR 1.06 (0.90–1.24), I2 = 31%). This meta-analysis was dominated by one large study47 and is shown in Fig. 5. Wan et al.48 found pedometer use significantly reduced the risk of any acute COPD exacerbation over 15 months with a rate ratio of 0.51 (0.31–0.85).

Meta-analysis investigating the association between wearable technology and COPD exacerbations.
It is worth noting that all four of these studies included multi-component interventions where wearable technology was combined with health coaching.
The remaining studies investigated the role of wearable technology in exacerbation prediction. Al Rajeh et al.44 found that a continuous oxygen saturation and heart rate composite score had a positive predictive value of 91.7% of exacerbation detection. Hawthorne et al.46 found significant changes in both heart rate and respiratory rate three days prior to an exacerbation but no changes detected in physical activity or skin temperature. Wu et al.49 conducted a telehealth study incorporating a wearable alongside a health application and home air quality device and algorithms combing these inputs could predict early detection of COPD exacerbations (sensitivity 94% and specificity 90.4%). Finally, Cooper et al.45 combined wearables with daily spirometry, however, due to a high attrition rate no data analysis was conducted.
Study quality
The quality of the studies, as assessed by the Cochrane risk-of-bias tool50 can be seen in Supplementary Figure 6. Several studies had concerns in the domain looking at deviations from the intended interventions due to the per-protocol analysis employed, and the high drop-out rate in a large number of studies which would have affected the overall results. Studies had a low risk of bias in most of the other domains. The seven observational studies were of good quality and their Newcastle Ottawa Scale51 ratings can be seen in Supplementary Fig. 7.
Discussion
This systematic review and meta-analysis, has shown: (1) wearable technology interventions significantly improved the mean daily step count in COPD patients over a median duration of 3 months, with an average effect size of 0.42, equating to a clinically important difference of 850 (494–1205) steps/day, [minimal important difference (MID) 600–1100 steps/day52]; (2) wearable technology significantly increased the 6MWD with a mean difference (95%CI) of 5.81 m (1.02–10.61 m), however, this was below the MID of 25 m53; (3) wearable technology significantly decreased the CAT score (mean difference −0.99 (−1.59 to −0.40)) but this did not reach the MID of −2 points54; (4) wearable technology may support COPD exacerbation detection, however, studies were heterogenous with mixed outcomes and had a high attrition rate, suggesting further work in this field is necessary to draw firm conclusions; (5) wearable technology had no significant impact on other activity or quality of life metrics.
To our knowledge, this is the largest and most up-to-date review investigating the effect of wearable technology interventions on physical activity and exercise capacity in a COPD population. The overall increase in mean daily step counts falls within the MID range and is higher than 600 steps/day, which has previously been shown to reduce the risk of hospitalisation in the COPD population52. Moreover, it is probable that wearable technology interventions have a larger positive impact on physical activity than exercise training programs, long-term oxygen therapy or neuromuscular stimulation55,56. It is worth noting that the studies were heterogenous (due to different intervention designs and wearable technology devices), and this could not be explained during multivariable meta-regression analysis, suggesting that findings need to be interpreted with caution. While our findings echo previous reviews8,9,10,11, key points of differences lies in our subgroup analyses: firstly, isolated pedometer use (with feedback and goal setting) has no significant difference to usual care (MD 243 (−314–801) steps/day) and prior reviews have not made this distinction; secondly, studies combining wearable technology with health coaching (e.g., motivational interviewing and counselling) had the largest mean difference of 998 steps/day (539–1456); thirdly, wearable technology in addition to pulmonary rehabilitation compared to pulmonary rehabilitation alone also had a significant improvement in mean daily step count (MD 723 (191–1255) steps/day). These results suggest, wearable technology interventions that include another facet (such as health coaching or pulmonary rehabilitation) are more likely to have a greater benefit to patients, then just giving patients a step-counter to use, even if goals are prescribed. Patients who have ongoing encouragement through telephone calls, counselling and motivational interviewing have a higher success rate and increased improvement.
Subgroup analysis also found that the increase in mean daily step count was lower in studies of greater than 3 months duration this increase in mean daily step count was lower in studies of more than 3months duration, in the severe COPD population and if an accelerometer was use for outcome measurement (Fig. 6). The latter may be explained by the fact that accelerometers are validated tools to measure step count in COPD patients, meaning pedometers may overestimate the true effect57.

Squares represent mean daily step count with error bars representing confidence interval. The dotted horizontal line represents the minimum clinically important difference (600 steps/day). The type of intervention is compared to usual care or pulmonary rehabilitation (PR).
While our study found no change in the time spent in MVPA, a recent international task force has suggested that the mean steps/day metric, irrespective of intensity, can be used as an overall surrogate for physical activity58. However, it should be noted that previous studies have also found that even a minimal increase in activity intensity (from very low to low), reduces the risk of COPD admissions and all-cause mortality59. Therefore, future wearable devices that incorporate and encourage changes in both overall activity and intensity are likely to be more beneficial in this population.
Our meta-analysis also showed an improvement in the 6MWD by 5.81 m (1.02–10.61 m), similar to previously published data by Qui et al.8,who found a change of 11.6 m. Both these values fall short of the MID of 25m53 but are higher than the change associated with telehealth interventions (1.3 m)60. Moreover, even a 6 m increase in 6MWD is associated with around a 4% risk reduction in all-cause and respiratory mortality in the COPD population61. Subgroup analysis showed that wearable technology combined with health coaching had a greater improvement with a mean difference of 11.75 m (3.93–19.56). This once again shows that multi-component interventions that include wearable technology are better that isolated devices.
This is the first review to our knowledge that has analysed the impact of wearables on quality-of-life measures in patients with COPD. Over a median duration of 3 months, wearables were associated with a significant reduction in CAT score by −0.99 points, below the MID of −2 points54 and thus unlikely to be clinically relevant, although it is worth noting a certain proportion of participants in these trials will have achieved the MID. While no study performed a responder analysis, a dedicated study investigating the association of wearable technology and CAT score may be useful. No improvement in any other quality-of-life measures were found. Similar findings were concluded from a recent umbrella review of five systematic reviews looking at the impact of activity trackers on psychosocial outcomes and quality of life in healthy participants and those with rheumatological and connective tissue disorders62. This may be because quality of life measures rarely consider participants’ perspectives or views of the actual activity. Two studies15,16 in this review incorporated the PROactive Physical Activity in COPD instrument (C-PPAC)63 which assesses patients’ experience of the amount of physical activity and the difficulty experienced with physical activity. Higher scores mean a better experience of the activity and less difficulty. Meta-analysis of these two studies showed wearable devices improved the difficulty score (i.e., patients had less difficulty with physical activity) and the total score. The difficulty dimension of the tool has a moderate-strong correlation with health status, chronic dyspnoea and exercise capacity63. These results need to be interpreted with some caution given only two recent studies have used this instrument. It is probable that quality of life is a key motivator for physical activity. Therefore, if wearables of the future can improve both quality of life while improving physical activity, it is more likely that patients will continue to use the devices and gain benefit in the longer term.
In this review five studies15,32,33,47,48 examined the association between use of physical activity monitors and the rate of exacerbations. A meta-analysis of four of these studies showed no significant difference with a pooled OR 1.06 (0.90–1.24), however, this should be interpreted with some caution as one study47 (n = 2707) was significantly larger than the others, and all studies used multi-component strategies, thus isolating the role of the wearable is difficult. It is also worth noting, that the primary aim of all the studies was to improve physical activity to decrease exacerbation risk, rather than using wearables to support detection of exacerbations.
Three studies44,45,49 used composite scores to predict exacerbation onset. Two of these studies44,49 showed high positive predictive values in exacerbation detection. While this is encouraging, some caution must be exercised. Al-Rajeh et al.44 had a high attrition rate and included only 13 patients in their final analysis, while Wu et al.49 incorporated a system combining environmental measures which can be quite costly and cumbersome to replicate in the non-research setting. However, it is probable that continuous monitoring of physiological parameters holds promise for exacerbation prediction, and future studies are needed to investigate wearables for this purpose.
Some limitations to our review should be noted. Firstly, the studies were heterogenous and used different objective outcomes and devices. This means that direct comparison between studies may be limited, however, the random effects model used in the meta-analysis and reporting standardised mean differences should reduce the bias attributed to this. Secondly, studies using pedometers differed in their approach to setting an individualised target step count. Thirdly wearables were often combined with other health interventions, such as motivational interviewing and walking programs, meaning the exact impact of the wearable device may be under or over-estimated. To account for this, we have performed a detailed subgroup analysis. Finally, many studies had a high drop-out rate which was not appropriately accounted for in the analysis. This led to attrition bias in most of the studies which will invariably impact the outcomes.
In conclusion, this systematic review and meta-analysis suggests that wearable device interventions significantly improve the mean daily step count and exercise capacity as measured by the 6MWD but does not impact activity intensity. The greatest benefit seems to be from multi-component interventions that include wearable technology and other facets, such as health coaching or pulmonary rehabilitation. Wearables have a limited impact on patient quality of life, and the gains seen in physical activity and exercise capacity are likely to be short-lived. Future work needs to focus on the positive reinforcement of wearable technology to simultaneously improve long term physical activity as well as quality of life measures. While the data is limited, wearables are likely to support the detection of COPD exacerbation, but further work in this field is required. The main findings from this review are highlighted Fig. 7. Overall, wearable technology has part of a multi-component intervention strategy seems to have the potential to become a core part of future COPD management and improve health outcomes, but further work is required for this to become a reality.

Summary infographic.
Methods
Search strategy and selection criteria
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting in Systematic Reviews and Meta-Analysis (PRISMA) guidelines and was prospectively registered on PROSPERO (registration number: CRD42022299706).
We included any article that investigated the use of wearable technology with or without other components in an adult COPD population with the following outcomes of interest: physical activity promotion, exercise capacity, exacerbation detection, smoking cessation, home self-management, disease progression and quality of life. The diagnosis of COPD had to be made with an adequate exposure history and post-bronchodilator spirometry showing either a forced expiratory volume in 1 s: forced vital capacity (FEV1:FVC) < 0.7 or <lower limit of normal (gold standard)1. Wearable technology was defined as any device that was worn/fitted to the subject’s body externally, which detected and collected data. The device needed a means to retrieve the data for analysis64. We excluded studies that were not in English, used other methods of COPD diagnosis, narrative reviews, non-research letters, abstracts, case reports, conference proceedings, theses, books, other systematic reviews (but searched the reference list), and studies looking at implantable or in-hospital wearables.
Following a scoping search in Google Scholar to identify relevant search terms, we did a systematic literature search of five database from inception to April 2023: MEDLINE (via OVID); EMBASE (via OVID); the Cumulative Index to the Nursing and Allied Literature (CINAHL, EBSCO host); Cochrane Central Register for Controlled Trials (CENTRAL); and the Institute of Electrical and Electronics Engineers (IEEE) Xplore digital library. We used an extensive search strategy under the supervision of an experienced health sciences librarian which included terms relating to COPD and wearable technology. Search strings used for MEDLINE (via OVID) can be seen in Supplementary Methods. We also conducted a full literature reference search of prior systematic reviews. The studies from the five databases were uploaded onto Endnote software and duplicates removed. Following this, the bibliographic data were loaded onto Rayyan65 for blind screening by two independent reviewers.
Data analysis
Firstly, two authors (A.J.S., M.A.) independently screened titles and abstracts of studies against the inclusion criteria in a blinded fashion. Potentially eligible articles moved onto the next stage. Second, authors A.J.S. and M.A. independently assessed full texts of the potentially eligible articles for inclusion in the review. Third A.J.S. and M.A. developed a data extraction table including the year and country of publication, study settings, sample size and population, study duration patient demographics, intervention details, control group details, outcome data and attrition rates. A.J.S. and M.A. independently extracted data from each included article. Disagreements at each stage were resolved by discussion with S.M. The methodological quality of included studies was evaluated independently by A.J.S. and M.A. using the Cochrane risk of bias tool50 for randomised controlled trials and the Newcastle-Ottawa Scale (NOS) for observational studies51. Disagreements were resolved by SM. We attempted to contact study authors for unclear or missing information.
Physical activity and exercise capacity measurements were only included in the meta-analysis if they used an objective measurement tool (e.g., a pedometer/accelerometer). Subjective outcome measurements were not included in the meta-analysis.
Where meta-analysis was not possible due to significant heterogeneity, we undertook a narrative synthesis describing the included studies and their risk of bias.
Mean change scores with the corresponding standard deviation (SD) for the outcomes of interest were used in the meta-analysis to obtain the overall effect size, which was presented as either the mean difference or the standardised mean difference (SMD) with a 95% confidence interval. SMD was used where the same outcome of interest was measured by different devices. Where studies had not given the mean change scores, the mean change was calculated by subtracting the post-intervention mean from the baseline mean measure. The SD for changes from baseline was calculated using an imputed correlation coefficient of 0.80 with the following formula, derived from the Cochrane handbook (Eq. (1))66:.
Heterogeneity was assessed by I2, with a value of ≥50% indicative of significant heterogeneity. If the data were heterogenous, a random-effects model was used rather than a fixed model. All statistical analysis was performed using the Cochrane Collaboration Review Manager software (version 5.4).
To understand the source of heterogeneity between studies, meta-regression analysis was performed on the mean daily step count pooled effect. Five covariates were included: age, publication year, FEV1% predicted, type of wearable used as part of the intervention, and the outcome measurement device. We conducted a mixed-effects meta-regression using Rstudio version 4.2.3. The regression analysis used a Knapp-Hartung modification and model fit was assessed by the Bayesian information criterion.
Data availability
A.J.S. and S.M. have full access to all of the data in the study and take responsibility for the data integrity and accuracy of the analysis. Data are Excevailable from the corresponding author upon reasonable request.
References
GOLD. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary disease. (Global Initiative for Chronic Obstructive Lung Disease, 2023).
WHO. Chronic Obstructive Pulmonary Disease (COPD). (World Health Organisation 2021).
Cavaillès, A. et al. Comorbidities of COPD. Eur. Resp. Rev. 22, 454–475 (2013).
Rabe, K. F., Hurst, J. R. & Suissa, S. Cardiovascular disease and COPD: dangerous liaisons. Eur. Resp. Rev. 27, 180057 (2018).
Ferreira, J. J. M., Fernandes, C. I., Rammal, H. G. & Veiga, P. M. Wearable technology and consumer interaction: a systematic review and research agenda. Comput. Hum. Behav. 118, 106710 (2021).
Insights, F. B. Wearable Medical Devices Market Size, Share & COVID-19 Impact Analysis. 133 (Fortune Business Insight, Fortune Business Insight, 2020).
Spulber, I. et al. Implantable & Wearable Medical Devices for Chronic Obstructive Pulmonary Disease. (National Institute for Health and Care Research, 2019).
Qiu, S. et al. Using step counters to promote physical activity and exercise capacity in patients with chronic obstructive pulmonary disease: a meta-analysis. Ther. Adv. Respir. Dis. 12, 1753466618787386 (2018).
Armstrong, M. et al. Use of pedometers as a tool to promote daily physical activity levels in patients with COPD: a systematic review and meta-analysis. Eur. Respir. Rev. 28 (2019). https://doi.org/10.1183/16000617.0039-2019
Han, X. et al. An Exploration of the application of step counter-based physical activity promotion programs in patients with chronic obstructive pulmonary disease: a systematic review. Front Public Health 9, 691554 (2021).
Reilly, C. et al. Physical activity promotion interventions in chronic airways disease: a systematic review and meta-analysis. Eur. Resp. Rev. 32, 31 (2023).
Al Rajeh, A. M. & Hurst, J. R. Monitoring of physiological parameters to predict exacerbations of chronic obstructive pulmonary disease (COPD): a systematic review. J. Clin. Med. 5, 108 (2016).
Altenburg, W. A. et al. Short- and long-term effects of a physical activity counselling programme in COPD: a randomized controlled trial. Respir. Med. 109, 112–121 (2015).
Arbillaga-Etxarri, A. et al. Long-term efficacy and effectiveness of a behavioural and community-based exercise intervention (Urban Training) to increase physical activity in patients with COPD: a randomised controlled trial. Eur. Respir. J. 52 (2018). https://doi.org/10.1183/13993003.00063-2018
Armstrong, M. et al. Behavioural modification interventions alongside pulmonary rehabilitation improve COPD patients’ experiences of physical activity. Respir. Med. 180, 106353 (2021).
Bentley, C. L. et al. The use of a smartphone app and an activity tracker to promote physical activity in the management of chronic obstructive pulmonary disease: randomized controlled feasibility study. JMIR Mhealth Uhealth 8, e16203 (2020).
Benzo, R. P. et al. Feasibility of a health coaching and home-based rehabilitation intervention with remote monitoring for COPD. Respir. Care 66, 960–971 (2021).
Chen, Y. H., Chen, L. R., Tsao, C. C., Chen, Y. C. & Huang, C. C. Effects of a pedometer-based walking program in patients with COPD-A pilot study. Medicina (Kaunas) 58 (2022). https://doi.org/10.3390/medicina58040490
Cruz, J., Brooks, D. & Marques, A. Impact of feedback on physical activity levels of individuals with chronic obstructive pulmonary disease during pulmonary rehabilitation: a feasibility study. Chron. Respir. Dis. 11, 191–198 (2014).
de Blok, B. M. et al. The effects of a lifestyle physical activity counseling program with feedback of a pedometer during pulmonary rehabilitation in patients with COPD: a pilot study. Patient Educ. Couns. 61, 48–55 (2006).
Demeyer, H. et al. Physical activity is increased by a 12-week semiautomated telecoaching programme in patients with COPD: a multicentre randomised controlled trial. Thorax 72, 415–423 (2017).
Geidl, W. et al. Long-term benefits of adding a pedometer to pulmonary rehabilitation for COPD: the randomized controlled STAR Trial. Int J. Chron. Obstruct Pulmon Dis. 16, 1977–1988 (2021).
Hornikx, M., Demeyer, H., Camillo, C. A., Janssens, W. & Troosters, T. The effects of a physical activity counseling program after an exacerbation in patients with Chronic Obstructive Pulmonary Disease: a randomized controlled pilot study. BMC Pulm. Med 15, 136 (2015).
Hospes, G., Bossenbroek, L., Ten Hacken, N. H., van Hengel, P. & de Greef, M. H. Enhancement of daily physical activity increases physical fitness of outclinic COPD patients: results of an exercise counseling program. Patient Educ. Couns. 75, 274–278 (2009).
Kato, D. et al. Short-term and long-term effects of a self-managed physical activity program using a pedometer for chronic respiratory disease: a randomized controlled trial. J. Phys. Ther. Sci. 29, 807–812 (2017).
Kawagoshi, A. et al. Effects of low-intensity exercise and home-based pulmonary rehabilitation with pedometer feedback on physical activity in elderly patients with chronic obstructive pulmonary disease. Respir. Med. 109, 364–371 (2015).
Kohlbrenner, D., Sievi, N. A., Senn, O., Kohler, M. & Clarenbach, C. F. Long-term effects of pedometer-based physical activity coaching in severe COPD: a randomized controlled trial. Int J. Chron. Obstruct Pulmon Dis. 15, 2837–2846 (2020).
Mendoza, L. et al. Pedometers to enhance physical activity in COPD: a randomised controlled trial. Eur. Respir. J. 45, 347–354 (2015).
Moy, M. L., Weston, N. A., Wilson, E. J., Hess, M. L. & Richardson, C. R. A pilot study of an Internet walking program and pedometer in COPD. Respir. Med. 106, 1342–1350 (2012).
Nguyen, H. Q., Gill, D. P., Wolpin, S., Steele, B. G. & Benditt, J. O. Pilot study of a cell phone-based exercise persistence intervention post-rehabilitation for COPD. Int J. Chron. Obstruct Pulmon Dis. 4, 301–313 (2009).
Nolan, C. M. et al. Pedometer step count targets during pulmonary rehabilitation in chronic obstructive pulmonary disease. A randomized controlled trial. Am. J. Respir. Crit. Care Med. 195, 1344–1352 (2017).
Park, S. K., Bang, C. H. & Lee, S. H. Evaluating the effect of a smartphone app-based self-management program for people with COPD: a randomized controlled trial. Appl. Nurs. Res. 52, 151231 (2020).
Robinson, S. A. et al. A randomised trial of a web-based physical activity self-management intervention in COPD. ERJ Open Res. 7, 00158–02021 (2021).
Sasaki, S. et al. Effects of individualized target setting on step count in Japanese patients with chronic obstructive pulmonary disease: a pilot study. Adv. Respir. Med. (2021). https://doi.org/10.5603/ARM.a2021.0080
Spielmanns, M. et al. Using a smartphone application maintains physical activity following pulmonary rehabilitation in patients with COPD: a randomised controlled trial. Thorax 78, 442–450 (2023).
Valeiro, B. et al. Promotion of physical activity after hospitalization for COPD exacerbation: a randomized control trial. Respirology 28, 357–365 (2023).
Varas, A. B. et al. Effectiveness of a community-based exercise training programme to increase physical activity level in patients with chronic obstructive pulmonary disease: a randomized controlled trial. Physiother. Res. Int. 23, e1740 (2018).
Vorrink, S. N., Kort, H. S., Troosters, T., Zanen, P. & Lammers, J. J. Efficacy of an mHealth intervention to stimulate physical activity in COPD patients after pulmonary rehabilitation. Eur. Respir. J. 48, 1019–1029 (2016).
Wan, E. S. et al. Promoting physical activity in COPD: Insights from a randomized trial of a web-based intervention and pedometer use. Respir. Med 130, 102–110 (2017).
Widyastuti, K. et al. Benefits and costs of home pedometer assisted physical activity in patients with COPD. A preliminary randomized controlled trial. Pulmonology 24, 211–218 (2018).
Wootton, S. L. et al. Effects of ongoing feedback during a 12-month maintenance walking program on daily physical activity in people with COPD. Lung 197, 315–319 (2019).
Wootton, S. L. et al. Effect on health-related quality of life of ongoing feedback during a 12-month maintenance walking programme in patients with COPD: a randomized controlled trial. Respirology 23, 60–67 (2018).
Al Rajeh, A. et al. Application of oxygen saturation variability analysis for the detection of exacerbation in individuals with COPD: A proof-of-concept study. Physiol. Rep. 9, e15132–e15132 (2021).
Al Rajeh, A. M. et al. Once daily versus overnight and symptom versus physiological monitoring to detect exacerbations of chronic obstructive pulmonary disease: pilot randomized controlled trial. JMIR Mhealth Uhealth 8, e17597 (2020).
Cooper, C. B. et al. Statistical process control improves the feasibility of remote physiological monitoring in patients with chronic obstructive pulmonary disease. Int J. Chron. Obstruct Pulmon Dis. 14, 2485–2496 (2019).
Hawthorne, G. et al. A proof of concept for continuous, non-invasive, free-living vital signs monitoring to predict readmission following an acute exacerbation of COPD: a prospective cohort study. Respir. Res. 23, 102 (2022).
Nguyen, H. Q. et al. Effect of physical activity coaching on acute care and survival among patients with chronic obstructive pulmonary disease: a pragmatic randomized clinical trial. JAMA Netw. Open 2, e199657 (2019).
Wan, E. S. et al. Long-term effects of web-based pedometer-mediated intervention on COPD exacerbations. Respir. Med. 162, 105878 (2020).
Wu, C.-T. et al. Acute exacerbation of a chronic obstructive pulmonary disease prediction system using wearable device data, machine learning, and deep learning: development and cohort study. JMIR Mhealth Uhealth 9, e22591–e22591 (2021).
Sterne, J. A. C. et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 366, l4898 (2019).
Wells, G. A. et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. (2014). https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
Demeyer, H. et al. The minimal important difference in physical activity in patients with COPD. PLoS ONE 11, e0154587 (2016).
Holland, A. E. et al. Updating the minimal important difference for six-minute walk distance in patients with chronic obstructive pulmonary disease. Arch. Phys. Med Rehabil. 91, 221–225 (2010).
Kon, S. S. et al. Minimum clinically important difference for the COPD Assessment Test: a prospective analysis. Lancet Respir. Med 2, 195–203 (2014).
Lahham, A., McDonald, C. F. & Holland, A. E. Exercise training alone or with the addition of activity counseling improves physical activity levels in COPD: a systematic review and meta-analysis of randomized controlled trials. Int. J. Chronic Obstr. Pulm. Dis. 11, 3121–3136 (2016).
Mantoani, L. C., Rubio, N., McKinstry, B., MacNee, W. & Rabinovich, R. A. Interventions to modify physical activity in patients with COPD: a systematic review. Eur. Respir. J. 48, 69–81 (2016).
Van Remoortel, H. et al. Validity of six activity monitors in chronic obstructive pulmonary disease: a comparison with indirect calorimetry. PLoS ONE 7, e39198 (2012).
Demeyer, H. et al. Objectively measured physical activity in patients with COPD: recommendations from an international task force on physical activity. Chronic Obstr. Pulm. Dis. 8, 528–550 (2021).
Garcia-Aymerich, J., Lange, P., Benet, M., Schnohr, P. & Antó, J. M. Regular physical activity reduces hospital admission and mortality in chronic obstructive pulmonary disease: a population based cohort study. Thorax 61, 772–778 (2006).
Lundell, S., Holmner, Å., Rehn, B., Nyberg, A. & Wadell, K. Telehealthcare in COPD: a systematic review and meta-analysis on physical outcomes and dyspnea. Respiratory Med. 109, 11–26 (2015).
Casanova, C. et al. Distance and oxygen desaturation during the 6-min walk test as predictors of long-term mortality in patients with COPD. Chest 134, 746–752 (2008).
Ferguson, T. et al. Effectiveness of wearable activity trackers to increase physical activity and improve health: a systematic review of systematic reviews and meta-analyses. Lancet Digit Health 4, e615–e626 (2022).
Gimeno-Santos, E. et al. The PROactive instruments to measure physical activity in patients with chronic obstructive pulmonary disease. Eur. Resp. J. 46, 988–1000 (2015).
Fernández-Caramés, T. M. & Fraga-Lamas, P. Towards the internet of smart clothing: a review on IoT wearables and garments for creating intelligent connected E-textiles. Electronics 7, 405 (2018).
Ouzzani, M., Hammady, H., Fedorowicz, Z. & Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 5, 210 (2016).
Collaboration, T. C. (ed Julian P T and Green Sally Higgins) (Cochrane, 2011).
Acknowledgements
Not applicable
Author information
Authors and Affiliations
Contributions
A.J.S., S.M., J.R.H. were involved in study conceptualization and study design. A.J.S. and M.A.A. were involved in the literature search, article screening and assessment for eligibility and data extraction. S.M. acted as the third reviewer for any disagreements in this stage. A.J.S., M.A.A., A.S. were involved in data analysis. A.J.S. and C.E.O. performed the meta-analyses and meta-regression. A.J.S. prepared the first draft of the manuscript. M.A.A., A.S., J.R.H., and S.M. made substantial contributions to the interpretation of the data and all authors reviewed and revised the manuscript critically for important intellectual content. All authors gave final approval of the final version.
Corresponding author
Ethics declarations
Competing interests
A.J.S. and S.M. have received grants from Acurable Ltd. The payments have been made to their institutions. These grants are not linked to the current manuscript. J.R.H. has received support to attend meetings, personal payment and payment to his institution from pharmaceutical companies that make medicines to treat COPD. All other authors have no conflicts of interest to declare.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shah, A.J., Althobiani, M.A., Saigal, A. et al. Wearable technology interventions in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. npj Digit. Med. 6, 222 (2023). https://doi.org/10.1038/s41746-023-00962-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41746-023-00962-0
- Springer Nature Limited