
Abstract
Galectin-3 and Suppression of tumorigenicity-2 (ST2) are known markers of cardiac fibrosis. We investigated the prognostic value of fibrotic markers for the development of diastolic dysfunction and long-term outcome in patients suffering an ST-elevated myocardial infarction (STEMI). We analyzed 236 patients from the GIPS-III cohort with available echocardiographic studies and plasma measurements at hospitalization and after 4 months follow-up. Adjusted logistic mixed effects modelling revealed no association between the occurrence of diastolic dysfunction over time with abnormal plasma levels of galectin-3 and ST2. We observed no differences regarding survival outcome at follow-up of 5 years between patients with normal versus abnormal values in both galectin-3 (P = 0.75), and ST2 (P = 0.85). In conclusion, galectin-3 and sST2 were not associated with the development of diastolic dysfunction in non-diabetic patients that presented with a STEMI.
Similar content being viewed by others

Introduction
Over the past decades, innovations in standard care for patients suffering ST-elevated myocardial infarction (STEMI) have led to improved survival rates. Simultaneously, the incidence of comorbidities such as heart failure have increased in the aftermath of STEMI. A hallmark of heart failure is fibrosis which occurs both as reparative and reactive response to myocardial infarction1.
Galectin-3 and Suppression of tumorigenicity 2 (ST2) are known markers of cardiac fibrosis. ST2 is a member of the interleukin (IL)-1 receptor family. The primary cell source of ST2 has not yet been discovered, however there are several indications that vascular endothelial cells might be an important source of ST2. It is also suggested as a possible therapeutic target2. Soluble suppression of tumorigenicity (sST2) and the isoform transmembrane suppression of tumorigenicity (ST2L) are mostly studied in heart failure research3. ST2 is upregulated by cardiomyocytes and cardiac fibroblasts when mechanical stress is imposed, for instance stretch.
Galectin-3 is a beta-galactoside binding lectin that is produced by macrophages during myocardial stress and activates fibroblasts4. Galectin-3 consists of two domains, namely an atypical N-terminal domain and a C-terminal carbohydrate-recognition domain (CRD). During differentiation of monocytes into macrophages galectin-3 is released and engages in many processes during the acute inflammatory response such as neutrophil activation and chemoattraction of monocytes. Galectin-3 has been identified as a causal factor in the development of cardiac fibrosis5. Furthermore, galectin-3 is associated with outcome (mortality/heart failure rehospitalization) in different sub-set of patients (ischemic, non-ischemic) and in the general population6,7.
Both galectin-3 and sST2 are thought to be promising markers for risk stratification in heart failure patients. However, our knowledge of their prognostic value in a post-STEMI setting is limited. We previously reported that galectin-3, but not sST2, taken immediately after STEMI, predicts left ventricular ejection fraction (LVEF) and infarct size after 4 months8. The association of (change in) these fibrotic markers with (change in) diastolic function and long-term outcome after STEMI remains unknown. In this study we therefore aim to investigate the prognostic value of fibrotic markers for predicting diastolic dysfunction and long-term outcome in non-diabetic patients suffering a first STEMI.
Methods
This is a sub-study of the GIPS-III trial, a single center, randomized, double-blind, placebo-controlled study about the effect of metformin on LVEF. GIPS-III is registered as a clinical trial with identifier: NCT01217307. Design of this study, patient characteristics at hospitalization and primary outcomes have been reported previously9,10,11. Briefly, non-diabetic patients aged 18 years and over presenting to the University Medical Center Groningen with STEMI were randomized to metformin or placebo treatment after successful percutaneous coronary intervention (PCI) with implantation of at least 1 stent with a diameter of at least 3 mm were included. Important exclusion criteria were inability to undergo magnetic resonance imaging, previous myocardial infarction, and severe renal dysfunction. Metformin 500 mg twice daily or visually matching placebo twice daily was started immediately after PCI and lasted 4 months. All patients were contacted by phone at 5 years after STEMI to determine long term outcome. Patients provided verbal informed consent before PCI and written consent following admission to the Coronary Care Unit. The study protocol was approved by the local ethics committee of the University Medical Center Groningen (Groningen, the Netherlands), and was in accordance with the Declaration of Helsinki and Dutch laws.
Measurements of biomarkers
On hospital admission and 4 months after acute STEMI blood samples were obtained and anticoagulated with EDTA. These samples were spun down and plasma was stored at − 80 °C until further assaying. Galectin-3 levels were measured in the plasma samples with the FDA-cleared galectin-3 ELISA kit (BG Medicine, Waltham, MA). Intra- and inter-assay coefficient of variability of this assay is 3.2% and 5.6% respectively12. This assay has been described in greater detail previously13. sST2 was measured in the plasma samples with the FDA-cleared Presage® ST2 Assay (Critical Diagnostics, San Diego, CA). Intra- and inter-assay coefficient of variability of this assay is 5.1% and 5.2% respectively. Further characteristics of this assay have been published elsewhere14. FDA-cleared threshold values of 17.8 ng/mL for galectin-3 and 35.0 ng/mL for sST2 were used to categorize patients in groups of elevated versus non-elevated plasma levels. Delta biomarker levels were calculated as the 4-month level minus the hospitalization level and used to categorize patients in groups with decreased versus increased plasma levels. All other samples were measured in a routine setting. Creatinine (enzymatic), CK and CK-MB activity was measured on a Roche Modular P platform (Roche, Mannheim, Germany). NT-proBNP and Troponin T were measured on a Roche Modular E system (Roche, Mannheim, Germany). Troponin T was determined using either a fourth or a fifth-generation troponin assay.
Echocardiographic assessment
During hospitalization for the index event and at 4 months follow-up, trans-thoracic echocardiogram was performed in left decubital position using a Vivid 7 echo system (General Electric, Horton, Norway). All echocardiographic data were digitally stored in DICOM format and off-line analyses were performed on an Echopac BT 10 (General Electric, Horton, Norway) at an independent core lab (Groningen Imaging Core Laboratory, Groningen, the Netherlands). These analyses were performed by observers that were blinded to treatment allocation and all other patient data. Evaluation of the echocardiographic data was performed in accordance to the contemporary guidelines15,16,17. When appropriate, echocardiographic measures were indexed for body surface area (BSA) according to the formula of Du Bois and Du Bois18.
In concordance with the latest recommendations from the Heart Failure Association of the European Society of Cardiology for diagnosing heart failure with preserved ejection fraction19, the following measurements related to diastolic function were assessed: Left atrial volume (LAV) was measured with the area length method. The left ventricular mass was estimated from linear dimensions as suggested by Devereux and colleagues17. Left ventricular global longitudinal strain (GLS) assessments for the left ventricle were performed in the apical four-, three-, and two-chamber views using speckle-tracking. Doppler measurements were used for the mitral valve early filling flow (E). Using tissue color Doppler, early diastolic tissue velocities (e′) from both the septal and lateral wall were measured16,20. Mean e′ was calculated as (e′ septal + e′ lateral)/2. The ratio of trans mitral early flow to early mitral annulus velocity (E/e′) was calculated as E/mean e′. Reported values represent the mean of three heart beats in end-expiration.
Study outcomes
Diastolic dysfunction was defined as a multi-parametric dichotomous value based on the recommendations from the Heart Failure Association of the European Society of Cardiology for diagnosing heart failure with preserved ejection fraction (HFA-PEFF score)19. The HFA-PEFF score has functional, morphological, and biomarker domains. Within each domain, a major criterion is worth 2 points, and a minor criterion is worth 1 point (Supplementary Fig. 1). Major and minor criteria are not additive in a single domain and points are added only when they come from different domains. In our study a total score ≥ 5 points was considered to be diagnostic for diastolic dysfunction. A separate categorical value was composed to identify patients in whom diastolic function either improved, deteriorated, or remained unchanged between hospitalization and follow-up.
Additionally, the presence of abnormal individual values for echocardiographic measurements used to determine diastolic function were compared between groups with non-elevated versus elevated fibrotic markers. Abnormal values were defined based on clinically established cut off points19.
The fibrotic marker groups were formed based on the FDA appointed thresholds plasma levels for galectin-3 (> 17.8 ng/mL) and sST2 (> 35.0 ng/mL).
Major adverse cardiac events (MACE), defined as death, re-infarction, and target lesion revascularization, was the primary parameter for long term outcome.
Statistical analysis
Continuous variables are presented as mean ± standard deviation (SD) or median (interquartile range, IQR) for normally and non-normally distributed data, respectively. Categorical variables are presented as frequency (percentage). Non-normally distributed data was transformed using log-transformation. Outcome observations of median ± 5 times the standard deviation was considered extreme outliers and excluded from the cohort. Differences between groups were tested using two-tailed t test for normally distributed data and Wilcoxon rank-sum for non-normally distributed data. Reported P values are two-sided. Predictors of plasma levels for galectin-3 and sST2 at hospitalization were determined using regression models to determine relevant co-variates for subsequent analyses. If correlation between these predicting variables was present, the strongest predictor (greatest β-coefficient) was selected for further use.
We utilized logistic mixed model analysis to analyze the association of diastolic dysfunction over time with elevated plasma levels of galectin-3 and sST2 at hospitalization, 4 months follow-up, and categorical change between hospitalization and 4 months follow-up (improved, deteriorated, or unchanged), with random effects factor for each individual patient subject. These models were adjusted for variables that were significant predictors of galectin-3 and sST2 at hospitalization (leukocytes, estimated glomerular filtration rate, urea, total cholesterol, myocardial band of creatine kinase (CK-MB), lactate dehydrogenase (LDH), aspartate aminotransferase (ASAT), N-terminal pro–B-type natriuretic peptide (NT-proBNP), ischemic time, and TIMI flow grade post PCI < 3). Models were additionally adjusted for the GIPS-III treatment intervention variable (metformin use), and variables that are known to be associated with diastolic dysfunction (age, sex, and history of hypertension).
To reduce the chance of a type I error in this explorative biomarker study a P value of < 0.005 was considered to indicate a significant association or difference between groups, and a P value between 0.05 and 0.005 was considered suggestive in accordance with the position paper by Benjamin et al.21. When P > 0.10 only 2 decimal points are shown for clarity.
A multivariable Cox proportional hazard model for was constructed to test equality of survivor functions across groups with non-elevated versus elevated fibrotic markers. Analyses were performed using Stata version 18.0 (StataCorp), and R version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria).
Ethical approval
The study protocol was approved by the local ethics committee (Groningen, the Netherlands), and was in accordance with the Declaration of Helsinki and Dutch laws. Informed consent was obtained from all patients that were included in this study.
Results
Study population
All 379 patients participating in the GIPS-III trial were alive at 4 months. Echocardiographic assessment and plasma levels of fibrotic markers could be determined in 306 (81%) patients during hospitalization and 290 (77%) patients at 4 months. 238 (63%) patients with echocardiographic assessment and fibrotic markers at both time points were eligible for our study analyses. Of these, 2 (1%) patients were recognized as having extreme outliers and excluded from the cohort. 236 (62%) patients with reliable echocardiographic assessments and fibrotic markers remained eligible for the final analysis (Supplementary Fig. 2).
Mean age of the 236 included patients was 57.9 ± 11.4 years and 21.6% were females. The characteristics at hospitalization were compared between the patients with diastolic dysfunction and those without diastolic dysfunction (Table 1). Patients with diastolic dysfunction were significantly older (P < 0.001), were more likely to have a history of hypertension (P = 0.002) and had significantly higher plasma levels of NT-proBNP at index event (P < 0.001) as compared to those without diastolic dysfunction.
Diastolic dysfunction and fibrotic markers over time
At hospitalization, 39 (17%) patients had diastolic dysfunction, which increased significantly over time to 73 (31%) patients at 4 months (P < 0.001; Fig. 1).

Prevalence of diastolic dysfunction over time.
Plasma levels of the fibrotic biomarkers of patients with a first STEMI were relatively stable over time (Fig. 3). Median levels of galectin-3 at hospitalization were 13.2 (11.2–15.8) ng/mL and were comparable after 4 months (13.6 ng/mL (11.6–15.9); P = 0.050; Fig. 2A). The median change between hospitalization and 4 months follow up was 0.6 (− 1.3 to 2.7) ng/mL. Galectin-3 levels were elevated (≥ 17.8 ng/mL) in 33 (14.0%) patients at hospitalization and in 35 (14.8%) patients at follow-up. Elevated galectin-3 levels improved to normal in 15 (6.4%) patients, whereas normal levels of galectin-3 deteriorated to elevated levels in 17 (7.2%) patients.

Biomarker levels over time. Median levels of serum galectin-3 (A) and serum sST2 (B) after acute STEMI, at hospitalization and after 4 months, are shown. Whiskers represent interquartile ranges.
Median levels of sST2 at hospitalization were 30.1 (24.8–39.6) ng/mL and decreased numerically (P < 0.001) to 29.1 ng/mL (22.9–35.1) after 4 months (Fig. 2B). The median change between hospitalization and 4 months follow up was − 1.4 (− 7.3 to 2.9) ng/mL. sST2 levels were elevated (≥ 17.8 ng/mL) in 85 (36.0%) patients at hospitalization and in 60 (25.4%) patients at follow-up. Elevated sST2 levels improved to normal in 38 (16.1%) patients, whereas normal levels of sST2 deteriorated to elevated levels in 13 (5.5%) patients.
Elevated levels of galectin-3 and sST2 were not associated with individual echocardiographic parameters of diastolic dysfunction at either hospitalization or 4 months follow-up (Table 2).
Association between galectin-3 and sST2, and development of diastolic dysfunction
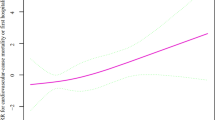
Adjusted logistic mixed effects modelling revealed no association between the occurrence of diastolic dysfunction over time with abnormal plasma levels of galectin-3 (Fig. 3) and sST2 (Fig. 4) at hospitalization, at 4 months, or with categorical change between hospitalization and 4 months follow-up.

Association of diastolic dysfunction over time with elevated plasma levels of galectin-3 at hospitalization (A), 4 months follow-up (B), and categorical change between hospitalization and 4 months follow-up (C).

Association of diastolic dysfunction over time with elevated plasma levels of sST2 at hospitalization (A), 4 months follow-up (B), and categorical change between hospitalization and 4 months follow-up (C).
Association of fibrotic markers with long term outcome
At 5-years follow-up, 20 (8%) patients had experienced a MACE event. A multivariable Cox proportional hazard model adjusting for variables associated with diastolic dysfunction, galectine-3, and sST2 revealed no differences regarding outcome between high and low groups in both galectin-3 (P = 0.75), and sST2 (P = 0.85; Supplementary Table 1).
Discussion
The present study suggests that galectin-3 and sST2 do not predict the development of diastolic dysfunction 4 months after STEMI. Additionally, both fibrotic markers did not predict MACE after 5 years in this patient cohort.
Diastolic dysfunction is increasingly recognized as a cause of symptomatic heart failure22. Diastolic dysfunction is associated with chronic hypertension, ischemic heart disease and degenerative processes. An underlying pathophysiology in each of these diseases is a dis-balance of adverse extra-cellular matrix accumulation and structural remodeling in the myocardium, referred to as cardiac fibrosis23.
In STEMI patients it could be speculated that a time-dependent damage to both myocytes and extracellular matrix (ECM) occurs in the infarct zone post myocardial infarction. Scar tissue will form at the place of injury that is characterized by fibrotic repair. The non-infarct zone exhibits reactive hypertrophy, interstitial fibrosis and increased collagen, potentially leading to cardiac dysfunction24,25,26. Fibrosis, the hallmark of this remodeling process could be a potential target for therapy. Identification of patients at risk for adverse remodeling and fibrosis which could lead to diastolic dysfunction would help clinicians to tailor therapy with anti-fibrotic agents27,28. Biomarkers that reflect myocardial damage, like cardiac troponin and creatine kinase can be used to estimate infarct size early after STEMI, but their sensitivity to detect other processes in cardiac remodeling is limited.
Galectin-3 and sST2 are emerging fibrotic biomarkers that are thought to be causally involved in the development of heart failure. However, galectin-3 is not cardiac specific, but is expressed in several fibrotic and inflammatory diseases29.
Elevated levels of sST2 have been associated with cardiac fibrosis, and its prognostic value is comparable to that of galectin-3 in heart failure patients. A previous study reported that ST2 correlated weakly with biomarkers of acute injury but was strongly associated with the risk of heart failure after myocardial infarction30.
In a previous post-hoc analyses of the same study we evaluated the association of both biomarkers with systolic function post-STEMI. We observed that patients with elevated galectin-3 levels at the time of acute MI have lower systolic function after 4 months. However, in the current study we did not find a similar association with diastolic function. We did find that plasma levels of the fibrotic biomarkers of patients with a first STEMI were relatively stable over time when comparing plasma levels at presentation with the plasma levels at 4 months follow-up. Similarly, a study on kinetics of selected serum markers of fibrosis in patients with dilated cardiomyopathy found that galectin-3 levels remained stable over 12 months regardless of diastolic dysfunction grade31. However, the pathophysiological chronology of dilated cardiomyopathy does not necessarily correspond to that of a STEMI. In murine models of post-myocardial infarction, galectin-3 rises directly after myocardial infarction both on tissue level and in the plasma level. However, it declines after a few days/weeks to nearly normal32. This corresponds with the timing of the scar formation. Exploring the predictive potential of maximum galectin-3 levels or the area under the curve of galectin-3 during the post-STEMI period warrants further investigation. A more detailed understanding of galectin-3 dynamics in post-STEMI patients may offer valuable insights into its clinical relevance.
Assessing diastolic dysfunction has proven to be much more difficult with definitions continuously being altered. It would be beneficial to know whether biomarkers could help us predict which patients are at risk to develop diastolic dysfunction after myocardial infarction. However, in this study, we could not identify patients that could be classified as at risk for the development of diastolic dysfunction by utilizing fibrotic markers alone. The latter could be due to the complexity of ventricular stiffness of the myocardium, which could not be represented by one single biomarker. A previous study in patients with hypertrophic cardiomyopathy showed that the combined parameters of NT-proBNP and maximum wall thickness had a better diagnostic performance for myocardial fibrosis assessed by late gadolinium enhancement on cardiovascular magnetic resonance imaging33. Moreover, ventricular stiffness is thought to be comprised of more than just interstitial fibrosis. Paulus et al. previously proposed a paradigm where a systemic proinflammatory state induced by comorbidities results in stiff cardiomyocytes and interstitial fibrosis. These alterations both contribute to a high diastolic left ventricular stiffness and heart failure development34. Additionally, diastolic dysfunction encompasses more than ventricular stiffness, reflecting the unique myocardial function of active relaxation35, which fibrotic markers may not fully capture. The diversity of underlying mechanisms and variables that influence diastolic dysfunction is further underlined by a recent study that identified a distinct profile of five microRNA’s that were significantly regulated in heart failure patients with preserved ejection fraction compared to healthy controls. These microRNA’s have previously been shown to be involved in the regulation of endothelial function and cellular ageing. The same study found that the SGLT2 inhibitor empagliflozin improves the regulation of two of these microRNA’s linked to endothelial function, indicating a possible reversibility36.
In this study we did not find evidence that biomarkers of fibrosis by themselves can predict the development of diastolic dysfunction after STEMI. However, results from a previous study show that fibrosis remains a promising target for therapy. Schimmel et al. identified two novel antifibrotic therapeutics based on naturally derived substance library screens for the treatment of cardiac fibrosis. These substances were shown to be effective antifibrotic molecules both in vitro and in vivo, leading to improvement in diastolic function in two hypertension-dependent rodent models of cardiac fibrosis37.
Galectin-3 and sST2 are recognized as independent predictors of adverse events and mortality in patients with heart failure38,39,40. However, our study did not reveal an association with long term outcome of MACE. One reason for this could be the fact that we have a low prevalence of symptomatic heart failure in our cohort. Additionally, while we maintained a substantial follow-up period of five years, the incidence of events was comparatively low. Consequently, our capacity to thoroughly investigate clinical outcomes is constrained by these factors.
Study limitations
A major strength of our study is that diastolic function was a predefined secondary endpoint in the prospective, randomized, placebo controlled GIPS-III trial. However, there are also some limitations in our study.
Echocardiographic assessment of diastolic dysfunction remains a continuing matter of debate and definitions differ between guidelines, and over time. Our study defined diastolic dysfunction based on the HFA-PEFF score which incorporates multiple criteria including tricuspid regurgitation peak velocity. Unfortunately, this parameter was not available in our dataset. As a results of this absent data our study is susceptible to non-differential misclassification bias. This bias may have led to individuals with diastolic dysfunction being misclassified as having a normal diastolic function, potentially attenuating associations with fibrosis related biomarkers. Based on the individual HFA-PEFF scores we were able to identify four (2%) patients with a potential for misclassification of diastolic dysfunction at hospitalization and 34 (14%) patients with a potential for misclassification of diastolic dysfunction at follow-up.
Roughly a third of the original cohort was excluded because echocardiography did not allow for diastolic measurements or because echocardiography was not performed. While we did not find evidence of a selection bias, we cannot exclude that an unknown patient selection based on presence of echocardiographic measurements has influenced our results.
Our study found no association between fibrosis related biomarkers and the development of diastolic dysfunction post-STEMI. However, these post-hoc analyses might be underpowered to detect small differences.
Conclusion
In summary, galectin-3 and sST2 were not associated with the development of diastolic dysfunction in non-diabetic patients that presented with a STEMI.
Data availability
The dataset analyzed during the current study is available from the corresponding author on reasonable request.
Abbreviations
- ST2:
-
Suppression of tumorigenicity
- sST2:
-
Soluble suppression of tumorigenicity
- ST2L:
-
Transmembrane suppression of tumorigenicity
- STEMI:
-
ST-elevated myocardial infarction
- MACE:
-
Major adverse cardiac events
- IL:
-
Interleukin
- ST2L:
-
Transmembrane suppression of tumorigenicity
- CRD:
-
C-terminal carbohydrate-recognition domain
- LVEF:
-
Left ventricular ejection fraction
- PCI:
-
Percutaneous coronary intervention
- BSA:
-
Body surface area
- LAV:
-
Left atrial volume
- GLS:
-
Left ventricular global longitudinal strain
- E:
-
Mitral valve early filling flow
- e′:
-
Early diastolic tissue velocity
- E/e′:
-
Ratio of transmitral early flow to early mitral annulus velocity
- SD:
-
Standard deviation
- IQR:
-
Interquartile range
- LVMI:
-
Left ventricular mass index
- TIMI:
-
Thrombolysis in myocardial infarction
- HbA1c:
-
Glycated hemoglobin
- NT-proBNP:
-
N-terminal pro brain natriuretic peptide
- LDH:
-
Lactate dehydrogenase
- eGFR:
-
Estimated glomerular filtration rate
- CK:
-
Creatine kinase
- CK–MB:
-
Creatine kinase–Myocardial band
- ASAT:
-
Aspartate aminotransferase
- LDL:
-
Low density lipoprotein
- HDL:
-
High density lipoprotein
References
Talman, V. & Ruskoaho, H. Cardiac fibrosis in myocardial infarction-from repair and remodeling to regeneration. Cell Tissue Res. 365, 563–581 (2016).
Kakkar, R. & Lee, R. T. The IL-33/ST2 pathway: Therapeutic target and novel biomarker. Nat. Rev. Drug Discov. 7, 827–840 (2008).
Weinberg, E. O. et al. Identification of serum soluble ST2 receptor as a novel heart failure biomarker. Circulation 107, 721–726 (2003).
Liu, F. T. et al. Expression and function of galectin-3, a β-galactoside-binding lectin, in human monocytes and macrophages. Am. J. Pathol. 147, 1016–1028 (1995).
Sharma, U. C. et al. Galectin-3 marks activated macrophages in failure-prone hypertrophied hearts and contributes to cardiac dysfunction. Circulation 110, 3121–3128 (2004).
Meijers, W. C. et al. Elevated plasma galectin-3 is associated with near-term rehospitalization in heart failure: A pooled analysis of 3 clinical trials. Am. Heart J. 167, 853 (2014).
de Boer, R. A. et al. The fibrosis marker galectin-3 and outcome in the general population. J. Intern. Med. 272, 55–64 (2012).
van der Velde, A. R. et al. Galectin-3 and sST2 in prediction of left ventricular ejection fraction after myocardial infarction. Clin. Chim. Acta. 452, 50–57 (2016).
Lexis, C. P. H. et al. Metformin in non-diabetic patients presenting with ST elevation myocardial infarction: Rationale and design of the glycometabolic intervention as adjunct to primary percutaneous intervention in ST elevation myocardial infarction (GIPS)-III trial. Cardiovasc. Drugs Ther. 26, 417–426 (2012).
Lexis, C. P. H. et al. Effect of metformin on left ventricular function after acute myocardial infarction in patients without diabetes: The GIPS-III randomized clinical trial. JAMA 311, 1526–1535 (2014).
Al Ali, L. et al. The effect of metformin on diastolic function in patients presenting with ST-elevation myocardial infarction. PLoS One 11, e0168340 (2016).
Meijers, W. C., Van Der Velde, A. R. & De Boer, R. A. The ARCHITECT galectin-3 assay: Comparison with other automated and manual assays for the measurement of circulating galectin-3 levels in heart failure. Expert Rev. Mol. Diagn. 14, 257–266 (2014).
Christenson, R. H. et al. Multi-center determination of galectin-3 assay performance characteristics: Anatomy of a novel assay for use in heart failure. Clin. Biochem. 43, 683–690 (2010).
Mueller, T. & Dieplinger, B. The Presage(®) ST2 Assay: Analytical considerations and clinical applications for a high-sensitivity assay for measurement of soluble ST2. Expert Rev. Mol. Diagn. 13, 13–30 (2013).
Nagueh, S. F. et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. Eur. J. Echocardiogr. 10, 165–193 (2009).
Lang, R. M. et al. Recommendations for chamber quantification. Eur. J. Echocardiogr. 7, 79–108 (2006).
Devereux, R. B. et al. Echocardiographic assessment of left ventricular hypertrophy: Comparison to necropsy findings. Am. J. Cardiol. 57, 450–458 (1986).
Du Bois, D. & Du Bois, E. F. A formula to estimate the approximate surface area if height and weight be known. Nutrition 5, 303–311 (1916) (Discussion 312–313 (1989)).
Pieske, B. et al. How to diagnose heart failure with preserved ejection fraction: the HFA-PEFF diagnostic algorithm: A consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur. Heart J. 40, 3297–3317 (2019).
Hummel, Y. M. et al. Diastolic function measurements and diagnostic consequences: A comparison of pulsed wave- and color-coded tissue Doppler imaging. Clin. Res. Cardiol. 99, 453–458 (2010).
Benjamin, D. J. et al. Redefine statistical significance. Nat. Hum. Behav. 2, 6–10 (2018).
Johnson, J. A. Diastolic dysfunction in congestive heart failure. N. Engl. J. Med. 325, 850–861 (1991).
Travers, J. G., Kamal, F. A., Robbins, J., Yutzey, K. E. & Blaxall, B. C. Cardiac fibrosis: The fibroblast awakens. Circ. Res. 118, 1021–1040 (2016).
Weisman, H. F., Bush, D. E., Mannisi, J. A. & Bulkley, B. H. Global cardiac remodeling after acute myocardial infarction: A study in the rat model. J. Am. Coll. Cardiol. 5, 1355–1362 (1985).
Manhenke, C. et al. The prognostic value of circulating markers of collagen turnover after acute myocardial infarction. Int. J. Cardiol. 150, 277–282 (2011).
Screever, E. M. et al. Diffuse myocardial fibrosis on cardiac magnetic resonance imaging is related to Galectin-3 and predicts outcome in heart failure. Biomolecules 13, 410 (2023).
Bender, S. B. et al. Mineralocorticoid receptor antagonism treats obesity-associated cardiac diastolic dysfunction. Hypertension 65, 1082–1088 (2015).
Cai, J. et al. Anti-fibrosis effect of relaxin and spironolactone combined on isoprenaline-induced myocardial fibrosis in rats via inhibition of Endothelial-Mesenchymal Transition. Cell. Physiol. Biochem. 41, 1167–1178 (2017).
Martinez-Martinez, E. et al. Galectin-3 blockade reduces renal fibrosis in two normotensive experimental models of renal damage. PLoS One 11, e0166272 (2016).
Kohli, P. et al. Role of ST2 in non-ST-elevation acute coronary syndrome in the MERLIN-TIMI 36 trial. Clin. Chem. 58, 257–266 (2012).
Wiśniowska-śmiałek, S. et al. Kinetics of selected serum markers of fibrosis in patients with dilated cardiomyopathy and different grades of diastolic dysfunction of the left ventricle. Cardiol. J. 27, 726 (2020).
Sharma, U. C. et al. Myocardial and serum Galectin-3 expression dynamics marks post-myocardial infarction cardiac remodelling. Heart Lung Circ. 26, 736–745 (2017).
Li, Y. et al. Predictive values of multiple non-invasive markers for myocardial fibrosis in hypertrophic cardiomyopathy patients with preserved ejection fraction. Sci. Rep. 11, 4297 (2021).
Paulus, W. J. & Tschöpe, C. A novel paradigm for heart failure with preserved ejection fraction: Comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J. Am. Coll. Cardiol. 62, 263–271 (2013).
Nagueh, S. F. et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: An update from the American Society of echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 17, 1321–1360 (2016).
Mone, P. et al. Empagliflozin improves the MicroRNA signature of endothelial dysfunction in patients with heart failure with preserved ejection fraction and diabetes. J. Pharmacol. Exp. Ther. 384, 116–122 (2023).
Schimmel, K. et al. Natural compound library screening identifies new molecules for the treatment of cardiac fibrosis and diastolic dysfunction. Circulation 141, 751–767 (2020).
Shi, Y. et al. Clinical implications of plasma Galectin-3 in heart failure with preserved ejection fraction: A meta-analysis. Front. Cardiovasc. Med. https://doi.org/10.3389/fcvm.2022.854501 (2022).
Dudek, M. et al. sST2 and Heart Failure—Clinical utility and prognosis. J. Clin. Med. 12, 3136 (2023).
Trippel, T. D. et al. The diagnostic and prognostic value of galectin-3 in patients at risk for heart failure with preserved ejection fraction: Results from the DIAST-CHF study. ESC Heart Fail. 8, 829–841 (2021).
Funding
The GIPS-III trial was supported by grant 95103007 from the Netherlands Organization for Health Research and Development (ZonMw), The Hague, the Netherlands.
Author information
Authors and Affiliations
Contributions
Conceptualization LAA, WCM, HEG, EL, DJvV, AAV, ICCvdH, RAdB, PvdH Methodology, analysis and/or software LAA, WCM, HEG, EL, DJvV, AAV, ICCvdH, RAdB, PvdH, IEB Resources EL, DJvV, AAV, ICCvdH, RAdB, PvdH Data curation LAA, WCM, HEG, EL, DJvV, AAV, ICCvdH, RAdB, PvdH Writing – Original Draft LAA, WCM, RAdB, PvdH Interpretation of data, review & editing LAA, WCM, HEG, EL, DJvV, AAV, ICCvdH, RAdB, PvdH, IEB Visualization LAA, WCM, HEG.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Al Ali, L., Meijers, W.C., Beldhuis, I.E. et al. Association of fibrotic markers with diastolic function after STEMI. Sci Rep 14, 19122 (2024). https://doi.org/10.1038/s41598-024-69926-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-69926-y
- Springer Nature Limited